Children's dental appointments have long ceased to be something special. It is now considered the norm to bring the happy owner of his first teeth to a pediatric dentist in order to develop in the child the right attitude towards dental care and the prevention of possible problems with them. It would seem that there is no caries, there is no yellow plaque either, nothing indicates a problem, so the diagnosis of “malocclusion” or “anomaly of occlusion” is like a bolt from the blue for many.
At 2-3 years of age, when the primary occlusion is still forming, it is almost impossible for a non-physician to identify the prerequisites and first signs of problems with occlusion. However, this is the very time when the applied correction techniques give the best results with virtually no costs. When signs of problems with the development of the dental system become obvious, it is still not too late to correct the pathological changes. The most important thing is not to put off a visit to the orthodontist and not wait for the time when lack of treatment will lead to complications.
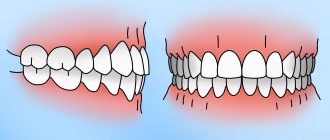
Which bite is considered correct?
Normally, the sizes of the jaws should correspond to each other, the arrangement of the upper and lower jaws should be symmetrical, the dentition should be even and close in a certain way: the large and small molars are in close contact with each other, and the upper incisors and canines overlap the lower ones by no more than a third of the height crowns This overlap is achieved due to a certain inclination of the dentition outward, when the outer arch is larger than the inner one.
There are a great many options for deviations from the so-called “central occlusion”. In children and adults, there are five main types of orthodontic anomalies, the severity of each of which can vary widely. Let's look at these five varieties in more detail.
Types of pathological bite in children:
- Distal. The lower jaw is disproportionately small in relation to the upper jaw due to its underdevelopment or, conversely, excessively rapid growth of the upper jaw.
- Mesial. In this case, the lower jaw, on the contrary, is disproportionately large and noticeably pushed forward. The disorder can occur due to underdevelopment of the upper jaw, excessively rapid growth of the lower jaw, or a combination of both of these processes.
- Cross. There is a violation of symmetry in the development of the jaws. As a result, in a certain place the closure of the dentition resembles scissors.
- Deep. The upper front teeth overlap the lower ones by more than half. When the anomaly is severe, the lower teeth rest against the gums of the upper jaw and can seriously injure soft tissues when chewing.
- Open. The most complex of the types of dental anomalies, in which the dentition does not close over a certain length, forming a noticeable gap. Usually the gap between the dentition is located between the incisors and canines above and below, but the defect can also be localized in the lateral regions.
In the case of ideal development of the dental system, an orthognathic bite is formed. In addition to the correct closure of the dentition, it is characterized by the absence of gaps between the teeth, crowding, and incorrect position of the teeth in the dentition. However, unfortunately, few people are naturally gifted with such a bite.
Classification
In orthodontics, there are several classifications of this disorder. Let's look at the most commonly used of them.
The classification according to Beltman A.I. includes the following types of anomalies:
- lower micrognathia (reduction in the size of the alveolar process) with a normally developed upper one;
- micrognathia above with proportionally developed lower part;
- upper macrognathia (increase in the size of the lower alveolar process) combined with lower micrognathia;
- prognathia combined with lateral compression.
According to Angle, there are two subclasses of pathology. The first implies a narrowing of the alveolar process on the sides, a fan-like divergence of the incisors from above. The second subclass is characterized by the deviation of the lateral incisors outward, and the central ones towards the palate. And also their rotation along the axis, the absence of a middle gap between them.
Signs of occlusion pathology
In most cases, it is impossible to determine the “correctness” of the bite visually. This can be done by an orthodontist, who is highly advisable to see the child annually, from the eruption of baby teeth to the completion of the formation of a permanent bite. A specialist can identify an emerging problem, and even the prerequisites for the fact that the bite may be formed incorrectly.
For example, crowding of baby teeth significantly complicates the process of eruption of permanent teeth. Molars are larger than primary teeth, so they generally need more space in order to occupy the correct position in the dentition.
When examining a child’s teeth, parents are unlikely to be able to assess the symmetry and uniformity of jaw development and the correct placement of teeth in the dentition. But there are other manifestations, the presence of which may indicate problems with occlusion or a predisposition to the development of orthodontic anomalies:
- Incorrect breathing. We can breathe through our mouths if, having caught a seasonal ARVI, we suffer from a runny nose. This is fine. It is a completely different matter if the child breathes through his mouth all the time out of habit or due to the presence of enlarged adenoids.
- Snore. Children can snore in their sleep only if there are serious disorders in the development of the dental system. This feature, unusual for childhood, should not be left unattended. Not only can you miss the best time to correct your bite, but during sleep apnea the brain does not receive enough oxygen, which can affect the mental abilities of a growing person.
- Certain facial features. What matters is the structure and proportionality of the lower third of the face. The chin should not be too massive, nor, on the contrary, sloping back. The upper jaw should also not be the most protruding part of the face, as this indicates its hypertrophy.
- Posture disorders. Changes in bite due to scoliosis and other disorders in the musculoskeletal system can develop as a compensatory reaction of the body, which needs to develop coordination of movements and the ability to maintain an upright body position at any cost.
Preventing abnormal jaw development
Long-term treatment can be avoided if changes are identified in time and preconditions for abnormal development are eliminated. To do this you should:
- wean the child from bad habits;
- promptly treat acute respiratory infections and ENT pathologies (rhinitis, adenoids, tonsillitis), avoiding frequent and prolonged mouth breathing;
- introduce solid foods in a timely manner;
- monitor posture and correct seating at the table (without asymmetry of shoulders, shoulder blades and other deviations);
- eliminate the usual incorrect position of the body and head during sleep (high headboard or tilting the head back).
A forward thrust of the lower jaw can cause unpleasant consequences, but fortunately, it can be corrected. The younger the patient, the easier it is to return the protruded jaw to its place, so it is better not to delay treatment. Adults will have to prepare themselves for long-term therapy, which requires accuracy and discipline, or for a complex surgical operation.
Causes of occlusion pathology
The formation of the dental system is influenced by a number of external and internal factors. If it is possible to identify such a causative factor and eliminate it in time, then the correction of violations is much easier and faster. We have combined the most significant reasons into one list:
- Heredity. The presence of occlusion pathology in one of the parents increases the likelihood of a defect forming in the child by 40%. If a pathology in the structure of the dental system is detected in both parents, then you should not expect a miracle. It is better to contact an orthodontist in a timely manner and artificially “direct” the growth of teeth and jaws in the right direction.
- Bad habits. The child actively tastes any objects. There is nothing wrong with this until holding something in your mouth and sucking becomes a habit. Absolutely everything is used: the edge of the blanket, fingers and even lips. Pacifiers do not cause harm only in cases where the child weaned off them in a timely manner.
- Problems of the musculoskeletal system. The bite affects the condition of the spine, primarily the cervical and thoracic regions. And pathology of the musculoskeletal system, for example, flat feet, is a significant factor that can disrupt the normal development of the bones of the facial part of the skull.
Symptoms
There are characteristic symptoms of this disorder, many of which are visible even to a layman.
The following features are distinguished:
- concave (bird-like) profile;
- strengthening the fold between the lower lip and chin;
- protrusion of the upper lip, falling inside the lower one;
- teeth protrude from behind the lip;
- if there is an inward inclination of the incisors, a recession of the upper lip is characteristic;
- relatively small chin;
- breathing through the mouth;
- violation of diction;
- impaired posture and gait;
- stretching the neck forward to normalize breathing;
- the upper jaw is displaced anteriorly;
- the lower one is pushed back.
There are symptoms that are visible only when examining the oral cavity and are not visible at first glance.
Intraoral signs of anomaly:
- inclination of the upper incisors forward;
- moving them forward;
- lack of closure of the incisors;
- the presence of sagittal space between the teeth;
- pathological location of the lateral teeth;
- Gothic sky;
- diastemas;
- three;
- crowding.
Over time, a child with a prognathic bite develops wedge-shaped defects and gum recession. This anomaly is accompanied by other pathologies.
What if the bite is not corrected?
Anomalies of occlusion cause physical and psychological discomfort to their owners. Psychological problems are more significant for children and adolescents, as crooked teeth often become a reason for ridicule. Physical discomfort begins already in adulthood, when the body's resources are depleted. Improper distribution of the load when chewing leads to problems in the temporomandibular joints, rapid abrasion of enamel, and periodontal diseases. Accelerated tooth decay requires expensive prosthetics at a much earlier age than would be the case in the absence of occlusal anomalies.
Duration of treatment
The duration of correction is largely determined by the age of the patient. However, you must immediately prepare yourself for several months of wearing orthodontic structures. During the period of mixed dentition, children will have to wear special devices for a year and a half. In adults, wearing braces may take several years to obtain lasting results. However, a person quickly gets used to any devices and stops feeling them. And you shouldn’t refuse correction, since prognathia can lead to serious problems in the foreseeable future.
Complications
This is a rather severe pathology of the dental system, and its consequences can lead to serious complications.
The following problems arise:
- diseases of the gastrointestinal tract due to problems with chewing food;
- active caries damage;
- periodontal pathology;
- dysfunction of the maxillary joint;
- disproportionate formation of the facial skeleton;
- breathing disorders.
All these anomalies provoke psychological problems and complexes in the child. This makes it difficult to communicate with peers, as well as the processes of socialization.
Diagnostics
The wide variety of forms of the anomaly often complicates the diagnostic process. In order not to make a mistake in making a diagnosis, in addition to visual examination, several research methods are used.
These include:
- Pon's method . Allows you to determine the relationship between the width of the mesiodistal fragment, which includes 12 teeth, and the width of the jaw arch;
- Howley-Herbst diagram . Helps to identify the degree of narrowing;
- anthropometric analysis . It is made using models made of plaster to identify abnormal areas and the degree of occlusion;
- teleradiography . Designed to determine the nature and type of narrowing;
- radiography . Aimed at studying the area of the palatal suture: determining its structure and width;
- orthopantomography . Used to obtain a general picture of the condition of the jaw and study the structure of its tissues.
In addition, external and functional characteristics are taken into account.