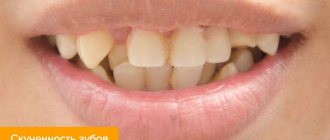
Polyodontia is an anomaly in the development of the dental system, characterized by the appearance of many primary or permanent teeth. Supernumerary teeth often grow in the upper jaw. They can be small in size and cone-shaped. There are also additional teeth of drop-shaped, chisel-shaped forms.
Even one supernumerary tooth can cause a lot of inconvenience, and not only aesthetic ones: its appearance can lead to bite defects and significantly increases the likelihood of developing multiple caries due to crowding and hygiene problems.
The presence of several extra teeth aggravates the problem. This phenomenon leads to the inability to chew food normally. Incorrect distribution of the chewing load may cause insufficiently long service life of normal, complete teeth. In addition, due to a larger number of teeth, speech defects are often observed - it becomes simply impossible to pronounce some sounds. Therefore, it is important to consult a dentist with such a problem.
Causes of hyperdontia
Researchers have not figured out the exact reasons for the appearance of extra teeth. But there are several hypotheses that explain the pathology. Normally, the primary bite includes 20 teeth, and the permanent bite includes 28-32 teeth. The presence of one extra tooth may indicate a defect in a specific gene that has not yet been identified.
Anthropologists claim that our ancestors had more incisors on the upper and lower jaws. Supernumerary teeth can now act as a kind of atavism.
The influence of pathogenic factors during pregnancy can also cause an increase in the number of teeth in a set. The hereditary mutation is that more teeth are formed from the dental plate during embryonic development - it is split into a larger number of tooth germs.
It is important to know that there are many reasons for an increase in the number of teeth. This phenomenon is observed in some congenital syndromes:
- cleidocranial dysplasia;
- Rothmund-Thomson syndrome;
- adenomatous polyposis of the colon.
Therefore, sometimes such a symptom is a reason to contact not only a dentist, but also specialists of another profile, for example, a geneticist or gastroenterologist.
Ask a Question
After removal of a recumbent wisdom tooth
While the anesthesia is in effect, the patient does not feel pain. But when the effect of the drug wears off, sensitivity gradually returns, and the person begins to feel pain. This pain is physiological, because the doctor cut the tissue, touched the bone, and the nerve endings were damaged. After a few days, the sensations finally subside. The following symptoms are possible:
- Mild hyperthermia;
- General malaise, weakness;
- Development of edema;
- Bleeding in the socket area.
Sometimes bleeding from the site of tooth extraction frightens a person; this is a natural reaction. The patient always thinks that he has lost more blood than actually happened. Sometimes the phenomenon continues for hours and usually stops completely by the evening. But if the nature of the bleeding remains unchanged throughout the day, the pain increases, and purulent spots appear in the socket, then the discomfort cannot be tolerated. This requires quick response measures to stop the developed inflammatory process.
Symptoms of hyperdontia
Polyodontia usually manifests itself during one of the following age periods:
- Newborn. The pathology is detected during the first examination of the child; a neonatologist may detect an erupted tooth in the oral cavity or suspect an abnormal development of the jaw.
- From 4-7 months to three years, during the formation of the primary occlusion.
- From 5−7 to 18−25 years during the formation of permanent dentition.
The extra tooth is usually located in the midline of the face, between the central teeth. It is characterized by its small size, shortened root system and conical crown, tapering closer to the cutting edge. However, in some cases, the size and shape of the crown are completely normal.
The second most common option is an extra fourth molar. It may correspond to the normal size of a regular chewing tooth or be smaller.
An additional unit of dentition can erupt anywhere or remain in the thickness of the bone tissue in the form of a rudiment. Cysts often form in the area of such unerupted teeth. This process is not characterized by pronounced symptoms, so the pathology is discovered by chance, as part of a diagnosis carried out for another reason. The best way to make a diagnosis in this case is radiography.
A decrease in local protective forces can lead to exacerbation of periodontitis, swelling of the gums, redness of soft tissues, and the formation of fistulous tracts with the contents of the cyst being released. This is one of the common complications of unerupted supernumerary teeth.
There are other possible consequences of the anomaly:
- retention and dystopia - impossibility of eruption of a normal tooth, change in its normal position (eruption at an angle, rotation of the incisor along the axis, etc.);
- diastemas, trema: gaps between teeth, central incisors;
- anomalies in the position of the teeth, including their location in the palate, displacement towards the cheeks;
- discrepancy between the sizes of the dentition and jaw, which leads to crowding and bite defects.
Long-term consequences of this phenomenon include tooth decay due to caries or excess pressure due to lack of space in the jaw.
Varieties of polyodontia
There are several forms of polyodontia in humans:
- Atypical. The extra units do not grow in the alveolar socket or even within the dentition. For example, a tooth germ can form in the body of the palatine bone.
- Typical. A supernumerary tooth grows within the dentition. This happens more often with small sizes of the dental unit, when there is enough space for it in the row.
- False. Delay in the rate of change in the primary occlusion. The rudiments of permanent teeth erupt when the milk teeth have not yet fallen out. They can erupt behind, in front and even outside the dentition.
- True. Formation of the rudiments of supernumerary teeth, in which the location of the tooth may not be limited to the dentition.
A separate category is genetic diseases, in which supernumerary teeth are often formed. These include cleidocranial dysplasia, when there are defects in the development of the skull bones, complete or partial absence of the clavicles. It provokes dental anomalies and adenomatous polyposis of the colon - the appearance of multiple polyps in the large intestine. Rothmund–Thomson syndrome is also characterized by multiple pathologies, including skin, nails and teeth.
Teething order
The timing of the replacement of baby teeth with permanent ones is approximately the same for all children. Molar teeth emerge at the age of 5 years, when the first large molars appear. Next, the replacement scheme approximately corresponds to that for the eruption of baby teeth:
- First, the central incisors on the lower jaw are replaced.
- Then the upper central and lower lateral incisors are cut approximately simultaneously.
- By the age of 8-9 years, the lateral incisors of the upper jaw begin to change.
- At the age of 9-12 years, premolars (small molars) change.
- At about 13 years of age, the canines change.
- After 14 years, the second large molars, which were not in the milk set, erupt.
- From the age of 15, large third molars, called “wisdom teeth,” may appear. But there are often cases when, even in old age, such teeth do not erupt and remain in the gums.
»
Possible complications with polyodontia
The most common consequence of polyodontia is an unaesthetic smile, facial disproportions, as well as impaired diction, usually a lisp. In especially severe cases, extra teeth are noticeable even at rest, when the mouth is closed. Lips may protrude unnaturally or jaws may not close properly.
Additional teeth put pressure on the complete ones and take up space in the dentition. Teeth can shift, rotate along an axis, be located outside the row - on the palate, under the tongue, etc. Supernumerary units of the row cause crowding of the teeth. This complicates hygiene, provokes the accumulation of plaque, the formation of tartar, multiple caries and complications in the form of pulpitis and periodontitis.
When crowding occurs, the tissue around the teeth does not form correctly. In addition, the chewing load is distributed incorrectly. This can cause diseases of periodontal tissues - gingivitis, periodontitis, periodontal disease, in which deep periodontal pockets are formed, tooth mobility and further loss are observed. When overcrowding occurs, normal prosthetics are almost impossible without prior orthodontic treatment.
This disease leads to functional disorders, cosmetic defects, and therefore is one of the causes of self-doubt and interferes with normal communication and adaptation in society.
Useful tips
Before removing an incorrectly positioned wisdom tooth, we offer a number of tips that will help you prepare and go through the operation more comfortably:
- Try to make an appointment for tooth extraction in the morning. During the night, the hormone cortisol accumulates in the body, which helps to survive stressful situations. In addition, one should take into account the fact that the inevitable bleeding from the wound at the site of the former tooth will stop by the evening, and the person will be able to sleep peacefully.
- Eat well before surgery. As a result, saliva will be released in smaller volumes, and then you will need to leave your jaws alone and not eat for some time.
- If possible, immediately use a cold object and periodically apply it to your cheek on the way home to prevent swelling from forming. A pack of dry ice from a motorist's first aid kit will do.
- At home, rinse your mouth with clean water or medications recommended by your doctor.
- Take medications in the correct dosage, do not get carried away with self-medication and self-prescription of drugs.
Recommendations for a better rehabilitation period after removal of an impacted wisdom tooth:
- You will need to allow a blood clot to form at the site of the extracted tooth. His presence is mandatory. The clot protects the socket from the penetration of bacteria and prevents complete deformation of the gums. Dry socket is dangerous and provokes inflammation.
- Do not touch the blood clot with your tongue, toothbrush bristles, or cutlery. It is not even recommended to use mouth rinse for 2-3 days after surgery. It is better to take the medicine into your mouth, hold it for a while and spit, avoiding the chance of dislodging the clot.
- To stop bleeding, it is permissible to use sterile cotton wool or gauze swabs. It is allowed to moisten with Chlorhexidine, Miramistin. It is prohibited to use hydrogen peroxide!
- For several days you will have to eat soft food and maintain an acceptable temperature of food and drinks.
- You are supposed to temporarily give up physical activity and training. Baths and saunas, swimming pools, solariums are prohibited.
- You cannot heat the surgical area, as this will cause a dangerous inflammatory process. You can apply ice, but under no circumstances keep it on your cheek all the time. Optimal rhythm: 5 minutes cooling, 5 minutes break. If you don’t have ice at home, bags of frozen vegetables and meat from the freezer will do.
- Maintaining oral hygiene is not prohibited. The main thing is to leave the operated area alone in the first days and not try to thoroughly clean the teeth located near the wound. Disinfection can be carried out with solutions of Chlorhexidine, Furacilin, holding it in the mouth and spitting it out, without rinsing.
Medicine knows of cases when wisdom teeth are prescribed to be preserved. But if it grows, pushing neighbors, lies horizontally or rests on the roots of nearby teeth, there is no need to think twice. Such an eight is considered problematic and is deleted without regret.
If a wisdom tooth grows horizontally and puts pressure on the adjacent tooth
Removal of wisdom teeth using ultrasound in Moscow without pain and complications
Diagnosis and treatment
High-quality and timely diagnosis allows you to prevent possible complications and take timely measures to eliminate the problem. Most often, extra teeth are located in the anterior part of the upper jaw. The more accurately the position of the units is determined, the better the surgical treatment will be.
In children, removal of supernumerary teeth is carried out as carefully as possible to avoid damage to the growth zones of complete teeth and the formation of bone defects in the alveolar process. Therefore, radiography is performed - it allows you to determine the position of the teeth, features of the root system, and evaluate the relative position of units in the thickness of the jaw bone.
The following diagnostic methods are used:
- CT;
- Orthopantomography (OPG);
- targeted image - intraoral radiography (when assessing the condition of one or two teeth);
- MRI.
CT allows you to obtain a layer-by-layer image of bone structures in a matter of minutes. The method is relevant when it is necessary to obtain an image of a tooth in different planes. The radiation dose in this case will be safe, and the procedure is easily tolerated by most patients and does not require any preparation.
Orthopantomography (OPG) is a method that involves performing a panoramic image of the entire jaw, as well as adjacent tissues and structures of the facial skeleton. Can be performed on patients aged three years and older. This is a quick, simple and very informative method that helps to get a general idea of the condition of the dental system. If you suspect multiple supernumerary teeth, as well as when planning orthodontic treatment, it is especially relevant.
Intraoral radiography is the simplest and most popular diagnostic tool. The image can provide an image of 1-4 teeth, depending on their size, as well as the structures adjacent to them. When identifying many extra teeth, this method will be less effective, but can be used if it is impossible to use others.
It is also used as part of surgical treatment planning if supernumerary teeth are removed one at a time. An accurate determination of the relationship of the additional unit with the root systems and rudiments of normal teeth is carried out using intraoral radiographs before surgery and some time after it. Using this method, it is possible to determine the degree of changes in the position of the impacted tooth, the condition of the roots of complete teeth, the structure and condition of the bone in the area under study.
It is also used as part of surgical treatment planning if supernumerary teeth are removed one at a time. An accurate determination of the relationship of the additional unit with the root systems and rudiments of normal teeth is carried out using intraoral radiographs before surgery and some time after it. Using this method, it is possible to determine the degree of changes in the position of the impacted tooth, the condition of the roots of complete teeth, the structure and condition of the bone in the area under study.
Other situations
Sometimes after tooth extraction a phenomenon called ecostosis occurs. After tooth extraction, the edge of the gum settles, causing part of the bone to protrude to the surface. Many patients may mistake a piece of bone for a tooth fragment. Ecostosis can be easily eliminated using the usual grinding procedure, so there is practically nothing to worry about in this case. Sometimes part of the bone material may come out of the hole, which is replanted with the patient before implantation if the height and volume of the native bone is not enough. Sometimes small pieces of bone material may come out through the sutures, but this is also not considered a serious complication.
Treatment of polyodontia
If hypodontia - fewer teeth than normal - requires the restoration of missing units, then with supernumerary teeth the approach may be the opposite. There are standard protocols for providing care in each case. The only correct approach is complex treatment, and the tactics of surgical, orthopedic, and orthodontic treatment are determined individually. Not only the number and relative position of extra teeth are taken into account, but also the rate of jaw growth and development of the dental system.
Treatment is possible only with a collegial approach; it is carried out by a whole team: a dental surgeon, an orthodontist, an orthopedic dentist. For children, a pediatrician or neonatologist is involved in developing a treatment program. Sometimes the help of an oral and maxillofacial surgeon is required.
There are two main areas of treatment: surgical and orthodontic. Surgical intervention is indicated in all cases where an extra tooth affects the formation of the bite. Removal may be complicated by the fact that it does not erupt completely, is located close to the root systems of complete teeth or to the rudiments, the maxillary sinus of the upper jaw or the mandibular nerve of the lower jaw. Therefore, after removal in children, it is important to monitor the condition of the little patient for another year.
It is recommended to remove additional teeth from the age of 8, during the period of change of the frontal group of teeth. This will prevent dental deformation and malocclusion. Only if there is a high risk of damage to a normal tooth germ in close proximity, the doctor will recommend postponing the operation.
With false polyodontia, removal of baby teeth usually does not cause problems. The root systems of such teeth are already resorbed in most cases, and the risk of complications is extremely low.
The type of operation is determined by the location of the tooth, the degree of its adherence to the complete teeth, the depth of its location in the bone tissue, age characteristics and other factors.
Orthodontic treatment is also determined by the specific situation. It is usually used after the surgical stage, if the additional tooth has already had a certain effect on the bite. Functional devices can be chosen as a correction method: plates, aligners, and braces.
Making a butterfly prosthesis
This method of prosthetics is the least reliable and comfortable. Therefore, such a prosthesis can be exclusively temporary. It solves aesthetic problems, but not functional ones. A removable denture is made of acrylic (plastic) or nylon. It has many disadvantages: the prosthesis is mobile, impairs diction, sometimes there are allergic reactions to the material from which it is made, it is not functional - it restores chewing function by less than 50%, and wears out quickly. But it is the most inexpensive. Therefore, the best use is to temporarily close the defect while the implant heals.
Prognosis and prevention
There is no specific prevention of hyperdontia, since the exact reasons for the appearance of additional units of the dentition are unknown. You can only prevent the consequences of false hyperdontia - it is important to monitor the rate of change in the primary occlusion and take action if the primary tooth does not fall out in due time.
Most often, the prognosis for treatment is favorable. Modern possibilities will allow you to restore the aesthetics of your smile and the function of your teeth. The main treatment tactic is the removal of excess row units and subsequent correction of the position of the remaining teeth. In childhood, it is usually possible to get by with removable orthodontic appliances. Adults are most often recommended to wear braces and the subsequent retention period (wearing retainers).
It is advisable to preserve supernumerary teeth only if they are capable of bearing the load during planned orthopedic and orthodontic treatment, can be a full-fledged unit of the dentition, and can replace complete teeth that cannot be restored due to their severe destruction by trauma or caries. The decision on the treatment method is made by a team of dentists from different fields.
You can get qualified help from dental surgeons, orthodontists and orthopedists for hyperdontia at the STOMA clinic. To schedule a consultation, call the number provided or fill out a special form on the website.
How are baby teeth different from molars?
A human tooth consists of three main parts: the visible part (crown), the root, which is recessed into the gum tissue, and the neck, located between them. Despite the fact that the general structure and functions of primary and permanent teeth are similar, there are still differences between them:
- the surface shade of temporary teeth is white, while permanent teeth are yellowish;
- the tissues of the molars are denser and harder, and the pulp is much larger;
- the shape of the milk teeth is flat and wide, the molars are quite long (the width is significantly less than the length);
- The roots of baby teeth are thinner and shorter than those of permanent teeth.
During the process of loss of temporary teeth and the appearance of permanent teeth, the child’s jaw actively grows, and by the time it ends it reaches an adult size - thanks to this, 32 permanent teeth grow in place of 20 temporary teeth.