Changing children's baby teeth to permanent ones is always an exciting time for parents. This process is quite lengthy and often painful for the child, because it can be accompanied by various inflammations and discomfort. To help parents, for a better understanding of the physiological processes associated with the formation of teeth, dentists offer to look at the pattern of loss of baby teeth in children.
Content:
- Why is it necessary to replace baby teeth with permanent ones?
- When do the first baby teeth fall out?
- Which baby teeth fall out first?
- Drop order
- At what age do radical units appear?
- Possible abnormalities in the child
- Why do empty spaces remain unoccupied for a long time?
As the child grows, the baby teeth are replaced by permanent ones. This is a natural process, without which the full functioning of the dentofacial apparatus is impossible. But parents should treat it with the utmost responsibility, since very often violations in the sequence of loss of temporary units cause serious malocclusions that have to be treated in the future.
Deviations in timing and problems when changing teeth
One or another problem with the loss of baby teeth and the germination of molars occurs in at least every tenth child. Fortunately, dentists are ready to correct the bite during the growth stage, remove extra teeth, and even insert an implant if there is no point in waiting for a root one.
Let's look at the main deviations that may cause concern:
"Shark's Mouth"
Sometimes baby teeth do not have time to fall out, but the molars have already grown “second row”. The “shark’s mouth” is not worth admiring. You need to go to the dentist as soon as possible and remove unnecessary temporary teeth, otherwise your bite may be significantly damaged.
Untimely change of teeth
If the first baby teeth begin to leave the baby’s mouth before 5 years of age or after 8 years of age, then this is a deviation from the norm, which means you need to understand the reason. Trauma, caries, ecology, nutrition, congenital problems with bite or other heredity, various infectious diseases, hormonal problems (for example, thyroid disease), as well as diseases due to which the child is at risk for underdevelopment and delay may be to blame. formation of permanent dentition (diabetes, leukemia, immunodeficiency and others).
The molar does not grow in place of the lost milk tooth
There is no need to panic, but it is worth consulting with a specialist. For example, if a molar tooth does not erupt, although the baby tooth has fallen out a long time ago, the reason cannot be determined with ordinary eyes, but an x-ray will help. If there is no tooth germ in the picture, this is called adentia. This problem is extremely rare - the tooth simply has nothing to grow from. The decision will require the help of a prosthetist.
With retention, the germ of a new tooth is present, but it is directed incorrectly or is deep in the gum. All that remains is to wait for the tooth to grow. This problem occurs more often in the lower third molars, as well as in the upper incisors and canines.
With impaction, the tooth cannot come out due to the close fit of neighboring teeth. Here, too, you cannot do without the help of professionals.
We also advise you to consult a doctor if:
- molars appear darkened or grow crooked;
- the order of tooth loss and growth differs significantly from the above graphs;
- the child’s gums hurt and his cheek is swollen;
- baby tooth is corroded by caries;
- a tooth fell out, but blood from the socket does not stop oozing for more than an hour (not to be confused with ichor).
Why is it necessary to replace baby teeth with permanent ones?
The chewing apparatus is improving and developing. In infancy, it is adapted exclusively for the intake of liquid food - breast milk. But closer to six months, you can already see baby teeth in children’s mouths. They allow the baby to get acquainted with the variety of solid adult foods.
There are few temporary teeth - ten pieces in each jaw. This is quite enough for the baby to eat well and talk normally. Closer to primary school age, the jaw grows. She is ready to cope with more serious chewing loads. Then children's incisors, canines and molars begin to wobble. They are replaced by a constant shift.
Molars in children: symptoms of eruption
- Fever. When teething in children, body temperature may rise, usually not higher than 38 degrees.
- Itching and pain at the site where the molar appears. Various gels and ointments, as well as gum massage, will help relieve children from unpleasant sensations.
- Increased salivation and runny nose.
Important!
The growth of molars in children, especially at the initial stage, leads to weakened immunity. Take vitamins and do not forget about preventive visits to the dentist.
Which baby teeth fall out first?
According to the standard pattern for replacing baby teeth, the lower incisors are the first to fall out. They are located in the center of the jaw. They can loosen one by one or almost simultaneously.
Following them, the opposite upper units begin to move. This is why you can often see children five or six years old with a funny toothless smile.
Bookmarking teeth
The formation of baby teeth occurs at approximately 4-6 weeks of fetal development. At the same time, the formation of the fundamental elements occurs much later - during the first months of the child’s life. For this reason, new mothers who are bottle-feeding are strongly recommended to supplement their baby’s diet with calcium. This substance promotes the proper formation of tooth enamel.
At an early age, unprotected baby teeth are extremely susceptible to carious lesions. Parents should monitor this closely, as infection can subsequently cause destruction of permanent teeth. The fact is that the rudiments of permanent teeth are in close proximity to the roots of milk teeth, so as soon as you discover dark spots on your child’s enamel, immediately go to pediatric dentistry.
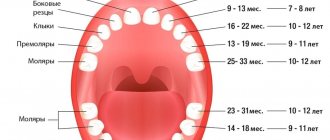
Drop order
The dropout pattern looks like this:
- 5-7 years - central incisors;
- 7-8 - lateral incisors;
- 9-11 - first molars of the upper jaw and second molars of the lower jaw;
- 9-12 - fangs;
- 10-13 - second molars of the upper dentition and first lower ones.
The diagram shows that the timing of changing units is quite arbitrary and quite long. This is why some children already have a permanent bite at the age of ten, while others still walk around at the age of 12 with actively loose baby teeth.
Why can a 7-14 year old child sometimes experience pain when all his teeth are intact?
Yes, this can happen, but in this case the pain occurs not in the tooth itself, but in the jaw, which is growing rapidly at this age. Since permanent teeth are almost twice as large as baby teeth, they need much more space. Therefore, large new teeth can sometimes overlap each other or grow at an angle, getting out of the dentition. As the jaw grows, they align and settle into place. But a qualified specialist can competently assess this situation, as well as the risk of anomalies and developmental defects. That is why in this case you will need to consult an orthodontist.
At what age do radical units appear?
We can talk about adult occlusion only a few years after the start of the change in time units. Typically, a stronger replacement will erupt several weeks or months (or, if pulled out prematurely, years) after the baby teeth fall out.
Central incisors grow from 6 to 8 years of age, lateral incisors from 7 to 9, premolars and canines from 9 to 12. Molars begin to grow at approximately six years of age. They immediately grow permanently, replacing the empty space.
At what age should a bite be corrected?
You can start correcting your bite at 4-5 years of age. In this case, the growth of permanent teeth will be even, in the place intended by nature. Therefore, there is no need to carry out subsequent long-term bite correction. In any case, if there is a malocclusion, the problem can be eliminated efficiently and as quickly as possible by contacting a qualified orthodontist as early as possible.
| Teeth | Dairy (temporary) | Permanent | ||
| Jaw | Lower | Upper | Lower | Upper |
| Central incisors | 6-12 months | 8-12 months | 6-7 years | 6-8 years |
| Lateral incisors | 10-16 months | 9-13 months | 7-8 years | 7-8 years |
| Fangs | 17-23 months | 16-22 months | 9-10 years | 11-12 years old |
| First Premolars | — | — | 10-12 years | 10-11 years |
| Second Premolars | — | — | 11-12 years old | 10-12 years |
| First Molars | 14-18 months | 13-19 months | 6-7 years | 6-7 years |
| Second Molars | 23-33 months | 25-33 months | 11-12 years old | 11-13 years old |
Possible abnormalities in the child
Parents should know when to expect changes in their child's bite . Late change of baby teeth, like premature change, is undesirable. They speak of lateness when an eight-year-old child has not yet lost any of his incisors; they speak of early eruption if a five-year-old child has already lost many of his incisors and fallen out. It is important to find out the cause of the changes occurring and, if possible, eliminate it.
Factors due to which the bite changes earlier than standard periods:
- severe jaw injuries;
- congenital diseases leading to anomalies in the eruption of temporary and permanent units;
- advanced caries, due to which crowns and roots are destroyed faster than necessary.
As for a late shift, it is possible due to:
- rickets, calcium and vitamin D deficiency in the child’s body;
- hereditary characteristics of the dentofacial apparatus;
- some infectious pathologies.
Nutritional Features
In newly erupted permanent teeth, the enamel is not yet fully formed, so it is very important to provide the child with adequate nutrition:
- Your diet should include dairy products or other foods rich in calcium every day.
- You should eat fish twice a week - it contains phosphorus
- It is better to consume vegetables and fruits more often, fresh and in solid form.
- It is better to avoid sweets and white pastries. Also, sodas are very dangerous for fragile enamel.
- Avoid eating toffees, candies, nuts and other chewy or hard foods. It is also better not to eat foods with active dyes, as they can easily change the color of the enamel for life.
Temporary teeth are formed during fetal development and appear in the baby at 5-8 months. When are baby teeth replaced by molars? What to do if they don't fall according to schedule? What should parents pay attention to?
Why do empty spaces remain unoccupied for a long time?
It often happens that a child walks around with a toothless smile for a long time, but the situation still does not change. When examining his oral cavity, the parents do not see even a hint of an imminent full bite. This happens when:
- Retentions. Dental pathology in which a segment of gum tissue is shown very little or not at all. The violation may be complete or partial. In any case, if it occurs, you should consult your dentist. Sometimes the situation can only be corrected through surgery.
- Edentia. The banal absence of a permanent germ. So, for example, a temporary fang falls out, and there is nothing to replace it with. The anomaly can be confirmed using x-ray diagnostics - the images show that the rudiment is missing. Fortunately, congenital adentia is rarely diagnosed in young patients. If it is, only prosthetics will save you.
- Impacts. Difficulties with eruption with this diagnosis are explained by the fact that the crowns of the “neighbors” are too close to each other and do not leave room for the crown, which should be between them. Deviations can also be detected using x-rays.
If there are any problems with the bite, parents should show the baby to the doctor. Moreover, children should have annual checkups at the dentist's office. This simple measure serves as an excellent prevention of serious complications and reduces the likelihood of an unattractive smile in adulthood.
What does the dental formula look like?
The medical record, which the big one keeps in the dental clinic at his place of residence, contains notes about his dental condition. To avoid confusion, doctors number the teeth on each side of each jaw. So, the 1st and 2nd teeth are incisors, the 3rd are canines, the 4th and 5th are small molars (doctors call molars molars), the 6th and 7th are large molars. The 8th - the farthest one - is a “wisdom tooth”; a number of people do not have it, or they do, but not all. Each side of the jaw is also numbered: 1 - top right, 2 - top left, 3 - bottom left, 4 - bottom right. For example, entry 48 does not mean that you are a “Tarkatan” with a combat superset of teeth that does not exist. You simply do not have a “wisdom tooth” on the lower right. Entry 41 - a person lost one of the frontal incisors on the same side on the same jaw. You can write down the formula of the teeth more clearly: for example, “there is no 8th tooth from the bottom right.”
It often turns out that due to lack of space on the jaw, the wisdom tooth develops incorrectly - it can grow crooked, in which case its removal is indicated. For example, it may remain under the gum and, because of this, be affected by caries, which can subsequently develop into pulpitis or a dental cyst. Problematic “wisdom teeth” are quickly and decisively removed, and their absence will not greatly affect the quality of chewing food.
Typical problems
PHOTO: The child's lower permanent incisors erupted in the second row. In this situation, it is necessary to free up space by removing the mobile baby teeth so that the permanent teeth can take the correct position in the dental arch.
Sometimes the permanent upper and lower incisors erupt behind the primary ones (“second row”), which do not have time to resolve by this time. This situation requires the intervention of a dental surgeon.
Progression of previously formed caries on the teeth, especially in the area of primary chewing teeth.
The eruption of the first permanent molar in conditions of poor individual oral hygiene and the presence of a large number of untreated carious teeth nearby is often accompanied by the development of caries on the erupting young tooth (molar). During the process of eruption, the 6th tooth is partially covered with a mucous membrane, like a hood, under which plaque and food debris become clogged. The carious process in such conditions develops extremely rapidly, often unnoticed by the patient and his parents, and is quickly complicated by inflammation of the nerve of the tooth.
Treatment
The tooth is isolated from the oral cavity, from saliva using a rubber dam. It is convenient for both the doctor and the patient, as it allows the patient to partially close their mouth to rest during treatment.
Starting from the age of 5, children can easily tolerate long-term dental procedures in the oral cavity, provided they are adequately prepared for the first appointment and the doctor is able to find an approach to the child.
Treatment of caries of young erupting permanent molars at the age of 5 - 8 years is associated with a number of features that impose certain requirements. To carry out QUALITY treatment, complete isolation of the tooth from saliva is necessary. This can be achieved by using a rubber dam - a special latex screen (see photo), which allows you to quickly and efficiently restore a chewing tooth, without fear of saliva getting into the restoration area.
Like