- Crooked teeth
- The appearance of a second row of teeth in the jaw
- When permanent teeth do not appear for a long time
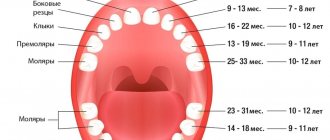
- How to distinguish baby teeth from permanent ones?
The complex process of replacing baby teeth with permanent ones is often painful and accompanied by a number of problems. The most common of them is malocclusion. The second most common problem is the appearance of a second set of teeth. Also, many parents are faced with the fact that their child’s molars and incisors do not appear for a very long time.
Crooked teeth
If permanent teeth begin to grow unevenly, you need to come for a consultation with an orthodontist at the A-Medic Network of Medical Clinics as soon as possible. The sooner such a decision is made, the easier it will be for the dentist to correct their growth. An incorrect bite is not only inconvenient, it can lead to the development of a number of diseases, for example, caries, stomach diseases, and cause childhood and teenage complexes and psychological problems.
The easiest way to straighten your jaw is to wear braces. It is very important for parents, together with the attending physician, to explain to the child that temporary inconveniences when using braces are justified and will bring invaluable benefits in the future. You need to take good care of it, because it will stay in your mouth for at least six months. This design will work most effectively during adolescence. Small children can more easily tolerate plates or trainers, which look something like boxing mouthguards, rather than braces. Children's enamel is quite delicate, so trainers that do not damage it will be the best way to correct a child's malocclusion.
What should mom do?
When teeth erupt out of order, every parent should take this fact seriously. Pediatricians advise feeding your baby in a balanced manner. For six-month-old children, mother's milk is not enough. Complementary foods should be introduced gradually. Mothers should properly allocate time for wakefulness and sleep, and visit the doctor according to the schedule. A vitamin complex may be prescribed. It is prohibited to select medications on your own, since only a doctor can give an objective assessment of the baby’s condition.
If the chewing organs do not appear according to the calendar, specialists prescribe certain tests to determine the cause of the failure. Mom should not neglect the doctor's recommendations. Its instructions should be followed exactly to stimulate the appearance of units. To do this you need:
- Include foods rich in vitamins in your diet;
- Correctly create a daily routine and monitor its implementation;
- Conduct comprehensive physical exercises with children;
- Regularly visit a doctor for preventive purposes;
- Treat illnesses in a timely manner;
Taking medications without a doctor's recommendation is dangerous and detrimental to a child's health. Only care and affection, proper care and feeding will allow you to raise a healthy child.
The appearance of a second row of teeth in the jaw
Each canine, incisor and molar has its own place, but sometimes a child's permanent teeth begin to form a second row. This often happens when the milky ones have not yet fallen out, but the radical ones have already begun to appear. An undeveloped jaw that provides too little room for growth can also be a source of the problem. The third reason is that the incisors and canines in the second row are “superfluous”, or supernumerary.
The second row of teeth is not only inconvenient, but also unsightly, so the problem needs to be solved. A baby tooth that does not fall out in time can be removed in the clinic. If the reason for the formation of the second row is underdevelopment of the jaw, then the dentist can remove several teeth and install braces on the remaining ones.
Difficulty in teething is a relatively broad concept. These include congenital dental malformations associated with dental anomalies; diseases of the teeth, jaws and oral mucosa, causing pathological phenomena during tooth eruption.
Tooth retention is a delay in eruption, refers to tooth development defects, but can sometimes be associated with diseases and damage to the dental system.
Tooth impaction is more often observed during the eruption of permanent teeth. The most common cases of impaction are the upper canines, second lower molars, and lower wisdom teeth. Tooth retention can be complete (the tooth is located in the bone tissue) or incomplete.
Incomplete retention (half-retention) is the partial eruption of a tooth. In this case, the tooth is called semi-retained, or semi-retained.
Dystopia is an abnormal position in the dentition of a fully erupted tooth or the tooth has erupted outside the dentition. This most often occurs as a result of a violation of the sequence and timing of teething, and therefore the teeth occupy the wrong position.
The timing and nature of teething in children are criteria for the child’s development.
Impacted teeth can lead to disruption of the normal position of neighboring teeth, that is, their displacement in the vestibular or oral direction is determined.
Inflammatory phenomena in the area of an impacted tooth can give a picture of periodontitis of the adjacent tooth, which in turn causes acute periostitis of the jaw, acute osteomyelitis of the jaw, inflammatory processes in the perimaxillary soft tissues - abscesses, phlegmons, lymphadenitis.
Inflammatory phenomena that occur in the area of the impacted tooth and in the surrounding tissues can sometimes be associated with the spread of infection from a neighboring infected tooth.
Sometimes a follicular cyst develops in the area of the impacted tooth, which is manifested by deformation of the alveolar process or even the jaw (swelling), and when the cyst suppurates, various inflammations occur. It is also possible for a follicular cyst to develop unnoticed by the patient when it is detected during an X-ray examination.
Half-retention is observed more often than complete retention. It often leads to inflammation. In these cases, you can find part of the erupted tooth crown in some vestibular part of the alveolar process, on the hard palate, behind the last large molar. As a result of constant trauma to the mucous membrane adjacent to the erupting part of the tooth crown, inflammation occurs.
In the clinic of surgical dentistry, difficult eruption of the third lower molar is often observed.
The reasons for difficult eruption of the lower wisdom teeth are varied. Thus, there is a disruption of the normal development of the lower jaw and a decrease in the size of the distal part of the alveolar process. Due to this, the lower wisdom tooth does not have enough space in the alveolar process.
Difficult eruption of the lower molar can be caused by its dystopia, due to which it is deprived of its correct position in the dentition.
When the lower third molar erupts, the medial cusp or cusps may first erupt, the rest of the crown remains covered by a hood of the mucous membrane, or the entire crown of the tooth is covered by such a hood. Due to chronic inflammation in this area of the mucous membrane, scarring occurs, which makes further tooth eruption difficult. In these cases, food debris accumulates under the hood of the mucous membrane, creating favorable soil for the development of microorganisms. Inflammation occurs here as chronic marginal periodontitis and gingivitis, pericoronitis. Inflammation may be associated with the occurrence of erosions and ulcerations on the mucous membrane covering the hood above and below.
Clinic. Complete tooth retention often remains asymptomatic and is discovered incidentally during an X-ray of the jaw.
Tooth retention is indicated by the absence of one of the permanent teeth in the dentition; in its place there may be a temporary tooth. In some cases, impacted teeth create a protrusion of the outer wall of the alveolar process or the body of the jaw. In this case, sometimes you can palpate the contours of the tooth or part of it.
With inflammatory complications, patients often complain of pain in the area of the impacted tooth. In some cases, complaints of pain are a symptom of nerve damage - neuralgia or neuritis due to pressure, impaired trophism. In some cases, tooth impaction can cause paresthesia.
Semi-retention, or difficult eruption of the lower molar, is accompanied by periodic pain, sometimes very intense, which is associated with inflammation of the mucous membrane (hood) covering the crown of the tooth (pericoronitis). Pain is noted in the area of the causative tooth, sometimes radiating to the ear and intensifying when chewing. Sometimes there is pain when swallowing. The disease may be accompanied by a rise in temperature to 37.5-37.8°C. An objective examination reveals enlarged and painful lymph nodes in the distal part of the submandibular triangle, sometimes fused into a conglomerate.
Mouth opening is usually limited and painful due to the spread of inflammation to the area of the masseter or medial pterygoid muscle. The degree of restriction in mouth opening may indicate the degree of involvement of the masticatory muscles in the process.
When examining the oral cavity, the picture varies. The medial cusps of the wisdom tooth are visible, the rest is covered with a swollen, hyperemic hood of the mucous membrane. Pressing on it significantly increases the pain. A drop of pus or bloody-purulent fluid is released from under the hood. Inflammatory phenomena in other areas of the surrounding mucous membrane are expressed differently. Characteristic is the appearance of inflammatory swelling along the pterygomaxillary fold, followed by the spread of edema to the anterior palatine arch.
The wisdom tooth can be located in different projections in the alveolar process. More often the crown moves to the buccal side, less often - to the lingual side and the tooth is always tilted forward.
In some cases, the entire wisdom tooth is covered with a hood of mucous membrane, and only by lifting it can you see the crown of the tooth. Inflammatory phenomena developing in the tissues around the tooth largely depend on the density of the hood and its edge, and the possibilities of outflow of purulent exudate from under it.
When the tooth is tilted forward over the mucosal hood, the distal portion of the crown can be seen, and the mesial portion of the crown faces downward and is adjacent to the lower second molar.
The X-ray image determines the position of the third lower molar, the change in bone tissue in its circumference, and its relationship to the mandibular canal. Characteristic is the expansion of the periodontal line at the neck of the tooth, as well as the often detected rarefaction of bone tissue behind the crown in the form of a crescent.
Treatment of pericoronitis depends on the severity of inflammatory phenomena, the general and local picture of the disease, as well as on radiological data.
The most effective way is to dissect the hood covering the crown of the tooth or its distal part, followed by washing and draining the wound. Excision of the hood is advisable in the absence of acute inflammatory phenomena.
In case of acute inflammatory phenomena in the area of the third molar, treatment should consist of creating a maximum outflow of pus from under the hood. This is achieved by washing the gap between the overhanging mucous membrane and the tooth crown with antiseptic solutions and moving the hood away with iodoform gauze or a tampon soaked in an antibiotic emulsion.
A good therapeutic effect is achieved by blockade of the type of conduction and infiltration anesthesia, often repeated (it is advisable to infiltrate the tissues surrounding the third molar with an anesthetic with antibiotics, furacillin, a proteolytic enzyme). Analgesics and oral desensitizing drugs are indicated. Thermal procedures are prescribed in the form of mouth baths, rinses, inhalations; physical methods of treatment - UHF, microwave therapy for 5-7 procedures. For inflammatory swelling of the perimandibular soft tissues and symptoms of lymphadenitis, external ointment dressings, Sollux, and light external heat are indicated.
The surgeon's tactics in cases of tooth impaction without pronounced symptoms of inflammation may be different. By comparing the indicators of the patient’s general condition, his age, the location of the impacted tooth and the traumatic nature of the upcoming operation, as well as the risk of complications, the feasibility of such an intervention is determined. In the absence of patient complaints and complications associated with tooth retention, tooth extraction surgery is not indicated; dynamic monitoring of the patient is possible.
If there is a significant change in the position of the tooth, when its eruption is impossible, tooth extraction is indicated. If the lower wisdom tooth is positioned correctly and its eruption is beyond doubt, then preservation of the tooth and appropriate therapeutic measures (excision of the hood) are indicated.
In case of pain in the area of the impacted tooth or follicular cyst, as well as in the inflammatory process, the impacted tooth is removed.
The operation of removing impacted and semi-impacted teeth presents certain difficulties. Before the operation, it is necessary to determine the location of the tooth in the thickness of the bone tissue, its relationship to various formations: the edge of the lower jaw, the mandibular canal, the maxillary sinus and nasal cavity, and to neighboring teeth. To determine the location of an impacted or semi-impacted tooth, an X-ray examination should be done, sometimes in several projections. The surgical technique for removing impacted and semi-impacted teeth can be different. Conventionally, tooth extraction in the upper and lower jaw is divided.
Extraction operations are performed on the upper jaw (incisors and canines, small molars and wisdom teeth).
Operation to remove incisors and canines on the upper jaw . Two converging incisions are made from the transitional fold to the alveolar process, to the location of the crown of the impacted or semi-impacted tooth. The flap should cover the boundaries of the tooth. After detachment of the mucoperiosteal flap, the bone tissue located above the tooth is removed using a drill.
The tooth is removed using an elevator (or forceps). If, during tooth extraction, the apex of the root of one of the adjacent teeth is exposed and the neurovascular bundle is disrupted, then resection of its apex with retrograde filling of the apical part of the canal is indicated. The bone cavity after tooth extraction should be handled carefully so as not to perforate the nasal mucosa.
Removal of semi-impacted incisors and canines presents particular difficulties when the tooth is located in the anterodistal direction, i.e., the apex of the tooth root is adjacent to the mucous membrane of the transitional fold, and the crown is located on the palatal surface of the alveolar process. With this arrangement, the tooth is removed after sawing it into two parts; each part is removed separately.
When removing incisors and canines located on the palatal surface of the upper jaw, the incision is made from the side of the hard palate, forming a trapezoidal, semi-oval or angular flap. Having tilted it, using a bur, the tooth is freed from the bone and removed using elevators or forceps.
The operation of removing the upper small molars. Here one should take into account the possible proximity of the tooth to the bottom of the maxillary sinus. The incision is made from the vestibular side, the same as when removing incisors and canines.
Using a drill, the bone tissue surrounding the tooth is removed, then it is carefully removed using an elevator or forceps. If the integrity of the maxillary sinus is damaged, the postoperative wound should not be washed. The perforation hole is tightly sutured.
When the neurovascular bundles of the roots of adjacent teeth are exposed, they are retrogradely filled and the root apices are resected.
The operation of removing the third upper molar. An incision is made on the alveolar process at a right angle, the mucoperiosteal flap is peeled off, after which the tooth is carefully removed using forceps or an elevator. When a part of the tubercle of the upper jaw is broken, the sharp edges of the bone are smoothed and sutures are placed on the mucous membrane.
The operation of removing teeth in the lower jaw is determined by their location, relationship to the mandibular canal, mental foramen, roots of adjacent teeth and the edge of the lower jaw.
When the tooth is located in the area of the alveolar process, the upper part of the jaw body, the incision is made from the oral cavity from the vestibular side. This is usually a trapezoidal, semi-oval or angular incision. Having folded back the mucoperiosteal flap, the bone is removed with a bur, freeing the tooth from it. We must remember about the exit of the neurovascular bundle from the mental foramen and preserve it when peeling off the mucoperiosteal flap. After removing the bone tissue covering the tooth, it is removed using an elevator or forceps.
When impacted teeth are located closer to the edge of the lower jaw, they are removed extraorally.
The incision is made parallel to the edge of the lower jaw, departing from it by 2-2.5 cm. By dissecting the soft tissue layer by layer, the bone tissue of the jaw is exposed. It is trepanned at the location of the tooth. Then it is loosened and removed with straight, bayonet-shaped forceps or an elevator.
The operation of removing the third lower molar. For certain clinical and radiological indications, this intervention is performed in a hospital setting.
So, for example, when an impacted wisdom tooth is located in the middle or upper third of the jaw branch in a hospital setting, an incision is made in the submandibular region and after crossing the masticatory muscle, the soft tissue is peeled off with a rasp.
In the area where the impacted tooth is located, the bone tissue covering the impacted tooth is removed using a drill. The tooth is removed using an elevator. The wound after tooth extraction is sutured layer by layer with catgut, and sutures are placed on the skin with hair.
When the tooth is located closer to the alveolar process, the operation is performed intraorally
An incision is made in the mucous membrane along the alveolar ridge above the impacted tooth and a second one is made from the neck of the second large molar downward and obliquely forward.
A triangular mucoperiosteal flap is folded back. The bone tissue of the outer wall of the alveolar process is removed. Sometimes it is necessary to remove not only the bone from the vestibular surface, but also the overhanging areas of bone over the tooth. After tooth extraction, the mucous membrane is sutured with catgut.
Complications. Depending on the development of inflammatory phenomena in the area of the erupting lower wisdom tooth, a number of complications may arise; acute purulent periostitis, abscesses and phlegmon of the maxillo-lingual groove, pterygo-maxillary and peripharyngeal space (Fig. 54).
Less commonly, the purulent process spreads to the bone tissue and osteomyelitis of the angle and branch of the lower jaw occurs.
When a purulent infection spreads to the retromolar area, acute purulent periostitis occurs (retromolar periostitis). There is an inflammatory swelling of the soft tissues of the lower part of the parotid-masticatory, distal part of the submandibular region on the corresponding side.
Mouth opening is limited, pain increases when swallowing (dental sore throat). When examining the oral cavity, inflammatory infiltration of the pterygomaxillary fold, anterior palatine arch, transitional fold of the lower jaw at the level of the molars and along the anterior edge of the jaw branch is determined; swelling of the soft palate. The inflammatory process can spread along the external oblique line to small molars or into the maxillo-lingual groove - an abscess occurs in the soft tissues of these areas. The spread of purulent infection is facilitated by loose connective tissue and fatty tissue located in the retromolar triangle and retromolar fossa. The inflammatory process during pericoronitis can spread to other anatomically similar areas - submandibular, parotid-masticatory, buccal, pterygo-maxillary and peripharyngeal space and other areas along the length.
The development of surgical dentistry is constantly reaching new levels; dentists are creating the latest techniques to make operations completely painless and effective. Piezosurgery (ultrasound surgery) is one of the most advanced techniques in dental surgery today. Ultrasonic tooth extraction using the VarioSurg system makes it possible to minimize heating and damage to the bone and surrounding tissues due to the generation of ultrasonic vibrations, affecting only the hard tissues of the oral cavity (bone, tooth). When removing a tooth using ultrasound, the cut is made very thinly and precisely.
3D tomography in dentistry
Cone beam computed tomography – accuracy and comfort
Diagnosis and treatment of a number of dental diseases require an accurate examination. Several years ago, the main diagnostic method was dental radiography, or, more simply, film X-ray. It provides general information, but it does not provide such indicators as bone density, bone level, or precise measurements down to millimeters. A significant disadvantage is also the radiation dose.
Currently, an excellent diagnostic assistant is cone beam computed tomography. It is designed and created to provide information to the physician in great detail of the area being studied. produces precise digital images that are simultaneously panoramic, cephalometric and three-dimensional. This “picture” is the best dental assistant, and not only that.
Precise computer 3D images allow a specialist to examine an object from all sides and magnify the smallest detail, sometimes invisible in a regular photograph.
When permanent teeth do not appear for a long time
The absence of permanent teeth for too long can be due to several reasons: these are the genetic characteristics of the body, their immaturity, and the destruction of tooth germs by some kind of infection.
Only a dentist can determine the true cause. At the A-Medic Network of Medical Clinics clinic, they will take a picture of the jaw, which will show how the child’s permanent teeth are formed. Sometimes they can grow inside the gums. If nothing is visible on the image, the doctor may suggest solving the problem by installing dentures.
How to distinguish baby teeth from permanent ones?
Both molars and baby teeth have a similar structure, but have a number of external differences.
- Thus, milk ones are on average lighter and whiter than permanent ones, which are distinguished by a yellowish enamel tone.
- On average, a molar is larger than its primary tooth.
- Permanent ones have a thicker layer of hard tissue and a less developed pulp.
- Dairy varieties have thinner and shorter roots.
It is important for all parents to remember that both baby and permanent teeth of children must be protected, and any problems that arise in their growth and development must be resolved immediately. Specialists from the “A-Medic” network of medical clinics can help them with this.
Cost of correcting diastema
It is easy to guess that the cost of correcting a diastema depends on the chosen method and the need to use certain materials. The severity of the defect also matters.
In general, the most affordable way to achieve a beautiful smile is cosmetic correction or surgical plastic surgery. Artistic restoration, braces and other methods of correcting the position of teeth will be more expensive, but the cost of these methods remains affordable for most patients. When it comes to mouthguards, their production will be the most expensive.