On the posterior surface of the upper jaw, facies infratemporalis, on its convex part, called tuber maxillare, there are two to three small openings, foramina alveolaria superiora posteriora, through which the posterior superior alveolar nerves enter. These nerves take part in the formation of the posterior part of the upper dental plexus and innervate the posterior part of the alveolar process, the three molars sitting in it and the corresponding part of the outer mucous membrane of this process and the mucous membrane of the maxillary cavity. To achieve conduction anesthesia in this area, you need to bring the anesthetic solution to the posterior superior alveolar openings.
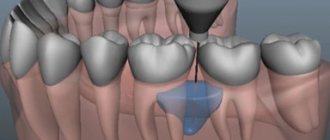
Location of the posterior superior alveolar foramina (target point of tuberal anesthesia)
To determine the target point, it is necessary, as mentioned above, to navigate using some easily accessible identification points. In this case, the upper teeth and the socket edge of the upper jaw are used.
The distance from the buccal wall of the socket of the upper wisdom tooth to the posterior superior socket openings is 2-2.5 cm.
We examined 75 skulls and upper jaws of adults and found the following distances from the buccal wall of the wisdom tooth socket to the posterior superior socket foramina: in 44 cases - 2 cm, in 23 - slightly less than 2.5 cm, in 8 - slightly more than 1.5 cm. Tuberculosis technique (tuberal) conduction anesthesia (injection site and needle direction) Intraoral method of tuberal anesthesia
When the patient's mouth is half-closed, the cheek is moved away with a mouth mirror, a spatula or a blunt hook. (Tightly closed jaws cause significant tension in the adjacent muscles, which prevents proper anesthesia from this route.) Then the zygomaticoalveolar ridge, crista zygomaticoalveolans, is felt, and behind it, above the second molar (closer to the third), slightly below the transitional fold (the place where the mucous membrane of the gums enters the mucous membrane of the cheek), a needle with a diameter of 0.75-0.8 mm is inserted and 4.5-5 cm long. At the same time, direct the syringe as far as the cheek allows, transversely to the bone, turning it so that the needle goes upward, backward and inward, all the time close to the bone. When encountering an obstacle, make slight turns. Thus, holding the bone, advance the needle 2 cm from the injection site and inject 1.5-2 ml of anesthetic solution there, after which they wait 10-12 minutes for the onset of complete anesthesia.
Contraindications and side effects
Contraindications to dental anesthesia are:
- Allergic reactions to substances included in anesthetics;
- History of cardiovascular diseases;
- Diabetes;
- Pathology of the endocrine system organs;
- Some types of severe injuries of the maxillofacial area.
Side effects of anesthesia in dentistry
Whether the doctor is a professional in his field, complications with local anesthesia in dentistry are very unlikely. There are some things that worry patients after dental treatment and, in principle, are a variant of the norm: swelling of the lip or swelling of the cheek, pain in the gums or even a headache for several hours.
However, all these symptoms should go away within 1-3 days after treatment. If you see that the situation is not improving or even worsening, contact the dentist who performed the procedure.
Intraoral method of conduction anesthesia.
At the tubercle of the upper jaw, we consider it not entirely satisfactory for the following reasons.
1. The injection site with the intraoral method is very unfavorable in terms of the possibility of infection, since the injection with Intraoral tubercular conduction anesthesia is made into the area of the mucous membrane behind the crista zygomaticoalveolaris. This area forms a fold with the mucous membrane of the cheek near the Stenon's duct, from where the flowing saliva prevents the surgical field from being kept dry and also washes away the iodine from the injection site, so that it partly loses its disinfectant effect.
2. With the intraoral method, it is necessary to move from the lateral surface of the upper jaw to the back, which is hindered by the cheek; therefore, the end of the needle, when moving along the posterior surface of the upper jaw, cannot have close contact with the jawbone, especially at the target point of this anesthesia. Due to non-compliance with one of the most important rules of conduction anesthesia, injury to the vessels and nerves passing through the soft tissues here is possible, which can lead to hematomas, persistent neuralgia, paresis and paralysis.
3. Often, intraoral tubercular conduction injection does not provide a complete analgesic effect. This is explained by the fact that the end of the needle always (with the intraoral method of this anesthesia) is at a certain distance from the target point - foramina alveolaria superiora posteriora, and the anesthetic solution often does not reach these holes.
4. Infection during tubercular conduction anesthetic injection into the infratemporal fossa is very dangerous. With this injection, due to the possibility of injury to the retromandibular vessels, hematomas are often formed in the infratemporal fossa, which, in the presence of infection, can easily fester and cause various complications.
Often, as a result of the formation of a hematoma that occurs during intraoral tubercular conduction anesthesia in the infratemporal fossa, neuritis of the infraorbital nerve occurs.
In cases of the absence of purulent-inflammatory processes and in the presence of minor pathological foci, instead of intraoral tubercular (tuberal) conduction anesthesia, we used plexual anesthesia (anesthesia of the upper dental plexus).
In case of purulent-inflammatory or extensive pathological processes of the upper jaw, we were more willing to resort to anesthesia of the entire maxillary trunk at the round foramen (see below).
But tubercular conduction anesthesia still has its indications. It is known that in the area of the upper first molar, the vestibular wall of the alveolar process is greatly thickened due to the zygomatic-alveolar ridge, as a result of which it is difficult to obtain complete anesthesia using infiltration anesthesia.
With a more developed alveolar process and a significant thickness of its bone walls, infiltration anesthesia does not provide the proper analgesic effect.
It should be pointed out that in the area of the molars, especially the first and second, there are almost completely no bone canals, with which the upper jaw is richly supplied in its other areas. This explains the insufficient analgesic effect obtained from infiltration anesthesia in this area.
In addition, infiltration anesthesia does not sufficiently anesthetize the mucous membrane of the maxillary sinus in the area of the tubercular conduction anesthetic injection.
To avoid these complications of intraoral tubercular conduction anesthesia, some authors recommend advancing the needle from the indicated injection site instead of 1.5-2 cm by only 0.5-1 cm. But with such advancement of the injection needle, plexual anesthesia is obtained (dental plexus anesthesia) , far from completely anesthetizing the posterior segment of the upper jaw.
In connection with the above, starting from 1928, we began to predominantly use the extraoral method of anesthesia at the tubercle of the upper jaw, which is much freer from the listed complications encountered with the intraoral method of this anesthesia. Extraoral method of tuberal anesthesia
With the extraoral method of conduction anesthesia at the tubercle of the upper jaw, the injection site can be well disinfected, the needle can be pointed directly at the bone and kept in contact with the bone during the entire advance, since the cheek does not interfere with turning the syringe in the desired direction.
Area of influence
Tuberal anesthesia affects the area from the gums of the first molar to the first molar. The needle enters the space between the optic nerve and the fat pad. In some cases, it is possible to reduce or increase the working space.
The anesthetic is injected near the alveolar ending, located behind the fixed jaw bone. The action extends to adjacent mucous tissues, the posterior part of the alveolar process and directly to the molars.
Anesthesia technique.
We feel the surgical field on both the right and left sides with the left hand, and always carry out the injection with the right hand. When performing extraoral tubercular conduction anesthesia on the right side, we turn the patient’s head to the left, and when operating on the left side, to the right.
When injecting on the right side, we place the index and thumb of the left hand from top to bottom on the tissues covering the zygomatic-alveolar ridge so that the index finger probes the anterior surface of the said ridge, and the thumb - the angle formed by the lower edge of the zygomatic bone and the zygomatic-alveolar ridge, and posterior surface of the ridge.
With the same fingers we try to pull down the soft tissues and fix them (especially with the thumb) as far as possible to the surface of the upper jaw, behind the zygomatic-alveolar ridge. We take a strong needle, with a diameter of 0.75 mm and a length of 4-5 cm. We make an injection at the named angle immediately to the bone (the back surface of the ridge). We immediately release a little anesthetic solution and from here direct the needle into the tissues, not too obliquely upward, inward and backward by 2-2.5 cm.
When injecting on the left side, place the thumb on the anterior surface of the zygomatic-alveolar ridge and the index finger on the (zygomatic-alveolar) angle and posterior surface of the ridge (Fig. 84). With these fingers, we pull the soft tissues of the cheek down and press this time (mainly with the index finger) to the surface of the jaw behind the ridge. Then everything goes the same way as with anesthesia on the right side.
Advantages and disadvantages
The advantages of this type of pain relief include:
- to achieve the effect, a minimal amount of solution is sufficient,
- the effect of anesthesia lasts for 2 - 3 hours,
- decreased salivation,
- You can numb large areas and deep tissues.
The disadvantages of the technique include:
- complex technique of execution,
- high probability of injury to blood vessels or nerves,
- the risk of painkillers getting into the blood vessels,
- high risk of all kinds of complications,
- risk of hematoma formation,
- Patient complaints of prolonged numbness that does not go away for a long time.
Complications of tuberal anesthesia
It should be borne in mind that during tubercular conduction anesthesia, the posterior superior alveolar artery (a branch of the internal maxillary artery) or the infraorbital artery may be injured. To prevent this complication, it is necessary, as already indicated, to stay directly at the bone if possible and not to immerse the needle more than 2.5 cm. The best way to avoid injury to blood vessels during any conduction anesthesia, and these vessels in particular, is continuous release anesthetic solution throughout the entire time the needle is advanced deep into the tissue towards the target point of anesthesia.
Bleeding from the injection site is easily stopped by pressing on the bleeding area with a sterile napkin.
With tuberous conduction anesthesia, as with other peripheral conduction anesthesia discussed below, an area of facial skin blanching may appear already at the beginning of the injection.
This phenomenon is usually associated with spasm of a vessel located in the area of anesthetic injection as a result of the slightest damage to its wall with an injection needle and even just the touch of the needle to the vessel. For the significance of this phenomenon, see the section “Anesthesia at the greater palatine foramen.”
Pallor of facial skin naturally occurs as a result of injury to the vessel and the entry into it of an anesthetic solution containing adrenaline, as well as as a result of washing the vessel with such a solution.
Anesthetic injection technique
- Consultation with a dentist, during which a specialist identifies the presence of any chronic diseases that may be a contraindication to one or another anesthesia.
- Identification of nerve endings whose sensitivity must be blocked.
- Treating the injection area with a disinfectant.
- Administration of the drug chosen by the specialist. In this case, the required dosage of the anesthetic and its rate of administration are calculated.
- Monitoring the patient after drug administration.
Immediately before the start of treatment, the patient is asked questions to understand the threshold of sensitivity and the effect of anesthesia.
The duration of action depends on the chosen anesthetic and dosage.
The anesthesia procedure is performed according to the following rules:
- the anesthetic temperature should be 36.6 degrees;
- anesthesia is injected into the nerve itself or into the trunk;
- in some cases, before administering the anesthetic, the injection site is treated with an anesthetic;
- The procedure is performed exclusively with sterile materials.
The main advantages of conduction anesthesia:
- the possibility of administering the drug outside the operated area;
- long-term effect, the duration of which can be controlled by a doctor;
- a minimum amount of administered drug is required;
- soft tissues in the treatment area are not deformed;
- salivation activity decreases;
- safety of the technique;
- affordable price.
Flaws
- the injection technique requires certain skills from a specialist;
- when administering the drug, it is possible to injure a nerve or vessel;
- age restrictions (not applicable under 12 years of age).
Tuberal anesthesia zone
Typically, the zone of tubercular conduction anesthesia reaches in front of the space between the upper second premolar and the upper first molar, behind the free end of the alveolar process, including part of the tubercle of the upper jaw and the buccal mucosa in the area of the upper first, second and third molars.
While studying the method, we used a dental probe to test the sensitivity (actually, pain, since even after the onset of analgesia, tactile and temperature sensations often remain) of the entire area after each tubercular conductive anesthetic injection. We noted several cases where painlessness extended to the middle of the second and even first premolars, although in the vast majority of cases the anesthesia zone border in front was the middle of the upper first molar.
How can we explain cases (albeit very rare) of anesthesia spreading forward to the upper premolars, when, as is known, only three upper molars are innervated by the posterior superior alveolar nerves, and the upper premolars are supplied by the middle upper alveolar nerves.
The authors who studied this phenomenon explain it by the existence of anastomoses between adjacent nerves. However, this can explain the onset of some anesthesia only in part of the second upper premolar, but not the spread of anesthesia to the upper first premolar inclusive.
We explain this phenomenon as follows. It is known that the middle superior alveolar nerves begin from the infraorbital nerve in the middle or posterior part of the infraorbital groove. However, there are cases when these nerves (middle superior alveolar nerves) begin, like the posterior superior alveolar nerves, in the pterygopalatine fossa before the entry of the infraorbital nerve into the groove of the same name. Then they enter jaw through holes that are also located on the back surface of the upper jaw. Thus, during the release of anesthetic fluid at the target point of this anesthesia, on the tubercle of the upper jaw, to interrupt the conduction of the posterior superior alveolar nerves with a similar anomaly of the infraorbital nerve, the conduction of the middle superior alveolar nerves can also be interrupted (the anesthetic solution in this case enters a bit higher)
The mucous membrane and periosteum on the side of the palate are not anesthetized during a tubercular conduction anesthetic injection, and to obtain complete anesthesia of all tissues of the upper jaw in the area of three molars, it is necessary to add palatal (palatal) conduction anesthesia to the tubercular conduction anesthesia of the anterior palatine nerve at the greater palatine foramen.
When is general anesthesia required?
General anesthesia in dentistry began to be used relatively recently and has already established itself as the preferred method of pain relief for some groups of patients. Classified by time and degree of shutdown. In this regard, the following are highlighted:
- Anesthesia. Performed by intravenous or inhalation access. Suitable for complex treatment in children and adults. It is mostly used for surgical interventions in dental surgery departments.
- Intravenous sedation. A method of reducing the sensitivity of pain due to inhibition of nervous excitability. During exposure, the patient may fall asleep for several hours. Medication-induced sleep allows for a large volume of therapeutic manipulations in children and adults.
General anesthesia and sedation are limited for use in practice due to a wide range of contraindications. Dental offices and clinics must be equipped with special resuscitation equipment, and must have an anesthesiologist on staff.
Pain relief for pregnant women
The harm from pain management during dental treatment in pregnant women is negligible compared to the potential complications caused by the source of infection in the oral cavity. Modern drugs allow dental anesthesia to be performed safely during pregnancy. Drugs with lower concentrations of adrenaline are used more often.
Anesthesia in pediatric dentistry
The problem of pain during dental treatment in children is still relevant today. The immature children's psyche and fear of manipulation make adequate and complete treatment impossible. To reduce pain sensitivity, gentle non-invasive methods are used.
Many patients ask the question: can they return to work after anesthesia? Experts unequivocally say that today the drugs are absolutely safe and do not lead to a deterioration in well-being.
What are the indications for tooth extraction?
Before tooth extraction surgery, the doctor prescribes an x-ray examination; the resulting images help assess the condition of diseased teeth.
- Detection of chronic periodontitis at the acute stage, when it is impossible to eliminate the source of inflammation in the area of the apex of the tooth using therapeutic methods
- In order to prevent the development of more serious complications
- Diagnosis of basal (near-root) tooth cyst
- Presence of inflammation or trigeminal neuritis
- If a problematic tooth constantly injures the mucous membrane of the tongue or cheeks
- If a tooth puts pressure on adjacent teeth, injuring their roots, which leads to bone resorption
- If a problematic tooth disrupts the normal bite and displaces neighboring teeth
- Multi-rooted teeth that have caused odontogenic osteomyelitis must be removed
- Sometimes the doctor prescribes tooth extraction to fit a removable denture
- With severe destruction by carious lesions
- If the tooth has not fully erupted and has an incorrect angle
- Due to progressive periodontal disease
- Due to an injury that resulted in a tooth fracture beyond repair
- If the teeth are in an incorrect position in the dentition (this situation is often detected during the eruption of wisdom teeth)
Subsequently, the removal of a tooth causes a gradual displacement of adjacent teeth; with prolonged absence of a tooth, this can lead to significant impairment of chewing function and noticeable deformation of the entire dentition. In order to prevent such complications, it is recommended to restore the extracted tooth by replacing it with an artificial one.
Modern dental practice has wide capabilities in the field of operative surgery and implantology, due to which replacing a defect in the dentition by installing a dental implant is the most natural and preferable; depending on the clinical situation, the modern patient has access to the latest technologies for the manufacture of dental bridges or removable partial dentures.
Results and discussion
The results of the first clinical signs of pain relief in the form of paresthesia in the area of the anterior third of the tongue and the corresponding half of the lower lip are presented in the table.
Clinical manifestations of anesthesia with methods of blocking the mandibular nerve according to P.M. Egorov and J. Gow-Gates, modified by S.A. Rabinovich and O.N. Moskovets The effectiveness of conduction anesthesia in the lower jaw according to P.M. Egorov was 92%, according to the modified method of J. Gough-Gates - 98%. In conditions of tissue inflammation when performing anesthesia according to P.M. Egorov noted effective pain relief in 89% of cases. When performing anesthesia according to the J. Gow-Gates method as modified, effective anesthesia occurred in 96%. At the same time, the number of complications, hematomas, positive aspiration tests, and post-injection pain was 1.9%. Slightly more (2.2%) local complications were observed during anesthesia according to P.M. Egorov.
When using the modified method according to J. Gou-Gates, when removing impacted and dystopic teeth, additional anesthesia was performed 2.6 times less frequently than using the P.M. method. Egorova. In addition, during anesthesia according to P.M. Egorov, insufficient anesthesia of the mucous membrane on the lingual side was identified in 3 (3.2%) patients, and on the buccal side - in 14 (15.2%) patients. With mandibular anesthesia according to the modified J. Gow-Gates method, insufficient pain relief on the lingual side was noted in 2 (2.1%) patients, and in the area of innervation of the buccal nerve - in 11 (11.9%) patients. Our data confirm that buccal nerve blocking is achieved in significantly fewer cases. A combination of any method of mandibular anesthesia with buccal nerve block is necessary.
Dynamics of somatosensory evoked potentials: after anesthesia according to the method of P.M. Egorov observed a rapid decrease in the amplitude of fluctuations of somatosensory evoked potentials. The amplitude of the sensation threshold reached its minimum values already at the 5th minute. When blocking the mandibular nerve according to the modified J. Gow-Gates method, the greatest decrease in the amplitude of fluctuations of somatosensory evoked potentials at all sensitivity thresholds was noted at the 10th minute, when determining the pain threshold and level of endurance - at the 10-15th minute. The dynamics of the amplitude of N2P2 oscillations of somatosensory evoked potentials at the sensation threshold, pain threshold and pain tolerance level after blockade of the mandibular nerve are presented in the figure.
Dynamics of the amplitude of N2P2 fluctuations (negative and positive waves) of somatosensory evoked potentials at the sensation threshold (TS), pain threshold (PT) and pain endurance level (PAL) after blockade of the mandibular nerve according to P.M. Egorov and according to J. Gou-Gates (modified) using a 4% solution of articaine with adrenaline at a concentration of 1:100,000.
Thus, clinical and physiological studies have shown that the effectiveness of conduction anesthesia in the lower jaw depends on the method of injection anesthesia, the composition of the local anesthetic drug, the type of dental intervention and the presence or absence of an inflammatory process in the anesthetized tissues.
Preparing the patient for the procedure
The skillful hands of the doctor, the correctly selected anesthetic and the patient’s attitude are the main components of a good result of the tuberal method of pain relief and a favorable outcome of surgical intervention. To avoid various complications, doctors adjust the patient’s diet. Food should bring maximum benefits so that the body can gain strength and resist possible complications after surgery. To do this, the patient must eat more vegetables, fruits, boiled meat and fish.
7 days before the upcoming procedure, the patient should give up long physical exertion and strong emotions, stay in clean air longer, and monitor sleep and wakefulness. The ideal option would be a vacation during which the patient’s body can rest and gain strength for the upcoming operation and subsequent rehabilitation.
It would be a good idea to undergo a complete examination of the body. It will tell you about all hidden diseases and predispositions. The doctor may prescribe a complex of vitamins to the patient as therapy to maintain the body.
It is prohibited to drink alcohol during preparation for surgery. Several weeks before the upcoming procedure, you should stop taking medications. If this is not possible, the doctor must be informed about this so that he can adjust the anesthetic administered.