The time when a child is cutting his adult teeth is one of the most serious and difficult periods of his development. To help the baby survive it without problems, parents need to know what symptoms indicate the eruption of molars, and how to help the child in this situation.
Molar milk teeth
What do parents need to know about baby teeth?
- Deciduous incisors, like permanent incisors, have a root.
- The rudiments of such dental units are formed in the prenatal period.
- When a temporary tooth is replaced by an adult one, the old root eventually resolves on its own.
- On the first teeth the enamel is softer.
- Baby teeth are smooth and have wide roots to provide room for the development of permanent tooth buds.
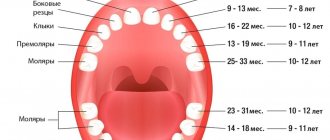
- Temporary teeth are canines and lateral incisors, central and first molars, premolars. The second molars in four-year-old children are already adults.
When the rudiments of an adult tooth appear, the root of its predecessor weakens and the tooth becomes loose. If it is not pulled out, an adult tooth may be visible underneath it. When milk interferes with it, it can grow with deviations from the norm.
The dentition is symmetrical in nature, and teeth erupt in pairs: on both parts of the dentition they appear almost simultaneously.
Timing of adult teeth eruption
The rudiments of the first teeth (on average, about 20 units) in infants are formed during the first two years of life. When the time comes to replace them with permanent teeth, the milk teeth become loose and fall out. There are no specific dates for the eruption of molars; many factors can affect the speed: environmental conditions, climate, water quality and diet. Genetic characteristics also play a certain role, some of which make themselves felt even during the formation of the fetus. The influence can be both positive and negative. If parents have healthy teeth from birth, then you don’t have to worry about the child’s teeth. If the first incisors, canines and premolars grow in 3 years, then the permanent ones take a long time to erupt. The first symptoms of dentition change can be seen at the age of 5, and it continues until the age of 21, when the third molars appear.
Advantages of treatment at Aurora
Removing the lower wisdom tooth is a complex procedure that requires high specialist competence. Due to the inconvenient location and improper growth of the last molar, neighboring teeth suffer. Highly qualified specialists of our center easily and quickly carry out complex operations of this level. In addition, Aurora dentistry has other important advantages over its competitors:
- the possibility of receiving installments from Pochtabank or Renaissance Credit;
- individual approach;
- work on weekends, including for residents of the region by appointment;
- The doctor is assisted by an assistant, which allows him to carry out manipulations 2 times faster;
- modern, 100% high quality, imported materials.
Our dentistry offers the following promotions for the removal of the lower wisdom tooth:
- If you found out about us through 2GIS, we provide 5% on services;
- 10% discount on your birthday and the next 3 days
- For pensioners there is a “Golden Watch” promotion - a 10% discount on tooth extraction from 9-00 to 11-00
In case of complex and long-term treatment, an individual discount policy and flexible payment schedule are provided
To make an appointment, just call. On the appointed day, the doctor will see the patient and tell him how the lower wisdom tooth will be removed without pain after the procedure and fear.
Signs of formation of permanent teeth
The most characteristic symptom of the formation of adult teeth in childhood is an increase in the size of the jaw. The gaps between the first teeth are small; if the jaw grows, this means that it creates conditions for new dental units. Adult teeth are larger than temporary teeth, so they require a lot of space. The distance between baby teeth increases. They lose stability and fall out. With any deviations, the teeth will break through with pain, bend, and ruin the bite. In order for a child’s teeth to grow correctly, parents need to control this process.
Permanent teeth can erupt at 6-7 years of age without any symptoms, but most often the child behaves restlessly, is capricious, gets irritated over trifles, and eats poorly. Often the formation of permanent teeth has the same signs as during the eruption of milk teeth. If other diseases occur during teething, they can distort the symptoms.
Increased secretion of saliva is a very common symptom; however, it is no longer as abundant as in infancy, but you can notice the difference. At the age of 6, children can already be taught to wipe their mouth with a napkin, otherwise irritation will appear on the face, since saliva contains many microbes that aggressively affect delicate skin.
During the period of growth of permanent teeth, the gums and mucous membranes become inflamed again. If you notice redness in the mouth, it is better to show the child to a dentist, who can accurately distinguish the beginning of teething from a banal viral infection.
Over time, swelling is observed on the gums - this is an adult tooth making its way to replace the temporary one. The germination process is painful; parents can alleviate the child’s condition with anesthetics.
Pain is replaced by itching. The child pulls any things to his mouth to soothe his gums.
A natural symptom will be deterioration in sleep quality. If he is bothered by toothache, the baby will not be able to fall asleep for a long time, often wakes up at night, cries, and tosses and turns.
Some children develop a fever, cough, and upset stool.
The listed signs may appear periodically and do not necessarily have to be present in all children.
Supernumerary molar: review of a rare case
Supernumerary teeth or hyperdontia is a dental anomaly that is defined as the presence of a tooth or any dental tissue in excess of the set of 20 primary teeth and 32 permanent teeth. Supernumerary teeth can occur singly, in groups, unilaterally, bilaterally, they can erupt or be impacted on one or both jaws, both in the primary and permanent dentition. The frequency of occurrence in primary dentition varies from 0.1% to 3.8% and from 0.3% to 0.6%. In permanent dentition, the anomaly is more common in men than in women in a ratio of 2:1. However, this gender disproportion is not observed in the primary dentition. There is also evidence that the Asian population is more susceptible to the anomaly. Single supernumerary teeth occur in 76-86% of cases, double teeth in 12-23% and multiple teeth in less than 1%. Multiple hyperodontia rarely occurs in people without any other concomitant diseases and syndromes. Typically, this anomaly is part of systemic disorders such as cleft lip and palate, cleidocranial syndrome, Gardner syndrome, Fabry-Anderson syndrome, chondroectodermal dysplasia, Euler-Danlos syndrome, and tricho-rhinophalangeal syndrome.
Supernumerary teeth can be found in almost any area of the dental arch. Localization on the upper jaw is much more common than on the lower jaw, especially in the anterior region (80%). Somewhat less frequently, supernumerary teeth can be located in the distomolar zone, lower and upper premolars, in the area of the upper canines and lower incisors.
The crowns of abnormal teeth have a normal appearance or an atypical shape, and the roots are also fully or partially formed.
The position in the dental arch varies: mesiodens, paramolar, distomolar and parapremolar. Mesiodens is the most typical localization between the central incisors on the upper jaw, paramolar position is an additional molar, usually rudimentary, small in size and located on the buccal or palatal side in relation to one of the molars on the upper jaw. Most often found in the interdental space of the second and third molars on the buccal side; distomolar position is the fourth permanent molar; parapremolar localization is mainly found in the interdental space on the buccal side between the first and second premolars in the upper jaw. Variations in the morphological shape include different conical type, number of tubercles, and odontome. Supernumerary teeth may be small, conical with a normal root; teeth with multiple cusps are usually short, with a barrel-shaped crown and an invaginated rudimentary root. Another variant of a supernumerary tooth - an additional one - resembles one of the existing ones and is located behind it. Most supernumerary teeth in primary dentition are of the accessory type.
Odontomas are any tumors that develop from tooth tissue. Many authors are inclined to believe that odontomas are a hamartoma or malformation rather than a neoplasm. Compound and compound odontomas are two different types described. Complex odontomas are characterized by diffuse dentin tissue that is completely disorganized, while compound odontomas are malformations that have superficial anatomical similarities to a normal tooth.
According to their shape, supernumerary teeth are classified into additional (eumorphic) and vestigial (dysmorphic). If supernumerary teeth have normal morphology, they are classified as “additional”; if the morphology is abnormal, the teeth are classified as vestigial. The position of the supernumerary teeth can be between the central incisors, overlapping, and the orientation is described as vertical, inverted, or transversal.
This article presents a clinical case of the presence of an additional molar in a somatically healthy patient. A review of the literature regarding the incidence, classification, etiology, complications, diagnosis and treatment strategies of this pathology is also presented.
Description of a clinical case
A 22-year-old man came to the Department of Conservative Dentistry and Endodontics with complaints of pain in the posterior segment of the upper jaw on the left. Hereditary anamnesis and disease history are unremarkable; no signs of systemic diseases or syndromes have been identified.
Intraoral examination revealed Class I occlusion and no pathological tooth alignment. In addition to the full set of permanent teeth, one supernumerary tooth was found, located on the palatal side between the upper first and second molars on the left (Figure 1).
Figure 1: Intraoral photograph showing the paramolar position of the supernumerary tooth between the upper first and second molars on the left.
The supernumerary tooth is defined as a paramolar. The paramolar crown had two cusps and very much resembled the structure of a permanent premolar. The tooth is rotated axially, with the buccal surface distally and the mesial surface buccal. A carious lesion was found on the mesial side of the paramolar (Figure 2). Examination of the soft tissues revealed periodontal inflammation between the first and second molars and paramolars. X-rays were taken: panoramic, sighting and occlusal. Reading the panoramic image was difficult due to the palatal position of the tooth. On sighting and occlusal photographs, it was discovered that the supernumerary tooth was affected by caries and had one root (Photos 3 and 4).
Figure 3: Spot X-ray showing a paramolar with a fully formed tooth (indicated by arrow).
Figure 4: Occlusal radiograph of the maxilla showing the supernumerary tooth (arrow).
The patient was informed of the existing situation. It is recommended to remove the paramolar due to its inconvenient location for hygiene, possible food retention, recurrence of caries and damage to periodontal tissue. The patient was sent to the Department of Maxillofacial Surgery for paramolar removal.
The extracted tooth is cleaned, disinfected and analyzed. The morphology of the tooth is normal. The length of the root corresponds to the size of the crown. The root apex is fully developed. X-ray examination revealed type I canal configuration (Vertucci). Actual tooth dimensions: mesiodistal and bucco-palatal crown width 6 and 10 mm, respectively, crown length 6.5 mm, root length 12 mm. Morphometric measurements showed a high similarity of the supernumerary tooth with the premolar (Photo 2).
Photo 2: Photographs of the extracted tooth: (a) occlusal view, (b) mesial, (c) distal, (d) buccal, (e) palatal.
Discussion
The appearance of paramolars is a fairly rare occurrence. The etiology of this anomaly is not fully understood. Several theories have been proposed: phylogenetic, dichotomous, dental lamina hyperactivity theory, and a combination of genetic and environmental factors.
Phylogenetic theory refers to the process of atavism (evolutionary return). Atavism is a return to an earlier morphology or type. In past centuries, the third molar was almost always present in the permanent dentition; it was comparable in size to the second molar. Moreover, the fourth molar was also quite common. However, as a result of the evolution of phylogeny, the size of the dental arches gradually decreased, which led to a reduction in both the number and size of human teeth. This was one of the stages of preferential development of the cerebral skull over the facial skull. Thus, the appearance of additional paramolars can be considered an example of atavism, the genetic memory of the fourth molar in previous generations. It is worth saying that this theory was rejected by many authors.
The dichotomous theory explains the appearance of supernumerary teeth by splitting the tooth germ. The rudiment splits into two equal or unequal parts, from which morphologically normal independent teeth subsequently develop.
The lamina hyperactivity theory is the most accepted theory. She explains the appearance of paramolars as a result of local, independent, due to special stimulation, increased activity of the dental plate. According to the theory, lingual expansion of the accessory tooth bud leads to the development of a morphologically unchanged tooth, and the vestigial forms arise from the proliferation of epithelial lamina remnants, which is induced by the pressure of permanent teeth. Others are inclined to believe that hyperodontia is associated with multifactorial causes, which are still based on hyperactivity of the dental plate. Remnants of the dental lamina may remain in the jaws in the form of epithelial pearls or islands. When exposed to inducing factors, supernumerary teeth or odontomas can develop from additional rudiments. The best supported hypothesis is that the development of supernumerary teeth is associated with a complex of genetic and environmental factors. This is confirmed by the presence of similar anomalies in close relatives. However, despite the literature data, similar pathology was not found in the relatives of the described patient.
A careful analysis of the literature revealed very little information about the appearance of paramolars. Paramolars are somewhat less common in the upper jaw, very rarely bilaterally and almost never in the primary dentition. They are usually vestigial and located buccally between the second and third molars, although in some cases they can be located between the first and second molars. Fusion of paramolars with normal teeth is also incredibly rare. The literature describes the only case of endodontic treatment of a fused second left molar in the lower jaw and a paramolar with a split crown.
Diagnosis also requires differentiation of other structures that may appear in the molar area, such as an additional cusp or a fused supernumerary tooth. Bolk in 1916 first described an additional cusp on the buccal surface of the upper and lower permanent molars, which he called the paramolar cusp. Dahlberg in 1945 proposed the term paramolar cusp to refer to any abnormal cusp, supernumerary inclusion, or elevation on the buccal surface of both maxillary and mandibular premolars and molars. He presented a paleontological nomenclature in which he classified these structures as “protostylid” if they are on the lower jaw and “parastylid” if on the upper jaw. It is widely accepted today that such formations originate from the cervical region of the tooth and are variable in appearance. Often these structures appear on the buccal surface of the mesiobuccal tubercle and quite rarely on the distobuccal tubercle. It is believed that the paramolar tubercles may originate from the remains of their own epithelium or be a genetic remnant from mammals and lower primates.
Supernumerary teeth may erupt normally, remain impacted, or appear axially rotated or with other abnormalities. Supernumerary teeth with a normal position in the bone usually erupt. However, only 13-34% of supernumerary teeth in the permanent dentition erupt normally, compared to 73% in the primary dentition. The rest may remain impacted and cause complications.
The development of complications can cause a delay in the eruption of associated permanent teeth, retention, ectopic eruption, disposition, rotation of adjacent teeth, crowding due to insufficient space for eruption, malocclusion due to a decrease in space in the dental arch during the eruption of paramolars, tremors in the molar area, traumatic bite and ulceration of the buccal mucosa with buccal placement of paramolars, difficulties in orthodontic treatment, pathological development of the root of associated permanent teeth, formation of follicular cysts from the follicular sac of a supernumerary tooth, trigeminal neuralgia due to compression, pulp necrosis and root resorption due to excessive pressure of the paramolar , caries due to plaque accumulation, gum inflammation and localized periodontitis. As can be seen from the described case, due to plaque retention, carious lesions of the paramolar and inflammation of the surrounding periodontium occurred.
Most supernumerary teeth are impacted and are usually discovered incidentally during radiographic examination. However, if a patient presents with complications that are often associated with the presence of a supernumerary tooth, the dentist should consider this anomaly in the differential diagnosis and insist on appropriate x-ray examination.
The most valuable radiographic examination is the OPG with additional targeted photographs and photographs of the upper and lower jaw in the occlusal plane. To clearly localize an unerupted tooth, use the vertical or horizontal parallax technique. Parallax is a change in the view of an object against a specific background based on the movement of the viewer. This technique can be carried out by taking images of the same area, but from different angles, with two different devices. When using this method, as a rule, the reference point is the root of the adjacent tooth. In addition, cone beam CT may be used. This technology provides a three-dimensional image of the structures of the specified zone and is incredibly informative for the described anomaly.
Clinical management of patients with paramolars depends on the position of the tooth and its effect on surrounding tissues and important anatomical structures. Treatment offers two options: removal or observation. Observation does not include any manipulations other than clinical and radiological monitoring of the patient. This method is preferable if the presence of a paramolar is asymptomatic and does not cause any inconvenience. If any complications arise, tooth extraction is advisable. In the described case, we resorted to tooth extraction in order to maintain the proper level of hygiene, prevent the carious process and preserve the surrounding periodontium.
Conclusion
The dentist needs to know about the different types of supernumerary teeth for proper diagnosis and timely detection of this anomaly. Each such case requires careful diagnosis and subsequent appropriate treatment that causes minimal complications.
Authors: Gurudutt Nayak, Shashit Shetty, Inderpreet Singh, Deepti Pitalia Department of Conservative Dentistry and Endodontics, Kanti Devi Dental College and Hospital, Mathura, Uttar Pradesh, India
The order of appearance of adult teeth
Almost all milk teeth that erupted in the first two and a half years, 10 on each half, are replaced by permanent ones. Compared to their predecessors, adult teeth form in a different order.
Table. The order of formation of permanent teeth
| Tooth name | Development timeframe | Peculiarities |
| Lower and then upper molars | This usually occurs in the seventh year of life | They make their way behind the second primary molars |
| Molar lateral | In time, this can take three years - from 6 to 9 years | They sprout when the central incisors are already formed |
| Permanent fangs | Normally, this occurs between the ages of 9 and 11 years. | By cutting the gum from the inside, they seem to displace milk precursors |
| First and second adult premolars | Appears at 10-13 years of age | They grow in place of central incisors, which become loose and fall out. |
| Third molars, better known as wisdom teeth | They may erupt at 18 years old, or at 25, or not at all. | Such cases are not considered a deviation from the norm. |
If a baby's individual teeth grow in a different order, this is not dangerous. Individual characteristics, deficiency of vitamins and minerals slow down the speed and sequence of formation of permanent teeth. It is important for parents to know that an adult tooth should not become loose; if there are similar symptoms, this should be a reason to visit the dentist.
Removal steps
The procedure can be divided into three stages:
- preparatory;
- The operation itself;
- After surgery.
Preparatory stage.
At this stage, the doctor visually examines the patient's oral cavity. Then a computed tomography is done to look at the length and shape of the roots, the depth of the tooth, etc.
Surgery
Complex wisdom tooth removal is divided into several stages. Let's consider a generalized operation scheme:
- A painkiller is given. To do this, a needle is inserted into the lower jaw to the nerve bundle so that the patient does not feel pain. Lips, chin, tongue are numbed. If sensitivity does not disappear, an additional injection is given. After anesthesia, the course of a complex extraction procedure depends on the location of the tooth.
- An incision is made with a scalpel.
- The tooth is sawed down to make it easier to remove.
- Take out the crown and roots.
- The wound is treated and sutured.
This completes the surgical stage.
Postoperative stage
This stage is very important, its duration is 7 – 10 days. During this period, the surgical wound heals, and a clot first forms in the hole and then resolves. Patients must follow our doctor's instructions exactly to avoid post-operative complications.
How long does the procedure take?
With a simple type of extraction, the procedure is carried out in 10 - 20 minutes. The process of complex removal lasts from 30 minutes or longer, depending on the specifics of the operation. For example, removing a horizontal tooth can take up to 2 hours or more. At the same time, sometimes additional preparatory procedures are necessary, which also take time.
After tooth extraction in the lower jaw antibiotics to prevent the entry and spread of infection. Such complex manipulations are contraindicated for pregnant and nursing mothers. Painkillers are prescribed to reduce pain after the procedure.
For complex removal, the patient is asked to come back again in five days or earlier if a fever appears. If the tooth has come out halfway (semi-retinated tooth), removal is carried out in the same way, but it is easier to pull it out, since part of the molar is on the surface.
Associated symptoms
These symptoms do not appear very often, but they cannot be ignored. If the baby has a fever, an incomprehensible cough, or diarrhea, this can be either a sign of infection or a reaction of a weakened body to pathogenic microflora.
When teeth are forming, the temperature usually lasts for 3-4 days at 38.5°C. This symptom is irregular, so fever in children should be periodic. If it persists for a long time, you need to show the child to the pediatrician. Some doctors believe that cold symptoms have nothing to do with teething and prescribe appropriate treatment for cough and fever.
Adults also don’t understand what cough and runny nose have to do with new teeth. The gums are directly connected to the blood supply to the nose and respiratory tract. As teeth form, blood flow increases in the mouth. The nasal mucosa is close, so its glands also begin to produce more mucus, which children try to get rid of. Remaining mucus settles into the throat, irritating the airways and causing a cough.
Another symptom is loose stools with a frequency of no more than 3 times a day. While scratching his gums, the baby constantly puts dirty fingers and the first objects he comes across into his mouth. In addition to infection, diarrhea is facilitated by increased salivation, which constantly flushes the intestines. If the stool is short-lived and does not contain blood, there is no need to worry about the child’s health. It is necessary to monitor his condition, since with a weakened immune system there is always a risk of developing an infection, which aggravates all the symptoms.
Pain after removal of lower wisdom tooth
Pain after wisdom tooth removal is the body’s protective reaction to external intervention. This is absolutely normal, since an open, fresh wound remains in place of the figure eight. Gradually, a blood clot forms in the socket, acting as a “protective cushion” that prevents pathogenic microflora from entering and multiplying. That is, the pain syndrome appears due to damage that occurred during the operation:
- injuries to bone tissue or gums;
- damage to nerve fibers or blood vessels;
- inflammation of the gums.
In addition to pain after removing the figure eight, there are a number of other symptoms that should be taken into account:
- in the first few hours it hurts to open your mouth;
- soft tissue swelling;
- pain radiating to the temple;
- increased temperature (37-37.5°C);
- feeling of ear fullness;
- bad breath;
- swelling of the cheeks or lips.
The listed symptoms are considered normal if they begin to subside after 1-2 days.
If the pain intensifies and does not go away within a week, it is possible that a pathological process is developing. Severe pain at the site of the removed wisdom tooth may be associated with one of the common complications of the operation:
- alveolitis is an inflammatory disease affecting the tooth socket. May occur as a result of a blood clot being washed out or absent, a violation of the rules of oral care, infection entering the socket during or after surgery, etc.;
- damage to small blood vessels;
- allergic reaction to drugs
If symptoms such as swelling, bruising, increased body temperature, general deterioration in health, etc. appear, in this case you should definitely consult a doctor.
After removal of the lower figure eight, jaw pain . This may be due to several factors:
- during the removal process, blood vessels, ligaments, nerve endings, and tissues that supported the adjacent tooth were ruptured;
- The doctor applied pressure to the jaw to gain access to a distant tooth.
These are normal symptoms as long as you do not have difficulty opening your mouth or there is severe swelling of the face or soft tissues in the mouth.
It is worth considering that if a molar is pulled out the first time, the damaged area will hurt intensely for at least 3-5 days. By the end of this period, the damaged area will be almost completely healed.
If the removal was difficult, the healing time increases to 2-3 weeks. And soft and hard tissue will hurt for at least a month. The intensity of sensations will decrease every day.
When to see a doctor
If you experience the following symptoms, you should consult a doctor:
- the pain intensifies every day, painkillers do not help, or help little;
- the pain does not go away or decrease a week after tooth extraction;
- the pain is not aching, but pulsating, it radiates to the neck, eye, temple, and interferes with sleep. Such sensations are a sign of an inflammatory process; you should consult a doctor immediately;
- swelling does not disappear on the 2nd–3rd day after surgery, but, on the contrary, increases;
- there is a high temperature that does not fall even after 2-3 days;
- an allergic reaction to medications prescribed by a doctor occurs;
- alveolitis (inflammatory disease) occurs in the socket;
- your health worsens on the 2nd–3rd day after the procedure.
Important! If initially the pain was not intense immediately after surgery, but after 12-16 hours it intensified, this is a normal condition. The local anesthesia simply stopped working. If, after the removal of a wisdom tooth, the pain returns and becomes stronger after 5-7 days, then this is a sign of the development of a complication.
Children's adult dental problems
Permanent teeth that are barely emerging may already have developmental deviations, and parents should be prepared for this.
- Lack of permanent teeth. If all the normal deadlines have passed, but they still haven’t appeared, the dentist examines an x-ray, on which you can see the jaw with new teeth. The reasons may be heredity (this is noticeable in the picture) or adentia - the absence of the formation of rudiments in the womb. Sometimes newborn teeth die due to inflammation. In such cases, children are given prosthetics.
- Molar tooth pain. The new tooth does not yet have a normal layer of minerals. Due to weak mineralization, it is easy for a child to catch caries, and with deep destruction, pulpitis with periodontitis. In such cases, toothache will be accompanied by fever and weakness. Postponing a visit to the dentist risks losing an adult tooth. In case of weak enamel and milk caries, fissure sealing is sometimes recommended - closing the recesses on permanent teeth with a composite material.
- Uneven growth of permanent teeth. If the growth of an adult tooth outpaces the loss of a temporary one, the bite is disturbed. Orthodontic therapy is required, in which the temporary tooth is removed. There is no need to loosen it or remove it at home.
- Loss of adult teeth. It happens both with inflammation of the gums, pulpitis, caries, and with general diseases (diabetes mellitus, systemic pathologies of connective tissues). The loss of anterior teeth is a serious problem: in order for the maxillofacial apparatus to form normally, the baby needs temporary prosthetics. When the jaw is fully formed, temporary dentures are replaced with permanent ones.
- Injury to molars. Most modern children are hyperactive, so there is always a risk of mechanical damage to the teeth, especially since they fully mature only a few years after their appearance. For minor fractures and cracks, the volume is increased with composite material.
Possible complications after removal
Complications after surgery arise due to violations of doctors’ recommendations. Patients begin to rinse their mouth, go to the bathhouse, play sports, or do not take medications that were prescribed. It is absolutely IMPOSSIBLE to do this for 5 days, because the place where the tooth was located is easily inflamed. Pain after removal is normal. Because the anesthesia wears off and the gums heal. Taking painkillers reduces pain.
Without taking antibiotics, inflammation and suppuration may begin. This situation arises due to the fact that food often accumulates at the end of the gums, which is difficult to remove with a brush, and along with it remain microbes that cause suppuration.
If bleeding occurs after removal, you should press the wound with a cotton pad for 15 minutes. If the bleeding does not stop, you should consult a doctor.
For reference! For high-quality and rapid healing, it is necessary that the wound heals well, so you should not eat hard food for at least 5 days and clean the hole.
Caring for teething teeth
When changing teeth, caring for them must be especially thorough, because a lost tooth tears the tissue, and when infected, it quickly becomes inflamed. To prevent such problems it is necessary:
- teach children to regularly brush their teeth, use a scraper and floss, and rinse their mouths;
- to support the enamel, buy your baby a paste with added calcium and fluoride;
- Proper nutrition with limiting sweets and carbohydrates in favor of vegetables, fruits, and dairy products will help strengthen new teeth and protect them from caries;
- consult a doctor on the choice of vitamins (especially vitamin D) and gels to improve the mineralization of new teeth;
- In case of inflammation, before meeting the dentist, you should actively rinse the child’s mouth with antiseptics and herbal decoctions.
You can buy mouthwashes for children or prepare herbal teas for this purpose.
Bad habits interfere with the normal growth of adult teeth: sucking fingers or tongue, pacifiers and any objects. Despite the lost teeth, do not limit your baby to solid food. A piece of apple or carrot massages and strengthens the gums, freeing teeth from plaque.
Make an appointment for lower wisdom tooth removal
Byshlyaga Dmitry Yurievich
Byshlyaga Dmitry Yurievich Orthopedic dentist
Extensive practical experience. Regularly undergoes internships and advanced training courses.
Working hours: from 9.00 to 20.00, daily, seven days a week, by appointment
Make an appointment
More details
Asatryan Alexander Aramovich
Asatryan Alexander Aramovich Dentist therapist - orthopedist - surgeon
Extensive practical experience. Regularly undergoes internships and advanced training courses.
Working hours: from 9.00 to 20.00, daily, seven days a week, by appointment
Make an appointment
More details
×