Author: Alan H. Gluskin
The development and implementation of principles for shaping, cleaning and filling root canals poses potential and real challenges when it comes to the anatomical complexity of root canals and technical solutions to provide mechanical and medicinal canal debridement and obturation. In this review, we will focus on the reasons why material is removed beyond the root apex. We will look at how various sources define the term “extrusion of material beyond the apex,” try to come to a consensus on the definition of the working length, identify the influence of the canal shape on the overflow of material, and also find out the biological effect of filling materials extended beyond the apex. In addition to all of the above, the article will provide techniques to prevent channel overflow, as well as local factors affecting regeneration.
You can fail in many ways, but succeed in only one.
Aristotle
The cause of toothache is defects in canal filling
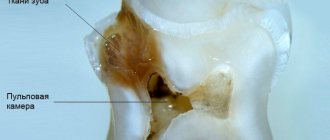
The most common cause of toothache after nerve removal is defects in filling the tooth canals. It is not always possible for a dentist to completely fill the cleaned canals of a tooth. Often, the desire not to leave voids in the tooth canals leads to squeezing out the filling material beyond the root.
Correct canal fillingA normally filled tooth canal during the treatment of pulpitis | Underfillingtooth canalThe filling material does not reach the root apex (to the end of the canal) | Refilling a tooth canalFilling material extends beyond the root of the tooth |
Why does a tooth hurt when it is not filled?
Underfilling does not cause pain immediately. The pain may appear after a month or even several months. A focus of infection forms in an empty, unfilled canal. Over time, the infection extends beyond the root tip and causes periodontitis (inflammation of the periodontium - the tissue behind the root tip). Then a cyst grows in this place. This, of course, can cause aching and even acute toothache and swelling.
Why does a tooth hurt during refilling?
More often, pain occurs during prefilling. The filling material rests on the bone tissue, puts pressure on it and causes pain.
What to do if a tooth hurts after nerve removal?
If the pin goes beyond the root of the tooth, you need to open the filling, clean the canal again and refill it.
If root cement has escaped beyond the tooth root, it is necessary to estimate how much material has escaped. If a lot of material has come out, then you will also have to unseal everything, expand the top of the canal and wash out the old cement, and then refill the canal and seal it. If a little material comes out, then it makes sense to wait - most likely the dental material will resolve.
Features of the immune system and toothache
The reaction to the shortcomings of root canal filling is very individual and depends on the characteristics of the person’s immune system.
Many patients come to our center. And in some photographs, the canals are half sealed, but no inflammation occurs. The human immune system copes 100%. For others, the slightest underfilling of the canal causes inflammation and pain.
The cement that comes out of the canal in some patients quickly resolves and does not cause problems, while in others it comes out just a little and immediately hurts.
Extension of filling material beyond the apex: endodontic failure versus clinical success
Many dentists believe that procedural errors in daily practice, such as extrusion beyond the apical foramen and contact of filling material (most often gutta-percha and zinc oxide eugenol sealer) with periapical tissues after treatment, are a direct cause of endodontic failure.
Some authors show the negative impact of extending the filling material beyond the apex on the predictability of endodontic treatment and emphasize the following:
- High incidence of postoperative pain with exacerbation of inflammation
- Toxicity of materials
- Constant irritation of the periapical tissues with manifestations ranging from mild inflammation to a general reaction of the body.
In contrast, other authors have argued that apex extrusion in itself does not directly contribute to endodontic failure, although it should be avoided. Ingle says that endodontic treatment can be successful despite extrusion of material beyond the root apex. Schilder notes that he has not encountered complications specifically associated with excessive filling of the canal. Weine states that periapical tissues, fortunately, tolerate contact with gutta-percha well and therefore endodontic failure due to its removal beyond the apex is rare. In most cases, there is no pathological radiological evidence, and sometimes there is even a decrease in the amount of excreted material due to phagocytosis.
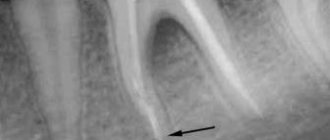
Image 1 – Mandibular first molar with amalgam filling and insufficient root canal obturation.
After retreatment, the radiograph shows three-dimensional filling of the root canals with a slight extension beyond the apex in the mesial canals obturated with Thermafil #25 and in the distal canal obturated by vertical condensation of heated gutta-percha.
After 5 years, the excess material had disappeared and the periapical tissue remained healthy.
These contradictory results can be explained by differences in research methodology and different composition of the derived materials. In general, the most common causes of discrepancy are related to differences in apical anatomy, limiting the effectiveness of endodontic treatment in various clinical situations.
Image 2 - The main factors leading to the removal of material beyond the root apex:
External inflammatory apical root resorption associated with apical damage to a previously treated tooth.
Incompletely formed root.
Excessive instrumentation with deviation from the natural course of the canal and apical perforation.
Inadequate handling of plasticized or unplasticized gutta-percha and sealants during obturation.
It is extremely important to identify and distinguish between the removal of filling material in three-dimensionally cleaned, formed and obturated root canals and in canals with obstructive overflow in combination with incomplete internal obturation.
Image 3 – Typical view of an exposed gutta-percha point: note the scratches on the point.
Image 4 – The apical foramen is completely filled.
Image 5 – Proper expansion for obturation, but insufficient filling of the canal. Note the transport of the apex during canal formation. (Courtesy of Dr. M. Vitullo).
Image 6 - Postoperative radiograph of the mandibular first molar showing a large apical lesion of endodontic origin. The mesial canals were obturated with Thermafil. A follow-up examination after 4 years shows osteoreparation. Excess filling material did not interfere with bone restoration.
Image 7 – Thermafil carrier extended beyond the apex in the distal root. Thermafil is a good method of obturation if the protocol is followed. The media was removed and the canals were refilled. After 6 months, the lesion was smaller than on the preoperative radiograph, and the patient noted the disappearance of pain when chewing.
Image 8 - These images show that even MTA can be released into the periapical tissue. In this case, the rule is the same as in the previous examples: if the canal is well cleaned, excess MTA cannot interfere with tissue restoration. 6-year follow-up kindly provided by Dr. R. Tonini.
Conclusion
Obturation is the last stage of endodontic treatment. Bringing either sealer or gutta-percha beyond the apical foramen will not necessarily be a mistake when performing obturation. However, this may result in an error in canal formation when parallel canal walls were created instead of conical ones, apical resorption or expansion of the apex.
Therefore, it is necessary to determine the direct causes of excessive root canal filling. “Is the excess material remaining after a complete three-dimensional obturation or is the material brought beyond the apex in combination with incomplete internal obturation of the canal?” Excess material beyond the apex is clearly not the goal of endodontic treatment, but rather the result of safely generated hydraulic forces in achieving three-dimensional obturation of the root canal system.
Numerous cases of root apex removal that have been successful, as evidenced by clinical and radiological signs of long-term restoration of periapical tissues, should reassure patients, doctors and insure against any legal charges.
Source: forum.stomatologija.su, styleitaliano.org
Introduction
Most problems in endodontics are related to the complex anatomy of the root canals and pulp chamber. For successful treatment, it is first necessary to provide access, then clean and shape the root canals so as to ensure the most effective and complete filling of the formed canals. It is safe to say that the scientific and technical aspects of endodontics have improved significantly over the past two decades. These developments help treat the pulp cavity with more reliable and advanced methods. Although these improvements have reduced the chance of iatrogenic problems, they have not completely eliminated them.
A ten-year-old report from the European Society of Endodontology states that “the goal of any technique is to hermetically fill the prepared root canals from the pulp chamber to the root apex with a biocompatible material.” If the ultimate goal of root canal treatment is to ensure that the root canal is protected from re-infection by bacteria, then filling the canal is an important factor affecting the long-term results of the treatment, as well as the health and safety of the patient.
The development and implementation of principles for shaping, cleaning and filling root canals present potential and real challenges when it comes to the anatomical complexity of root canals and technical solutions to support mechanical and medicinal canal debridement and filling. How can we create the molds we need in a biologically-like manner and how can we be sure that these molds will ensure complete filling of the canal with material and positive long-term results?
In this review, we will focus on the reasons why material is removed beyond the root apex. We will look at how different sources determine canal overfilling and material overexpansion, try to come to a consensus on determining the working length, identify the influence of shape on the extension of material beyond the apex, and also find out the biological effect of filling materials extended beyond the apex.
Filling the root canal using the single pin method with a sealer based on tricalcium silicate
Randall Cohen, DDS , Consultant, Alleman-Delipieri Center for Biomimetic Dentistry, General Dentist, Temple University (Philadelphia, PA, USA). INTRODUCTION
Lateral condensation and vertical compaction of gutta-percha have been widely used in endodontic practice in recent decades. The need to seal gutta-percha historically arose due to the fact that sealers themselves did not allow achieving an adequate result. The sealers were hydrophobic, unstable in volume, not biocompatible, subject to degradation and caused periodontal irritation when removed beyond the root apex. As a consequence, all modern techniques - lateral condensation, vertical compaction, hot gutta-percha on a carrier - have been developed to achieve a minimum volume of sealer. It was generally accepted that increasing the amount of sealer leads to shrinkage, microleakage and failure, and all root canal filling techniques were aimed at achieving a minimum thickness of the sealer layer.
This article provides an overview of the goals of endodontic treatment and the main obturation techniques. Its author proposes a simpler method of root canal filling using one gutta-percha point and a new material based on tricalcium silicate, which does not have the disadvantages of traditional sealers. Goals of endodontic treatment
The triad of biomechanical preparation, antibacterial treatment and complete obturation forms the basis of endodontic treatment.1
The tooth cavity and root canals must be thoroughly cleaned of organic residues and given the correct shape. This is achieved by instrumental and medicinal treatment of the root canal, after which the root canal is free from infection and ready for obturation.
A good sealer for filling destroys all bacteria remaining in the root canal system, depriving them of nutrition and creating conditions that make it impossible for them to reproduce. In addition to this, the root canal filling material must have antimicrobial properties to prevent further bacterial growth. It is also important to provide both coronal and apical sealing to prevent bacterial entry and reinfection.
For filling root canals, today it is generally accepted to use gutta-percha as a material with the necessary properties. Gutta-percha is insoluble, has minimal impact on tissue, is well tolerated by the body, is stable in volume and, if necessary, can be dissolved using a solvent.
Another component used for obturation is a sealer, which complements gutta-percha.
The sealer must:
- Easily inserted into the root canal.
- Seal the apex and lateral canaliculi.
- Do not shrink.
- Be impermeable to moisture.
- Possess bacteriostatic properties.
- Be radiopaque.
- Do not stain tooth tissue.
- Do not irritate periapical tissues.
- Subject to sterilization.
- If necessary, it can be easily removed from the root canal.1
Modern methods of root canal obturation
There are several methods of root canal obturation, each of which uses gutta-percha. The first technique is called lateral condensation (Fig. 1), under which root canals are usually treated using the traditional “step back” system.
Rice. 1. Lateral condensation The master pin, coated with sealer, is set to working length, and then the dentist, using a spreader, compacts additional pins until the entire space between the master pin and the root canal wall is filled.
Another method of filling root canals - vertical compaction (Fig. 2), first proposed by Schilder2 - involves installing a master pin coated with gutta-percha to the working length.
Rice. 2. Vertical compaction of hot gutta-percha Then, with a red-hot plager, the gutta-percha is thermoplasticized and compacted. This filling technique creates hydraulic pressure to fill the laterals and other branches of the root canal system. The coronal two-thirds of the master pin are removed when the heated plug is removed, and a “plug” is formed in the apical third, allowing controlled filling of the root canal with softened gutta-percha. This technique has many advantages, but also disadvantages compared to lateral condensation. One of the problems is the need to widen the orifice of the root canal sufficiently to insert a hot plug into the apical third (less than 4 mm from the root apex).
Other problems with vertical compaction are heterogeneity, relatively large amounts of sealer in the apical zone, poor adaptation to the root canal walls, and extension of gutta-percha beyond the apex.3
For the long-term survival of the tooth, it is critical to preserve as much coronal dentin as possible. This must be taken into account not only when creating the minimum possible endodontic access, but also when choosing a restoration technique. Unfortunately, both root canal filling methods require root canal preparation, which removes large amounts of coronal dentin and reduces the strength of the tooth. Method of filling a root canal using one pin
Recently, dentists have increasingly used the single pin method4 (Fig. 3), especially with a large taper corresponding to the taper of root canals after treatment with nickel titanium endodontic instruments (NiTi).
Rice. 3. Single pin method This technique does not require additional pins, lateral condensation, or vertical compaction of hot gutta-percha. In other words, the root canal is filled with a master pin corresponding to the last nickel-titanium instrument used. This combination of the single pin and sealer method allows you to avoid mistakes that are possible when using other root canal filling methods. This method is much easier for the dentist, requires less time, which makes treatment easier for the patient, and also does not result in pressure on the canal walls. Root canal treatment with nickel-titanium instruments
The use of rotary nickel-titanium root canal instruments allows for a simpler obturation method using a single pin (corresponding to the size of the last file used) tightly adjacent to the walls throughout the entire length of the root canal. By supplementing this technique with a bioactive, biocompatible, non-shrinking sealer, the requirements for successful preparation, disinfection, shaping and filling can be met without excessive dentin removal and a high long-term treatment success rate can be achieved. Sealer based on tricalcium silicate
Sealer based on tricalcium silicates BioRoot RCS (Septodont) has many advantages over materials of previous generations. Due to its alkaline pH (providing antibacterial properties), calcium ion release, sufficient radiopacity and flowability, BioRoot RCS is superior to all materials used today. BioRoot RCS is volume stable, biocompatible, hydrophilic, stimulates bone regeneration and provides sufficient adhesion to dentin in root canals. CLINICAL CASE
A 68-year-old patient consulted a dentist with complaints of pain in the left lower jaw. According to the patient, she took the antibiotic Augmentin, prescribed to her by her general practitioner. An x-ray showed a focus of bone tissue destruction and a diagnosis was made: periapical abscess of tooth 35.
The root canal was prepared to size 30.06. Irrigation was carried out with a 5% sodium hypochlorite solution. The root canal was washed with an anesthetic solution (Septocaine, Septodont) and solutions of EDTA and chlorhexidine. After repeated treatment with anesthetic, the canal was again washed with 5% sodium hypochlorite solution. A 30.06 master pin was then fitted and BioRoot RCS sealer was prepared according to the manufacturer's instructions. The root canal was dried with paper points and filled with BioRoot RCS using a master point. After this, the master pin was removed from the root canal, re-coated with sealer and set to working length. The master pin was cut at the level of the orifice with a heated plugger, and excess sealer was removed with a No. 2 spherical diamond bur (Fig. 4–7).
Rice. 4. Diagnostic radiograph
Rice. 5. The root canal is processed, the master pin is adjusted to the working length
Rice. 6. The master pin coated with BioRoot RCS (Septodont) at the mouth is cut off with a hot plugger
Rice. 7. A follow-up radiograph after one year shows complete healing of the periapical lesion. DISCUSSION
For the success of endodontic treatment, thorough instrumental and medicinal cleaning of the walls of the root canals, as well as high-quality filling, is necessary.
Sealers have disadvantages - shrinkage, degradation, irritation of surrounding tissues. As a result, traditional filling methods are aimed at filling the space of root canals with gutta-percha in such a way as to minimize the amount of sealer, which requires a lot of time, so success highly depends on the qualifications of the doctor, their use is tedious for both the dentist and the patient, and can even cause root cracks due to excess pressure.
The new method uses a single pin in combination with a tricalcium silicate sealer, overcoming the challenges associated with previous generations of materials. The new sealer based on tricalcium silicate has antimicrobial and anti-inflammatory properties, binds to dentin, remains stable in volume, that is, it most fully meets the requirements for an ideal material for filling root canals. Accordingly, there is no need to apply significant force to push the sealer, since it fills all the voids in the root canal, due to its hydrophilicity, and prevents the growth of bacterial colonies. Due to the lack of shrinkage and degradation, there is no apical and coronal microleakage. There is also no risk of tooth root fracture, since the master pin used for filling is inserted to the working length without pressure. In addition, there is no need to weaken the tooth by removing coronal dentin to allow the plugger to reach the apex. LITERATURE
- Cohen S, Hargreaves K. Pathways of the Pulp 9th ed. Mosby, St. Louis, MO, 2006.
- Schilder H. Filling root canals in three dimensions, Dent Clin of North Amer 1967;723-44.
- Tasdemir T, Er K, Yildirim T, Buruk K, Çelik D, Cora S, et al. Comparison of the Sealing Ability of Three Different Techniques in Canals Shaped with Two Different Rotary Systems: a Bacterial Leakage Study Oral Surg Oral Med Oral Pathol Oral R adiol Endod 2009 Sep;108(3):e129–34.
- Pereira C. A., et. al. Single-Cone Obturation Technique: a literature review. RBSO Oct/Dec 9(4):442–7 2012.
Go to the website of the exclusive distributor of Septodont in Russia Dental Times 37
Complications of pulpitis without treatment
If pulpitis is not treated, the inflammation progresses, extends beyond the root canal, and affects adjacent periodontal and periodontal tissues. Most often this leads to periodontitis. Acute periodontitis is manifested by sharp pain, which is localized in the area of the affected tooth. The intensity of the pain gradually increases, it becomes throbbing when purulent inflammation begins. If treatment is not started at this stage, purulent exudate begins to separate, and the periodontal collagen fibers are destroyed. Soft tissues swell, temperature rises, and general condition worsens.
With periodontitis, the ligaments that hold the tooth in the alveolus are destroyed, and the destruction of bone tissue begins. The tooth becomes loose and falls out. Large cysts may appear.
Another possible complication of pulpitis is periostitis. With periostitis, inflammation spreads to the periosteum (tissue surrounding the bone), and a flux is formed. The gums swell and the jaw becomes painful. Periostitis can appear after pulpitis or accompany periodontitis. Without treatment, the swelling of the gums increases, the pain intensifies, the cheek and lip near the site of inflammation swell. The pain becomes shooting and can affect the temple, eye, ear. A fistula (passage) may appear in the swollen gum, through which pus comes out. After the fistula tract appears, the inflammation becomes less intense, but the tissues remain infected, and the infection continues to spread, and periostitis from an acute form becomes chronic.
Pulpitis can provoke the development of periodontitis - an inflammatory disease of the gums, dangerous by the destruction of bone tissue, gradual recession of the gums, and adentia. Against the background of acute inflammation and tissue infection, severe systemic diseases may appear: general sepsis (blood poisoning), phlegmon (breakthrough of pus into the soft tissues of the face, requiring surgical intervention), amyloidosis (occurs due to the constant toxic effect of pus).