After the installation of a titanium implant is completed, it is necessary that it be completely covered with bone tissue and mucous membrane: this ensures the conditions for its successful engraftment into the bone. But situations arise when the edge of the implant becomes visible due to bone and gum deficiency. Such defects are eliminated by performing bone grafting and gingivoplasty - operations to increase the volume of tissue around the implant.
In order not to trigger a pathology that significantly impairs aesthetics, it is important to notice the initial manifestations of this complication in time.
Dental implant failure: peri-implantitis and mucositis
Today, implant rejection officially occurs in 2 to 5% of patients. And this process can begin either immediately or after several years of active use of the teeth. The main reason is considered to be the accumulation of pathogenic microflora, which leads to inflammation of the tissues around the installed implants. But there are two possible developments of the situation.
Peri-implantitis is a full-fledged and very severe inflammatory process that affects tissue along the entire length of the installed implant and leads to resorption (resorption) of the jaw bone. With this pathology, it is most often necessary to remove the structures in order to completely stop the development of inflammation. In any case, the doctor will diagnose and assess the condition; the more bone is preserved around the implant, the greater the chance of successful therapeutic treatment without extracting the titanium root.
But there is also such a thing as mucositis - in this case, the inflammation is localized only in the gum area, that is, it does not lead to the destruction of bone tissue around the implant body, and there is almost a 100 percent chance of saving the structure. For this purpose, drug therapy is carried out.
“Every patient must understand that the outcome of treatment is not only the responsibility of the attending physician. At the first stage - yes, the first 50% depends on the professionalism of the implantologist, on how he plans the treatment process and installs the implants. But the second 50% of success is the task of the patient himself: implants, just like living teeth, require careful care.”
Bespalov Roman Dmitrievich, maxillofacial surgeon, implantologist, more than 25 years of experience make an appointment
Implantation without risks and complications! Our doctors are professionals who are trained in the best foreign centers. We do not save on the health of our patients!
Enroll now
Symptoms of mucositis and peri-implantitis
With mucositis - superficial inflammation of the tissue - there is slight swelling, redness or even blue discoloration of the gums.
The mucosa may move slightly away from the crown or implant abutment. If you look at the picture, there is no bone inflammation and no bone loss. With peri-implantitis, the symptoms are more pronounced:
- redness and swelling of the gums,
- pain when pressing on the implant and its mobility,
- purulent discharge, bleeding from the area of the installed implant,
- increase in body temperature to 38 degrees.
Even with slight inflammation of the gums in the area of installed implants, you should promptly consult a doctor - the sooner a diagnosis is made and treatment is started, the greater the chance of saving the installed implant.
Stages and forms of peri-implantitis
- mild stage: loss of bone tissue around the implant is no more than 3 mm, while the mucous membrane becomes inflamed and minor pain occurs. Note that this is no longer mucositis, since bone resorption is observed. Treatment of this stage is usually conservative, with the use of antibiotics and painkillers,
- moderate stage: about half of the vertical bone tissue is lost, pus discharge appears from the area of the installed implant, bleeding and acute pain occur,
- severe stage: almost complete resorption of bone tissue, formation of deep pockets, development of infection, purulent discharge, constant bleeding.
How is diagnostics carried out?
If you find any of the listed symptoms, or the doctor himself has doubts during a routine examination, an x-ray diagnosis is required. This may be a panoramic image (OPTG), but better - a three-dimensional computed tomography, which will allow you to assess the degree of bone resorption around the entire body of the implant.
Also, the doctor must conduct a visual examination and instrumental diagnostics, or more precisely, probing. It is necessary to assess the depth of the gum pocket - normally the mucous membrane fits tightly and it is difficult to “get to” the implant itself, because it is immersed in bone tissue (if we are talking about a two-part structure). But with peri-implantitis, the gums easily peel off, and the depth of such a gum pocket can be from 5-6 mm or more.
Stages
- Easy . Minor loss of bone around the implant. Inflammation of the mucous membrane appears, the pain is not pronounced, and the artificial root wobbles slightly. Painkillers, antibiotics, and in some cases surgical treatment are prescribed.
- Average . Half of the vertical bone loss. Pus appears, bleeding, acute pain, the gums peel off, the implant is unstable. Surgical treatment or removal of the implant is prescribed.
- Heavy . Complete bone resorption. Deep gum pockets, spread of infection to neighboring areas, increased purulent discharge, prolonged bleeding. The implant will have to be removed.
It is considered normal to lose bone around the implant from one to one and a half millimeters in the first year and no more than 0.2 millimeters per year thereafter. Bone loss above these levels is pathological.
Why is peri-implantitis becoming more common? World Research Results
Due to the fact that peri-implantitis is diagnosed several times more often than 5 years ago, world implantologists are literally sounding the alarm - holding symposiums and meetings to discuss this growing problem. And they all agree that the main reason why peri-implantitis occurs is bacteria (how they get into the tissue around the implant is another matter, but this will be discussed later).
On traditional designs, which are designed for a two-stage protocol, a rough surface is provided along the entire length of the implants. This is done for their better fixation in the bone tissue - due to the presence of micropores, bone cells literally grow into the body of the implant. However, after installation of implants during the first five years1, bone resorption occurs up to 1-3 mm (this is considered a physiological norm, and manufacturers are trying to improve the design of implants to reduce this problem). As a result, the rough top of the implants becomes exposed. And if at the same time the lack of oral hygiene on the part of the patient is added to this, then a large amount of plaque accumulates on the implant. This is the main reason for the development of peri-implantitis and subsequent implant rejection.
According to studies conducted by the International Foundation of Implantologists, today it is customary to identify three main reasons for the development of peri-implantitis: the rough surface of implants in combination with poor hygiene and not entirely correct installation (above the gum level), the multicomponent nature of implants (when the connection between the implant body and the abutment is not tight, plaque accumulates ), as well as the wide diameter of the installed structures.
Naturally, we are not talking about all implants. But many manufacturers, unfortunately, do not take into account the high risks of developing peri-implantitis and produce models that significantly increase the likelihood of developing an inflammatory process. This means that their long-term service life is out of the question.
The main causes of the development of mucositis and peri-implantitis
So, as noted earlier, the main reason for the development of both mucositis and peri-implantitis is the accumulation of pathogenic microflora. In simple terms, like any inflammation, these problems are caused by ordinary microorganisms: mainly spirochetes and gram-negative anaerobes. These names will mean nothing to the average person; it is much more important to understand where they come from in the oral cavity and why they begin to be active.
In general, our oral cavity contains both “good” and pathogenic microorganisms. But their number is balanced. In the absence of daily oral hygiene, with a decrease in immunity (or if it fights other diseases), the number of “harmful” microbes prevails, which provokes the development of various inflammatory processes. With mucositis it is superficial, with peri-implantitis it is deeper. But if the cause of mucositis is mainly poor oral hygiene, then there are much more prerequisites for the development of peri-implantitis:
- doctor errors: insufficient examination of the patient; installation of implants only on the basis of a panoramic image without computed tomography; penetration of microbes (including saliva) into the cavity during implant installation; errors during prosthetics - for example, overloading of the implant or injury to the mucous membrane,
- violations on the part of the patient: failure to comply with hygiene rules; refusal to treat chronic diseases (in particular, HIV infection, diabetes mellitus); use of prostheses other than for their intended purpose.
Assessment and diagnosis of complications that have arisen
After the first symptoms are detected, professional diagnostic methods make it possible to reliably determine the cause and depth of the pathological process. For this purpose, radiography or computed tomography is used. They allow you to assess the condition of the bone tissue at the time when the implants fell out. A year after installation, the picture will be different than after one month of wearing implants. After diagnosis using these methods, the doctor gives his assessment and offers options for solving the problem.
What doctor mistakes lead to peri-implantitis?
At the first stage, when preparation for treatment and direct installation of implants is carried out, the positive outcome of implantation depends 90% on the doctor. After this, most of the responsibility passes to the shoulders of the patient himself.
- errors at the diagnostic stage: implantation only on the basis of OPTG (panoramic image) data without the use of three-dimensional computed tomography (CT); implantation without prior assessment of the patient’s health status,
- Chronic diseases are not excluded and are not taken into account, as well as certain conditions: pregnancy, menopause and menstruation in women, diabetes mellitus, active smoking and drinking alcohol, periodontitis and periodontal disease, ENT pathologies, poorly treated teeth in the oral cavity,
- errors at the treatment planning stage, for example, incorrectly chosen place for implants, too thin bone, too close to natural teeth,
- errors at the stage of implant installation: violation of sterility, damage to the coating of implants, saliva getting into the hole, use of non-original products, etc.,
- errors at the prosthetic stage: overloading of all or some of the implants in the complex, cement getting into the cavity, incorrect design of the prosthesis, restoration of only one jaw, etc.
Read more about all the mistakes that can be made during implantation in our separate material >>>
“The case of each patient in our clinic is reviewed by several doctors. This is necessarily a maxillofacial surgeon-implantologist, as well as an orthopedist. Already at the initial stage we evaluate every nuance, consider every detail. It is very important to us that the patient receives not only a beautiful smile, but also teeth that can be used to eat without pain.”
Chorny Stanislav Vladimirovich. orthopedic dentist, work experience over 19 years
Non-original components mean a risk of implant rejection! We use only original implants, abutments and other superstructures that are tightly connected without joints or micro-gaps. As a whole, they passed a quality test directly at the factory - the manufacturer guarantees that they will function fully for many years.
sign up now
Who is at risk and what depends on the patient
At the stage before surgery, it is very important for you, as a patient, to follow the doctor’s recommendations and also tell him about all your health problems. We understand that if you come to the clinic, you expect to undergo implantation and restore lost teeth. But this is an expensive and complex treatment - in order not to waste money and time, and also in order not to spoil your health, you need to be extremely honest with your doctor. Today the list of contraindications to implantation is very small - over the past two years in our clinic there have been less than 10 patients whom we had to refuse treatment.
Patients with the following problems are at risk for developing peri-implantitis:
- bruxism – teeth grinding and strong clenching of the jaws leads to overload of the implants,
- long-term treatment with corticosteroids leads to poor tissue regeneration, destruction of blood vessels, increased risk of bleeding,
- previous radiation or chemotherapy suppresses the immune system and the functioning of many organs and systems,
- diabetes mellitus or osteoporosis lead to metabolic disorders,
- Alcohol abuse (especially immediately after dental implantation) leads to an increased risk of bleeding, failure to heal wounds, and inflammation of the tissue around the implant. Read our material about why alcoholic beverages must be avoided after implantation,
- refusal of hygiene or its improper implementation - including the use of dental floss, which leads to injury to the gums and exposure of the tops of the implants.
All these conditions increase the risk of developing peri-implantitis, but are not independent factors in its occurrence. This group of patients requires a more thorough diagnosis. Often, “narrow” specialists are involved, for example, oncologists, endocrinologists, who will give their opinion on the person’s state of health or prescribe appropriate therapy. In such situations, not only the doctor must weigh the pros and cons, but the patient himself must understand the risks and possible complications. If a specialist is honest and professional, he will never undertake to work with a person whose health he will harm rather than improve.
How to care for your gums in the first days after implantation
It is very important to follow your doctor's recommendations, especially in the first time after surgery. This will determine how long the adaptive period will last and how unpleasant it will be.
To relieve swelling and relieve pain, do the following:
- In the first hours after implantation, apply ice to the cheek in the place where the new tooth was installed. To do this, place ice cubes in a plastic bag and apply it through a soft cloth to the skin. Keep it for about twenty minutes. Then rest for half an hour and apply again.
- Special adhesive balms ASEPTA will help reduce inflammation; they have an active antimicrobial effect, relieve inflammation and reduce bleeding of the gums. It is also recommended to use high-quality prophylactic pastes. All this will help you speed up tissue healing.
- It is better to sleep on a high pillow so that less blood flows to the new tooth, this will also help reduce swelling.
In the first week, eat warm food, exclude all cold and hot dishes from the menu. You should also avoid foods that are too hard or spicy. A good option for the first time is purees, yoghurts and soups.
On a note. Rinsing with homemade infusions of calendula and chamomile will help reduce swelling. You can also use preventative mouth rinses. But remember, rinsing cannot be done earlier than one day after surgery.
Help your body cope with inflammation, and your gums will soon return to normal and discomfort will disappear. If this is not observed by the sixth or seventh day, you should consult a specialist.
Be attentive to your sensations, observe the body’s reaction to a foreign object. If the swelling has not started to subside on the fourth day, see your dentist. It is necessary to understand whether this is normal or whether implant rejection or tissue infection has begun.
Also reasons to visit a surgeon will be:
- increasing hyperemia (increased blood flow) of the gums;
- formation of hematoma, blue discoloration of tissues;
- increasing pain after the first two to three days;
- bleeding and the appearance of pus near the operation site.
Risks of implant rejection in the postoperative period
After successful dental implantation and after the implants have fully fused with the bone (that is, after six months to a year), you still shouldn’t relax. It is important to maintain good oral hygiene and maintain your health. It is clear that no one is immune from developing any disease in the future, but if you have chronic problems, you need to ensure that they do not develop into an acute stage. For example, if you have diabetes, you need to follow a diet and take all medications prescribed by your doctor, and monitor your blood sugar levels.
Immediately after installation of the implants, it is necessary to strictly follow the doctor’s recommendations in terms of therapeutic treatment. If antibiotics have been prescribed, then you must take them for a strictly specified amount of time or at least ask your doctor if you can stop taking them.
If the prosthesis was installed immediately, then you can also eat right away. But the load should be moderate - you can’t go to a restaurant on the first day and eat a hard steak, snacking on nuts and drinking a glass of whiskey.
Read our useful article about how to behave after dental implantation >>>
After 1.5 years, Alexander went to the clinic to replace the adaptive prosthesis with a permanent one made of ceramic composite. During this time, he regularly underwent preventive examinations and paid attention to oral hygiene, so there were no complications after implantation.
View review
“It’s been a year since I lost my teeth. I am happy with everything! My situation was very difficult and serious; I had to remove eight teeth at once. Thanks to the doctors for returning me to normal life. I eat, chew normally, and smile!” – our patient shared his impressions.
View review
What we guarantee
- Correct implantation, strict adherence to protocols. Our Center has a team of highly qualified doctors, employees of Moscow medical universities. Implantologists are proficient in all known protocols, and constantly undergo internships and advanced training courses in the USA, Germany, and surgical centers in Russia.
- Installation of high-quality Nobel Biocare implants. They have no restrictions on installation, are suitable for all clinical cases, the survival rate is 99.3%, and are protected from counterfeiting. Patented TI-Unite surface promotes faster healing. We provide a lifetime warranty.
- Thorough diagnosis. The center is equipped with modern diagnostic equipment, the results will be known in 15 minutes.
- Quick response to problem . You can call us at any time of the day or any day of the week if something is bothering you. In addition, we conduct preventive examinations and free CT examinations after surgery.
How is the treatment carried out and is it possible to save the implant?
Treatment of moderate and severe peri-implantitis today, unfortunately, does not give the desired results2. According to an analysis of the literature carried out by Heitz-Mayfield and Mombelli3, in almost 93% of cases, the tissue around the implants becomes infected again after treatment. That is, the risk of relapse is very, very high. Therefore, often the only correct solution is to remove the implant and carry out subsequent drug therapy.
But treatment of mucositis is quite possible. As well as the treatment of peri-implantitis if the implant is immobile and only a small amount of bone tissue is lost. In any case, the final decision is made by the doctor after conducting appropriate diagnostics.
The treatment method is only surgical, but complex, therefore it consists of several areas:
- cleaning the surface of the exposed implant,
- therapy with antibacterial drugs,
- increasing the volume of bone around the implant, correcting the position of the gums,
- the use of membranes from the patient’s own blood plasma during the surgical stage of treatment,
- prosthesis correction.
“For patients with advanced periodontitis, we recommend basal implantation, since in this case smooth implants with an antibacterial coating are used. Due to this, their contact with the mucous membrane is allowed, and even in the presence of an inflammatory process, pathogenic microorganisms will not accumulate on their surface, so the risk of peri-implantitis is minimized.”
Namdakov Nikolay Vladimirovich, maxillofacial surgeon, implantologist, orthopedist with more than 17 years of experience make an appointment
Cleansing from granulations and inflamed tissues
The very first thing to do is to clean the surface of the exposed implant from contaminants, i.e.
inflamed tissues, granulations, plaque, bacterial plaques. The surface of two-piece implants is porous, so if it is open and located above the level of the bone and gum (after all, with peri-implantitis, the bone volume is reduced), the accumulation of pathogenic microflora is guaranteed. Cleansing is carried out using ultrasound, laser or Air Flow system. Finally, treatment with antiseptics. In fact, this is the initial preparation for the main surgical intervention. The main difficulty is that many implants have an active coating, which is achieved through complex multi-stage processing in the factory. And when washing the surface of the implant, it can be damaged, which can lead to poor implantation of the structure or even complete rejection. This is also one of the reasons why treatment of peri-implantitis sometimes does not give positive results.
Antibacterial therapy
In the presence of peri-implantitis, antibiotics must be prescribed to relieve the inflammatory process. These can be general medications, but in a number of situations, an analysis of the oral microflora is first performed to assess sensitivity to various antibiotics (it is quite expensive, so there is no need to refer each patient - it is carried out according to indications). Let us remind you that taking antibiotics is not compatible with alcohol.
Bone grafting and installation of protective membranes
This is the main surgical stage, the purpose of which is to restore bone volume, as well as remove all inflamed tissue. During the operation, the gum is cut and peeled off, thereby exposing the bone defect that the doctor will work with. In fact, this stage is similar to the first, but if the initial cleaning is only superficial, now it is deeper.
After peeling off the gingival flap using a scaler (ultrasonic device) or laser, granulations and inflamed tissues (gingival and even bone) are removed, as well as a better cleaning of the implant surface. After this, bone tissue is grafted (artificial or borrowed from another area), after which protective membranes are applied, which allow the grafted material to be securely fixed. It is worth noting that the technique of performing the operation depends directly on how many bone partitions (walls) are preserved around the implant. The more there are, the higher the chance of extending the life of the artificial root.
Application of PRF membranes from blood plasma
This is the main surgical stage, the purpose of which is to restore bone volume, as well as remove all inflamed tissue. During the operation, the gum is cut and peeled off, thereby exposing the bone defect that the doctor will work with. In fact, this stage is similar to the first, but if the initial cleaning is only superficial, now it is deeper.
At the stage of surgical intervention, our clinic also uses PRF membranes - this is a platelet mass obtained from the patient’s own blood. Numerous studies and our own practice prove that the use of membranes even at the stage of implant installation is an excellent prevention of peri-implantitis. And when treating this complication, blood plasma allows you to accelerate the process of regeneration of gingival and bone tissue.
Gum plastic surgery
This is the main surgical stage, the purpose of which is to restore bone volume, as well as remove all inflamed tissue. During the operation, the gum is cut and peeled off, thereby exposing the bone defect that the doctor will work with. In fact, this stage is similar to the first, but if the initial cleaning is only superficial, now it is deeper.
Plastic surgery can be either a consequence of bone grafting or an independent procedure. In the first case, it is needed to restore the aesthetics of the mucous membrane after surgery, especially when it comes to single tooth restoration. The position of the gums also needs to be adjusted due to the increase in bone tissue. In the second case, it is carried out when exposure of the installed implant occurs due to the gums being too thin in height or width, that is, when there is little mucous membrane or it does not fit tightly enough to the crown/implant.
Correction of orthopedic construction
In some situations, overload of installed implants leads to peri-implantitis. This can happen for several reasons:
- an incorrectly designed model of the prosthesis - this is why it is so important that complex dental restoration is carried out by several doctors at once: an implantologist and an orthopedist, who will create a single, properly functioning system,
- the patient eats inappropriate foods (for example, very hard foods immediately after implant placement),
- the patient does not come for prosthesis correction. After wearing removable appliances for a long time or without teeth for a long time, a person’s bite changes. With the help of prostheses on implants, we correct it, but we do it gradually - that is why the prosthesis is regularly corrected during the first six months to a year. So that it does not cause discomfort when closing the jaws and when chewing, and also does not cause overload of the implants.
How much does it cost on average in Moscow?
Treatment of complications
| Name of service | Cost, rub. |
| Periodontal applications in the area of 1 tooth | 370 |
| Application of a protective periodontal bandage | 400 |
| Laser therapy of the gum mucosa | 490 |
| Implant removal | 6900 |
| Implantation of osteoconductive material in the area of 1 tooth | 10900 |
| Implantation of a protective membrane (1 tooth) | 12900 |
Gum plastic surgery
| Name of service | Cost, rub. |
| Plastic surgery of marginal gums | 1200 |
| Gingivoplasty (1 tooth) | 1500 |
| Plastic surgery of marginal gums (segment) | 3500 |
| Plasty of gingival margin recession | 3500 |
| Flap surgery in the area of one tooth | 3500 |
| Smile line plastic surgery | 4000 |
| Gingivoplasty (1 tooth) using laser | 4000 |
| Gingivoplasty (segment) | 4500 |
| Flap surgery (three teeth) | 7000 |
| Gingivoplasty (segment) using laser | 10000 |
| Flap surgery (segment) | 10000 |
| Flap surgery (whole mouth) | 30000 |
Is re-implantation possible if the implant has been removed?
Classic two-stage implantation with delayed loading after removal of the implants will in most cases be impossible, since the bone tissue atrophies too much due to the inflammatory process. Naturally, in a number of situations, the option of increasing it is possible - but it will take several months for the initial rehabilitation of the tissue after the development of the inflammatory process, as well as another 3-6 months for the implanted material to engraft.
With complex implantation with immediate loading, rejection of all installed implants is extremely rare. There are cases when one of 8-10 structures does not take root, but in such a situation the load from the prosthesis is distributed evenly among the others without overloading them, and if necessary, the implant is replaced.
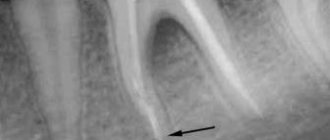
Why is the gum exposed under the implant?
Implant exposure is a fairly common occurrence. More common with two-stage implantation. A characteristic sign is the exposure of the metal rim of the abutment under the prosthesis, resulting in the formation of a black stripe . Usually the defect makes itself felt some time after the operation.
Common causes of complications:
- using an implant with a polished neck that remains above the bone surface after screwing in;
- too thin mucous membrane;
- overtension of the gingival flap;
- temporary crown pressure;
- poor quality oral care after implantation;
- mechanical trauma to the gums (toothbrush, hard food);
- improper formation of the gingival margin;
- subsidence of the bone as a result of long-term use of artificial teeth.
Prevention of peri-implantitis development
Thus, the following solutions allow us to solve the problem of the development of peri-implantitis:
- thorough diagnosis of the patient’s condition and planning of the treatment process,
- the choice of solid implants in which the intraosseous part is connected to the abutment, especially in situations where tooth restoration is carried out in the presence of generalized periodontitis,
- the choice of two-piece implants with an antimicrobial coating at the upper base of the implant body, as well as the use of abutments with a smooth antimicrobial coating,
- the use of polished implants that will not accumulate plaque,
- the use of implant models that transfer less load to the alveolar bone, which is susceptible to inflammatory processes,
- strict adherence by the patient to all recommendations of his doctor.
Thus, the main recommendation for patients is to choose a professional doctor who follows modern trends in the field of implantology, improves his skills, works with high-quality brands of implants and uses safe implantation protocols.
More examples 1 According to clinical studies of implant manufacturing companies: Nobel, Straumann, Astra Tech. 2 According to studies published in the journal Perio-implant advisory. 3 Esposito M1, Grusovin MG, Worthington HV Treatment of peri-implantitis: what interventions are effective? A Cochrane systematic review.