Children's dental appointments have long ceased to be something special. It is now considered the norm to bring the happy owner of his first teeth to a pediatric dentist in order to develop in the child the right attitude towards dental care and the prevention of possible problems with them. It would seem that there is no caries, there is no yellow plaque either, nothing indicates a problem, so the diagnosis of “malocclusion” or “anomaly of occlusion” is like a bolt from the blue for many.
At 2-3 years of age, when the primary occlusion is still forming, it is almost impossible for a non-physician to identify the prerequisites and first signs of problems with occlusion. However, this is the very time when the applied correction techniques give the best results with virtually no costs. When signs of problems with the development of the dental system become obvious, it is still not too late to correct the pathological changes. The most important thing is not to put off a visit to the orthodontist and not wait for the time when lack of treatment will lead to complications.
Which bite is considered correct?
Normally, the sizes of the jaws should correspond to each other, the arrangement of the upper and lower jaws should be symmetrical, the dentition should be even and close in a certain way: the large and small molars are in close contact with each other, and the upper incisors and canines overlap the lower ones by no more than a third of the height crowns This overlap is achieved due to a certain inclination of the dentition outward, when the outer arch is larger than the inner one.
There are a great many options for deviations from the so-called “central occlusion”. In children and adults, there are five main types of orthodontic anomalies, the severity of each of which can vary widely. Let's look at these five varieties in more detail.
Types of pathological bite in children:
- Distal. The lower jaw is disproportionately small in relation to the upper jaw due to its underdevelopment or, conversely, excessively rapid growth of the upper jaw.
- Mesial. In this case, the lower jaw, on the contrary, is disproportionately large and noticeably pushed forward. The disorder can occur due to underdevelopment of the upper jaw, excessively rapid growth of the lower jaw, or a combination of both of these processes.
- Cross. There is a violation of symmetry in the development of the jaws. As a result, in a certain place the closure of the dentition resembles scissors.
- Deep. The upper front teeth overlap the lower ones by more than half. When the anomaly is severe, the lower teeth rest against the gums of the upper jaw and can seriously injure soft tissues when chewing.
- Open. The most complex of the types of dental anomalies, in which the dentition does not close over a certain length, forming a noticeable gap. Usually the gap between the dentition is located between the incisors and canines above and below, but the defect can also be localized in the lateral regions.
In the case of ideal development of the dental system, an orthognathic bite is formed. In addition to the correct closure of the dentition, it is characterized by the absence of gaps between the teeth, crowding, and incorrect position of the teeth in the dentition. However, unfortunately, few people are naturally gifted with such a bite.
Why are the first teeth called baby teeth?
There are several opinions on this matter. Doctors attribute the authorship of the term to Hippocrates, who believed that these teeth are formed from mother's milk. Philologist N.N. Vashkevich states that “the term is a tracing from the Latin lactose “milk”. But the tracing paper is false, it is a misunderstood Arabic liwaqt - “for a while,” “temporary.”
One way or another, the first teeth actually actively “feed” on breast milk, since it is from it that the child absorbs the main building material of teeth and bones – calcium. And although baby teeth erupt, as a rule, at 6-7 months, their formation in the child’s jaws occurs long before that.
It is worth noting that for the health and strength of the first teeth, it is mother’s milk (not cow’s) that is necessary, since the nutrients from it are maximally absorbed by the baby’s body. Therefore, the universal recipe “breastfeed your baby” will help in this matter.
Signs of occlusion pathology
In most cases, it is impossible to determine the “correctness” of the bite visually. This can be done by an orthodontist, who is highly advisable to see the child annually, from the eruption of baby teeth to the completion of the formation of a permanent bite. A specialist can identify an emerging problem, and even the prerequisites for the fact that the bite may be formed incorrectly.
For example, crowding of baby teeth significantly complicates the process of eruption of permanent teeth. Molars are larger than primary teeth, so they generally need more space in order to occupy the correct position in the dentition.
When examining a child’s teeth, parents are unlikely to be able to assess the symmetry and uniformity of jaw development and the correct placement of teeth in the dentition. But there are other manifestations, the presence of which may indicate problems with occlusion or a predisposition to the development of orthodontic anomalies:
- Incorrect breathing. We can breathe through our mouths if, having caught a seasonal ARVI, we suffer from a runny nose. This is fine. It is a completely different matter if the child breathes through his mouth all the time out of habit or due to the presence of enlarged adenoids.
- Snore. Children can snore in their sleep only if there are serious disorders in the development of the dental system. This feature, unusual for childhood, should not be left unattended. Not only can you miss the best time to correct your bite, but during sleep apnea the brain does not receive enough oxygen, which can affect the mental abilities of a growing person.
- Certain facial features. What matters is the structure and proportionality of the lower third of the face. The chin should not be too massive, nor, on the contrary, sloping back. The upper jaw should also not be the most protruding part of the face, as this indicates its hypertrophy.
- Posture disorders. Changes in bite due to scoliosis and other disorders in the musculoskeletal system can develop as a compensatory reaction of the body, which needs to develop coordination of movements and the ability to maintain an upright body position at any cost.
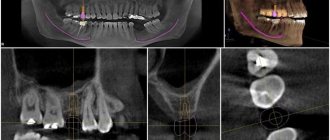
Decoding the results
The finished images must be deciphered by a specialist. It is possible that several doctors will be present during the decoding, for example a radiologist
, dentist, otolaryngologist.
The photographs are used to assess how symmetrically the teeth and jaws are positioned. If a focus of any pathology is detected, it is important to determine its exact location and size.
When diagnosing a jaw fracture, you need to determine its complexity, consider whether there are fragments and how they are located.
If a tumor-like neoplasm is detected, it is important to assess its size, consider its boundaries (clear or blurred), and determine its location.
Causes of occlusion pathology
The formation of the dental system is influenced by a number of external and internal factors. If it is possible to identify such a causative factor and eliminate it in time, then the correction of violations is much easier and faster. We have combined the most significant reasons into one list:
- Heredity. The presence of occlusion pathology in one of the parents increases the likelihood of a defect forming in the child by 40%. If a pathology in the structure of the dental system is detected in both parents, then you should not expect a miracle. It is better to contact an orthodontist in a timely manner and artificially “direct” the growth of teeth and jaws in the right direction.
- Bad habits. The child actively tastes any objects. There is nothing wrong with this until holding something in your mouth and sucking becomes a habit. Absolutely everything is used: the edge of the blanket, fingers and even lips. Pacifiers do not cause harm only in cases where the child weaned off them in a timely manner.
- Problems of the musculoskeletal system. The bite affects the condition of the spine, primarily the cervical and thoracic regions. And pathology of the musculoskeletal system, for example, flat feet, is a significant factor that can disrupt the normal development of the bones of the facial part of the skull.
Periods of skull development
The process of formation of the skull
There are several periods of development. The first lasts until 7 years from birth. At this time, the skull grows rapidly and actively increases in volume. The seams become narrower and the fontanelles gradually become smaller. The cavities of the eye sockets and nose are formed, and the shape of the lower jaw changes.
From 7 to 14 years, the second period continues, during which the shape of the skull and its parts does not change so intensively, however, the cavities of the orbits and nose, and the mastoid process increase significantly.
The third period lasts from 14 to 25 years, encompassing puberty. Over the years, the facial skull lengthens slightly and the frontal regions are formed. The area of the arched cheekbones is significantly increased, and the frontal tubercles are more noticeable.
The fourth period (25-45 years) is characterized by ossification of the sutures. Experts have noticed that early ossification of the vitreous suture leads to the formation of short, and the coronal suture – long-shaped skulls.
The fifth period begins at approximately 45 years of age. Gradual atrophy of the facial and brain regions occurs. Since many people have fewer teeth at this time, the shape of the jaws changes. The alveolar processes and other parts are smoothed, the angle of the lower jaw increases slightly, and the facial region decreases in volume.
What if the bite is not corrected?
Anomalies of occlusion cause physical and psychological discomfort to their owners. Psychological problems are more significant for children and adolescents, as crooked teeth often become a reason for ridicule. Physical discomfort begins already in adulthood, when the body's resources are depleted. Improper distribution of the load when chewing leads to problems in the temporomandibular joints, rapid abrasion of enamel, and periodontal diseases. Accelerated tooth decay requires expensive prosthetics at a much earlier age than would be the case in the absence of occlusal anomalies.
Deviations from the norm
The most common causes of deviations from the norm are developmental anomalies, congenital pathologies and birth injuries. Often injuries occur if the fetal head does not match the size of the mother's birth canal. However, almost all consequences can be corrected by the first year of life.
During this period, it is necessary to follow a number of recommendations related to caring for the baby. Often, the irregular shape of the head (occipital part) is a consequence of lying on the back for a long time. A flat neck sometimes indicates a lack of vitamin D, which can cause rickets in young children. When the fontanel is still open, it is not recommended to direct a stream of water onto the baby’s head.
Congenital diseases are much more difficult to cure. Particularly dangerous is dropsy of the brain or hydrocephalus. It can be detected during pregnancy and treatment can begin immediately.
Sometimes pathological deformation of the head in a child occurs:
- sloping back of the head (plagiocephaly);
- curvature of the occipital and frontal area (scaphocephaly);
- elongated shape (acrocephaly).
Asymmetry and curvature of the skull often lead to neurological pathologies, as well as retardation in physical and mental development.
Examination of a child by a neurologist
During the first month, asymmetry of the skull may be noticed by parents or a pediatrician during a routine examination, who will give a referral to a neurologist. In difficult cases, it is necessary to consult a neurosurgeon.
You should visit a neurologist for the first time when you are a month old. The main task of a specialist is to correctly diagnose the pathology, preventing the disease from developing. An experienced doctor will determine what abnormalities exist in the circumference and girth of the head. Up to a year, visits to a neurologist are scheduled every 3 months.
Large and small fontanelles on the head of a newborn - why are they?
Not only the size of a child’s head matters, but also its shape and fontanel.
This invisible and constantly pulsating island on the baby’s head always scares mothers. And this is understandable - won’t ordinary touching the fontanel affect the baby’s health?
Therefore, you need to know why fontanelles are needed.
So, in short, this is a reliable protector of the baby, who must gradually adapt to our world.
And you also need to know that there is not one, but two fontanelles - large and small:
- Big spring. This is the “breathing” place on the top of the head, approximately 2x2 cm in size. It shrinks as the baby grows and becomes overgrown around the age of one year.
- Small fontanel . It is located on the back of the head, and it is much smaller (up to 1 sq. cm.) of its fellow. Many mothers do not even suspect the presence of a small fontanelle, since it is difficult to palpate (which cannot be said about premature babies).
YOU NEED TO KNOW THIS : Children's fontanelles close differently due to individual development. But, if the fontanel does not heal by the due time, you should consult a pediatrician.
Torticollis in a child at birth - causes and symptoms of torticollis in newborns