Bite is a feature of the arrangement of the jaw rows and teeth relative to each other. The functionality of the oral cavity, the attractiveness of the smile and the external symmetry of the face depend on how correct the bite is. Permanent occlusion is the final stage of the formation of the general dental system, which is completed only at 24-25 years of life. Up to this point, correcting the abnormalities is not so difficult, but after 25 years, treatment can be quite complex and lengthy.
general information
In medical terminology, occlusion refers to the relationship of teeth. The dentist analyzes the state of the chewing muscles and the temporomandibular joint at the moment when the jaws are clenched.
Bite is the position of the teeth in relation to each other when the jaws are fully closed.
There are physiological and pathological or, respectively, correct and incorrect bites.
A physiological bite in humans ensures high-quality functioning of the dental system (chewing food), clear diction, free breathing and an attractive smile.
With a correct bite, the face is harmonious, the lower and upper jaws are formed proportionally, the load on all teeth is carried out evenly, the vertical axis of symmetry of the face crosses the junction between the front incisors. This allows a person to chew food thoroughly without injuring soft tissue or periodontium and without overloading the temporomandibular joint.
Other pathologies
The formation of a pathological permanent bite can occur due to a large number of reasons.
Dentists identify the main factors influencing the condition of teeth during their formation:
- disturbances during the formation of the rudiments of milk or permanent teeth due to a lack of calcium in the body of a pregnant woman or child;
- heredity;
- pathologies of intrauterine development or chronic diseases;
- presence of bad habits , for example, prolonged sucking of a pacifier or fingers, biting nails, resting the chin on the palms of the hands;
- mechanical injury to the jaw.
Experts in the field of orthodontics note that the formation of an abnormal permanent bite causes not only disturbances in the aesthetics of the appearance of the oral cavity, but also numerous functional disorders .
The most common of them are the following diseases:
- disturbances in the functioning of the digestive system as a result of inadequate chewing of food;
- inflammation of the gum tissue due to injury;
- pathological abrasion of the enamel due to the incorrect relationship of the opposite elements of the jaw rows;
- loosening of teeth , characteristic in cases of uneven distribution of chewing load;
- breathing and diction problems.
In the absence of timely treatment, acquired diseases will progress, leading to new severe consequences for the body.
What is Costen's syndrome and the symptoms accompanying the pathology.
From this publication you will learn how the pacifier affects your child’s bite.
Here https://orto-info.ru/zubocheliustnye-anomalii/chelyustey/krivaya-ne-prigovor.html all the most important things about methods for correcting a crooked jaw.
Physiological types of occlusion
Orthognathic
It is recognized as the standard type of occlusion, as it creates the most suitable conditions for processing food during chewing.
- The upper row of teeth overlaps the lower one by a third.
- When the jaws join, the teeth come into close contact with each other.
- There are no gaps or cracks between the incisors.
Biprognathic
Signs of bite:
- The upper and lower incisors are located with a slight vestibular inclination - towards the vestibule of the mouth.
- Contact between the incisors is maintained when closing.
- The upper canines overlap the lower canines by several millimeters.
Direct bite or orthognathic
This type of bite is diagnosed when, when closing the jaws, the upper teeth touch the cutting edge of the lower row of teeth. There are no voids, cracks or crowding of teeth. Correct occlusion of the chewing teeth is observed.
Functions and position of teeth
The total number of teeth located in a person's mouth can range from 28 to 32, depending on whether the third molars have been cut.
Depending on the structure, all elements of the jaw line are divided into several groups, each of which performs certain functions in the process of eating food:
- Incisors – eight central teeth, which are located four in the upper and lower jaw rows. These are elements with one root and a sharp cutting part, the purpose of which is to bite off food.
- The canines are located in the jaw row behind the incisors. There are 2 fangs on each jaw. These elements have a special pointed edge that helps them participate in the digestion process by tearing food particles away from a larger piece.
- Premolars are also called small molars. These elements are located 4 in each jaw row and are necessary for grinding and grinding food. This is achieved by the prismatic shape and the presence of two tubercles on the chewing surface.
- Molars are the largest elements of the jaw row.
Their number in the oral cavity reaches 12 units - 6 in each jaw row. The molars are rectangular in shape and have three strong roots. Their chewing surface is equipped with four tubercles, which allows them to thoroughly crush and grind food before swallowing it.
Wisdom teeth are the third molars in the jaw row, which erupt later than the other elements.
They play a small role in the digestive process; their main purpose is to protect the remaining molars from loosening as a result of high chewing load.
At what age does a mixed dentition occur and the features of its formation.
Read here about senile progeny and methods of its treatment.
At this address https://orto-info.ru/zubocheliustnye-anomalii/okklyuzii/profilaktiki.html we will talk about devices used to prevent malocclusions.
When the construction of teeth is considered incorrect
The main signs of malocclusion:
- Complete or partial absence of tooth contact during occlusion.
- Impaired chewing of food.
- Sound pronunciation defects.
- Changes in the shape of the face due to jaw deformations.
Pathological types of bites
Pathological occlusion is diagnosed if there are structural deviations from normal anatomy in the structure of the dentofacial apparatus, and disturbances in the functioning of the masticatory muscles and the temporomandibular joint are also detected.
Mesial
A distinctive feature of this type of abnormal bite is the advancement of the lower dentition in relation to the upper one.
Patients with mesial occlusion have a characteristic appearance - a massive protruding chin, a receding upper lip, and a concave facial profile. There are chewing disorders and speech defects.
Deep
With a deep bite, the upper incisors cover more than 50% of the lower incisors. In some cases, the upper incisors, when closing the teeth, reach the gums of the lower jaw and injure them.
Although orthognathic, biprognathic, and straight bites are normal, these types of bites can cause the following problems: damage to the enamel, chipped crowns, and injuries to the soft tissues of the oral cavity.
Open
The main sign of pathology is the presence of a vertical gap between the dentition in the area of the frontal or chewing teeth.
An open bite is often formed against the background of narrowing of the alveolar arches, which is why the teeth have an irregular shape and are crowded.
Symptoms: lengthening of the lower third of the face, slightly open mouth, hypertonicity of the facial muscles, impaired diction, difficulty breathing, inadequate chewing of food.
Cross
Due to the displacement of the lower jaw to one side, the dentitions close like scissors crosswise, and underdevelopment of the jaw on one side is noted. Facial asymmetry is pronounced.
Distal
This is a variant of a pathological bite, in which the lower dentition moves back in relation to the upper one. In this case, the frontal (front) group of teeth does not connect, and the chewing teeth contact incorrectly, which creates the preconditions for blocking the normal development and growth of the lower jaw.
Facial signs of distal bite:
- protrusion of the upper jaw;
- shortening of the upper lip and lengthening of the lower lip;
- sloping chin.
Dystopia
A type of abnormal bite when the teeth on the upper or lower jaw are located outside the dentition and not in their place. In addition, with dystopia, the teeth are often turned around an axis.
Occlusion and bite
Why does a patient come to the orthodontist? That's right: straighten your teeth and correct your bite... We have already talked about this (see here)
But what a bite is and what it is eaten with (especially what is a regular and incorrect bite of teeth) the patient usually does not have the slightest idea. For another patient, for example, what the bite and what the taste is unambiguous. That’s how they formulate it: “We’re... about this at Vkus ... like straightening it out.” Many of my colleagues are not far behind them: out of ten dentists I interviewed from different specialties (orthodontists, orthopedists, surgeons, therapists), only four were able to more or less clearly formulate what a bite . And on the question (desire) to justify and clarify the meaning of the concepts of occlusion and occlusion, every single one floated. How...
But such concepts as bite and occlusion are key not only in orthodontics, but in dentistry in general. Therefore, together with you and my colleagues, I would like to speculate on this topic and finally decide on the concepts of what kind of bite this is (which sometimes you really want to correct). And what exactly is correct and incorrect bite?
Dental occlusion is any (any) closure of the teeth of the upper and lower jaws. The key word here (both in the concept of occlusion and in the concept of occlusion) is closure . If there is no closure, this is no longer an occlusion. This is disocclusion (its absence).
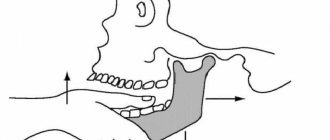
Depending on the position of the lower jaw (and as you and I know, it is mobile), several types of occlusion are distinguished: central , anterior , posterior and lateral .
a ) Central occlusion; b ) Posterior (distal) occlusion; c ) Anterior (sagittal) occlusion
Central occlusion (CO) is something of an ideal or template. In life and practice, the practically unattainable, or rather, often simply not achievable (for various reasons). It is generally accepted that CO is characterized by three (although later we will understand that it is far from three) main factors: dental , articular and muscular .
Well, with the dental factor everything is clear: the teeth must close together. And preferably not anyhow, but in a clear order. But I’ll tell you about this a little later, when we talk about bite . What about the other two factors? Let me explain.
Joint factor CO (central occlusion). You and I know that the position of the lower jaw can be determined by the position of the articular heads of the temporomandibular joint (TMJ). Well, with central occlusion, the articular heads stand most evenly and correctly, reflecting the ideal position of the lower jaw relative to the upper jaw.
Let me remind you: the upper jaw, unlike the lower jaw, is practically motionless. It is tightly nailed (and in some cases screwed) to the skull. JOKE! We will have a separate conversation about fixing the upper jaw to the skull... Everything there is also very interesting and not so simple.
The ideally even placement of the articular heads of the lower jaw in the articular fossa of the temporal bone should be ensured by the most uniform and balanced work of certain muscles of the maxillofacial area. After all, it is the muscles that ensure the position of the lower jaw in space (in fact, like any other bone). Here you have the muscle factor .
I repeat once again - CO (central occlusion) is like a certain ideal that everyone seems to strive for, but getting it is something with something (does everyone, and does it always succeed?). Because just imagine how many confusing factors (and you can’t even imagine how many) are preventing you from achieving this ideal. Well, we'll talk about this later.
What about other types of occlusion? Everything is simpler here. He moved the jaw forward - anterior occlusion . Pushed it back (it's not that easy, right?) - you get posterior occlusion . The jaw is turned to the right and left (the only thing is that the teeth must be in contact) - this is lateral occlusion .
the
occlusion . What is a bite ?
“Bite is the closure of the teeth in the usual, static position of the lower jaw” (L.S. Persin)
Based on the very formulation of the concept of occlusion, its main feature is the closure of the teeth (occlusion) or the absence of their closure (disocclusion). And the connection to the position of the lower jaw (and it is this, as we have already said, that determines the type of occlusion), allows us to say that a bite is the closure of the teeth in the usual occlusion. Those. occlusion is a very special case of occlusion. And it turns out that it is purely individual.
Someone’s teeth may be perfectly straight and seem to fit together correctly (i.e., have the most multiple and dense contacts). Those. The bite is basically there. But the lower jaw (and the articular heads clearly show this) is shifted, for example, into lateral occlusion. And for a person this closure will be habitual (teeth close together better than ever). And it is this habitual closure that will be his bite. Individual. Which, by the way, due to the incorrect position of the lower jaw, it would be nice to correct it... Despite the possible complete “Hollywood” with teeth.
So it turns out that when the bite (the habitual closing of the teeth) coincides with the central position of the jaws (central occlusion), the bite is physiological. And with anomalies of occlusion, the usual position of the lower jaw does not coincide with the CO. And then the type of bite is determined by the position of the lower jaw, which is familiar to a person.
This is how a physiological bite is distinguished from an abnormal one .
The concepts of physiological occlusion and physiological occlusion are identical. In the case when there is a problem with the closure of the teeth, but their closure still takes place, we can talk about an malocclusion (occlusion). For example: distal occlusion, mesial occlusion, etc. Those. There is closure of the dentition, it’s just disturbed. When there is no closure of teeth at all, then they don’t talk about bite. In this case it simply does not exist. Just as there is no occlusion. Therefore, for example, it is wrong to diagnose “open bite.” If there is no bite, it means disocclusion.
Physiological occlusion has a number of signs:
Fig.1:
Fig. 1: The upper lateral teeth overlap the lower ones to the depth of the longitudinal fissure (b) , and in the anterior section the upper incisors overlap the lower ones by no more than 1/3 of the height of their crowns (a)
Fig.2:
Fig. 2 : Each tooth intersects with two antagonist teeth (a) . In addition to the lower central incisors and the upper last teeth (they have one antagonist each) (b)
Fig.3:
Fig. 3: Each upper tooth intersects with the lower and posterior lower teeth of the same name (a) . And each lower one has the same upper and front upper teeth (b)
Fig.4:
Fig. 4: The midline should pass between the central incisors
Fig.5:
Fig.5:
• On the upper jaw, the dental arch is larger in diameter than the alveolar arch, and the alveolar arch is larger than the basal (jaw)
• On the lower jaw it’s the opposite: the basal arch is the widest, then the alveolar, and the narrowest is the dental
Fig.6:
Fig. 6: The teeth of one jaw are in contact with each other pointwise, on approximal (lateral for incisors and canines, and anterior-posterior for premolars and molars) surfaces
Fig.7:
Fig. 7: The height of the tooth crowns decreases from the central incisors to the molars, with the exception of the canines. The upper teeth are inclined outward (vestibular), and the lower teeth are vertical
Fig.8:
Fig. 8: The first molars, with their mesial-buccal cusp, enter the intercuspal fissure of the lower molar of the same name
Now we understand what, what closure (as a result of treatment) we should strive for? Although this is just the “external” part of the occlusion (bite). And in the modern interpretation, occlusion (occlusion) is not only the teeth and their closure. Everything there is much deeper and more interesting. But we'll talk about this a little later...
There are also closure of baby teeth ( deciduous occlusion ), closure of permanent teeth ( permanent dentition ) and mixed occlusion (closing of teeth during the period of change of baby teeth to permanent ones).
Well, we seem to have determined the guidelines for the “correct” bite. Have you read it? Remember. Great. Now... forget it. Why? Yes, because the landmarks here are the teeth. Only teeth. And teeth are a very superficial and very unreliable guide. Dependent on many other guiding factors. This means that it is at least unreasonable to determine the “correctness” or “incorrectness” of a bite only by the closure of the teeth. This is unreliable. Not exactly. It is fraught with errors and problems, which we see almost every day.
Unfortunately, in the vast majority of cases, all orthodontic treatment is based on these “unsteady”, unreliable “purely dental” guidelines. Yes, not only orthodontic, but dental in general. Prosthetics, implantation, and dental restoration also rely on the teeth themselves. Only on the teeth. In fact, the goals and objectives of dental (and orthodontic, including) treatment very often boil down only to “attracting” teeth to each other. And a prosthetic device is inserted into the lung and implanted. Getting a certain external effect, the appearance of a “correct” bite, the illusion of successful treatment. And then comes the reckoning...
Expensive crowns and bridges break for no apparent reason. The implants fall out or become inflamed. And crooked teeth are corrected in the wrong direction. And with the temporomandibular joint, the problem suddenly pops up out of the blue. And this, by the way, is really a problem, since you won’t find specialists in TMJ during the day. No, of course there is a lot of advertising and show-off. Has anyone seen the results?
Or even more abruptly: problems of a different order begin, seemingly far from the teeth: the lower back aches, the head hurts, the pressure jumps, the body somehow reacts negatively to the weather... And endless trips to neurologists, neurologists, psychotherapists, osteopaths, and other “atams” begin ", "-istam", and "-ologam". Endless, because these specialists usually also see nothing except “their” sore.
And it is not known that these troubles, including the incorrect formulation of the concepts of occlusion and occlusion, are to blame. But naturally, it is the patient who pays for this “broken aim.” Not with money (or rather, not only with money). The main thing, and the saddest thing, is your health. And often without even realizing that the cause of many (oh, many) sores is an incorrect, and sometimes incorrectly corrected, bite. And why all? Yes, because the attitudes and dogmas on which modern dentistry exists have not changed, by and large, for a hundred and fifty years. And what then is the “modernity” of today’s dentistry? Only in the fruits of technological progress? It turns out to be some kind of “race in width”. You look at the topics of training seminars and it makes you feel sick. What are they talking about: “which braces are cooler...”, “which fillings are better...”, “which ceramics are more beautiful...”. And what? Just spend your life on this? Is it hard to dig deep?
And the very formulation of the concepts of occlusion and occlusion , as the main guidelines in dental treatment, is high time to change. Otherwise we will remain Neanderthals. Savages armed with modern equipment. Incapable, with all their “weapons”, of competent treatment, of real help.
Are you upset? Understand. But let's figure it out...
So let’s start right away with the formulation of the bite. Remember what it sounds like? “Closing of teeth in habitual occlusion.”
Closing teeth . Where do teeth come from? That's right - from the jaws . And if, say, the jaw is in the wrong position, or is deformed, will this affect the closure of the teeth or not? Of course yes.
And where does the jaw (let’s take the upper one) grow from? Let's remember the anatomy... That's right - it is attached to the skull . To the very base of the skull. And if the cranial bones are deformed, or are in the wrong position (displaced as a result of injury), can this be reflected in the position of the upper jaw? Maybe. And therefore, such a displacement will also affect the closure of the teeth (bite). How interesting, right?
What about the lower jaw? In general, it also seems to be “attached” to the skull. Through the temporomandibular joint (TMJ). And an integral part of the joint is the temporal bone (skull bone!!!). More precisely, its articular fossa. And if the temporal bone is, for example, in some kind of external rotation (and this is quite common), do you think this will have any negative consequences for the lower jaw and lower teeth (and further for occlusion)? And there is no need to think - the answer is obvious.
In addition, the lower jaw (its position) is directly dependent on the position of the upper jaw. The dependence is approximately the same as a door depends on the door jamb: the jamb is smooth and the door does not creak. And it opens normally. And the jamb is crooked - and the door is also incorrectly positioned, which leads to problems with its opening and closing...
And it’s the same with the jaws: if the upper jaw is deformed or incorrectly positioned in space (by itself or due to “distortions” of the cranial bones), then the lower jaw is forced to adapt to the “wrong” upper jaw. And how is the adjustment (forced position) ultimately ensured and carried out? Yes, the teeth are compensatory and incorrectly positioned. Here you go: get the wrong bite.
Go ahead. And what does the skull “contact” with anatomically? That's right - with the spine. This means that any problem with posture (scoliosis of some kind) will immediately cause a compensatory restructuring of the bones of the skull. And with them the upper jaw. And then, as in the fairy tale about the turnip: the spine bent - the skull “moved” - followed by the upper jaw, followed by the lower jaw. Plus, the dentition is compensatory deformed... (read the mechanism above). The “exit” is, again, the problem of teeth closing.
One thing needs to be understood: teeth are part of the skeleton . And the skeleton is a closed kinematic system. Everything in it is built on compensation (to maintain balance). And we still treat flat feet separately. Separately, we “correct” the posture. And we are separately trying to solve the problem of teeth closing (occlusion). And we are also surprised when something “not very good” comes out.
Or on the other hand... Imagine if you thoughtlessly “correct your bite” and “straighten” your teeth. As many people think, put on braces and wear them for a year and a half. That's all. Happiness will arrive. And the fact that by “correcting” the bite we have “corked” all the skeletal distortions (unaccounted for), as if with a cork – how is that? What then is the treatment? And how (what problem) will the patient pay for straight teeth?
Even a hedgehog has long understood that the closure of teeth depends on many “non-dental” factors. And that the bite is not just teeth. That is why there is a need (long overdue) to expand our understanding of what occlusion and dental occlusion . And give a more precise formulation of these concepts.
READ CONTINUED…
Sign up for diagnostics
Social Like
Comments for the site
Cackl e
Causes of malocclusion
The formation of a bite is a complex and lengthy process that begins at the stage of intrauterine development and ends only when a person reaches puberty.
- Genetic factor. One of the leading reasons for the formation of malocclusion is heredity, which determines the size and shape of the teeth, the width and length of the dentition, the height of the hard palate, as well as the nature of the location of the teeth (sparse or crowded).
- Quality of nutrition and maternal diseases during pregnancy.
- Birth injury. Jaw injuries received during childbirth lead to displacement of the temporomandibular joint, and subsequently to the formation of a pathological bite.
- Incorrect selection of nipples during artificial feeding, when the child does not make enough effort to obtain milk, as when sucking at the breast, which causes underdevelopment of the lower jaw.
- Untimely introduction of solid foods into the diet during teething. In the absence of chewing, the muscles of the dentofacial apparatus, on which the development of the jaws largely depends, are not strengthened.
- Behavioral factors: sucking pacifier, upper lip, fingers; sleep with the head thrown back.
- Irregularities in the timing and sequence of teething.
- ENT pathologies due to which the child is forced to breathe through the mouth for a long time: chronic rhinitis, sinusitis, deviated nasal septum, adenoids.
- Diseases affecting bone growth and development.
All these factors can cause improper closure of the dentition and form a pathological bite.
Stages of bite development
By the age of 12, a child usually begins the process of active formation of a permanent bite, which includes the following stages:
- at the age of 13-15 years, a period of development begins, active growth of the alveolar processes, eruption of second molars, this stage ends only by the age of 18;
- The period of preformation lasts from 18 years to 24-25 years, at this time the dental arches develop, and the jaws acquire their final size. At the same time, third molars erupt, although experts note that not everyone has wisdom teeth;
- The final formation of the bite ends when a person has all 32 teeth, at which time development stops, but mesial displacement can continue throughout life.
In the process of forming a permanent bite, not only the position of the teeth changes, but the proportions of the face.
Prevention
A set of measures aimed at preventing the development of dental anomalies in children includes:
- balanced nutrition of a woman during pregnancy in order to provide the fetus with the substances necessary for its skeletal system;
- inclusion in the diet of a growing child of vitamins and microelements necessary for the proper formation and mineralization of teeth;
- preventing the development of bad habits in children that cause occlusion disorders (prolonged use of a pacifier, finger sucking);
- timely treatment of dental, infectious, endocrine and other somatic diseases;
- regular monitoring of the condition of the dental system.
Price
The cost of correcting a permanent dentition depends on the complexity of the malocclusion, the age of the patient, the number of teeth that need to be aligned, and the type of design used:
| Type of orthodontic device | Cost, rub. |
| Bracket system | From 5000 for metal to 90000-100000 for ceramic or sapphire |
| Aligners | 100000—180000 |
| Plate | From 4000 |
| Trainers | 6000—10000 |
It is worth understanding that prices may vary among different dental clinics. It depends on their location, prestige and fame.
Correction Methods
Correcting the position of teeth takes much less time and effort if done in childhood. This is explained by the fact that during primary occlusion the jaw lines are not fully formed, which allows the incisors and canines to change their position more easily.
Orthodontists note that in patients under six years of age, the bite can be corrected without radical measures, based only on performing myogymnastic exercises and wearing special plates and devices.
After the process of forming a permanent bite is completed, it is much more difficult to achieve its correction, but experts do not exclude this possibility.
To do this, they offer the use of various orthodontic structures.
Bracket systems
Braces are non-removable structures consisting of special clasps attached to the tooth surface and a power arc connecting them, as a result of which pressure is created on certain elements of the row.
Depending on the desired result, braces can be attached to all teeth or to certain elements of the jaw row, causing them to shift to the required position.
At the request of the patient, bracket systems made of various materials, such as metal, ceramics, plastic, and sapphire, can be used. The duration of bite correction with braces ranges from six months to two years.
Aligners
In this case, the change in bite occurs due to the wearing of special aligners made of transparent biopolymer material.
The number of these devices often ranges from 10 to 40 pieces, which must be changed regularly during the treatment process.
Dentists note that this method is effective for correcting minor malocclusion pathologies, such as crowding and displacement of individual teeth, the need to equalize the length of some elements of a row, and eliminating teeth and diastemas. The duration of orthodontic treatment with aligners can be up to two years.
Plates
Orthodontic devices consisting of a palatal plane and a metal arch that exerts pressure on the protruding elements of the jaw row.
Dentists recommend this method of bite correction for a small number of crooked teeth and the absence of periodontal disease.
The plate must be worn at least 22 hours a day, removed when eating and performing hygiene procedures.
Orthodontic trainers
These devices, made of polymer material, are installed on two jaws and allow them to influence not only the teeth, but also the jaw muscles.
During the process of occlusion correction, the patient changes elastic trainers to more rigid ones as needed.
This allows you to get rid of such pathologies as shifting of individual teeth, increased tone of the chin muscles, and loose jaw contact. The duration of treatment with trainers is usually 1.5-2 years.
When it is not possible to correct a malocclusion using various devices, dentists resort to a more radical method - the method of surgical correction.
It is indicated when therapeutic and orthodontic treatment is ineffective. The essence of the method is to make an incision into soft and bone structures and move certain elements to the required position.
Surgical intervention can be used both for congenital anomalies in the structure of the jaw rows, and due to their deformation as a result of injuries.
Preventive actions
The formation of a physiologically correct permanent bite largely depends on the person himself.
Therefore, dentists recommend adhering to the following recommendations:
- to refuse from bad habits;
- adhere to proper nutrition to ensure that the body receives a sufficient amount of micro- and macroelements;
- promptly eliminate oral diseases to prevent tooth displacement;
- take measures to prevent the development of calcium deficiency, which negatively affects the condition of the teeth;
- carry out hygiene measures regularly and efficiently;
- Visit the dental office in a timely manner to identify developing diseases of the teeth and gums.
Additional information on the topic of the article is presented in the video.