We treat open bites without surgery or tooth extraction!
What is an open bite | Reasons | Treatment | Our advantages | Doctors | Reviews
An open bite is the most disliked anomaly by orthodontists, because it is very insidious and thankless in treatment.
Seriously, the diagnosis of open bite is a misdiagnosis. A bite is, by definition, the closure of the teeth. And with an “open” bite there is no closure. Therefore, it is correct to call this pathology vertical disocclusion. Disocclusion is the lack of closure of teeth. And vertical - because in the vertical plane.
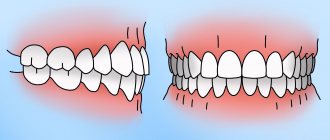
Such disocclusion can occur in any segment of the dentition. But most often it occurs in the frontal (front) area, that is, in the area of the incisors. Therefore, an even more complete name for this problem is vertical incisal disocclusion. It is characterized by the fact that only the lateral teeth close together, while the front teeth “hang” (do not close) and do not close vertically.
Vertical incisal disocclusion. Front view.
Vertical incisal disocclusion. Side view.
This is the reason for the “insidiousness” of this anomaly and the dislike of orthodontists for it. The fact is that open bite causes a huge number of relapses. That is, the treatment of vertical disocclusions in a huge number of cases is very unstable and all for one reason: there is no method, there is no apparatus that consolidates the success of treatment in the vertical plane. It’s the custom with orthodontists... If you’ve done it (cured it), fix it (just in case...). And it is right. Therefore, after any orthodontic treatment, retention devices and structures are installed. For anomalies in the sagittal plane, be it distal occlusion or mesial occlusion, such retention devices are available. There are also problems in the frontal plane (narrowing of the dentition, crossbite). But not in the vertical plane.
And therefore, in achieving a successful and stable result in the treatment of an open bite in an adult, it is very important to initially understand the reason for the occurrence of non-occlusion of the teeth vertically, in each specific case. After all, only by identifying and eliminating the cause can we “defeat” this most unfortunate and insidious open bite. No relapse. Once and for all.
Diagnostics is the first and key step in the treatment of open bite. Do you want to know why it’s impossible to do without diagnostics?
But, precisely, the reasons for vertical disocclusion are usually considered very simplistically and superficially. And is this why there are so many failures in correcting open bites?
Chapter 10. ANOMALIES OF DENTAL OCCLUSION
Anomalies of the teeth and jaws lead to disruption of the closure of antagonist teeth (i.e., the occlusion becomes incorrect). Violation of the closure of antagonist teeth occurs either in one of three directions (sagittal, transversal and vertical), or simultaneously in two or three directions.
The closure of the dentition in the lateral and anterior areas should be considered (Table 10.1).
Table 10.1.
Types of occlusion anomalies in the anterior and lateral areas of the dentition
| Direction (plane) of the malocclusion | Area of the dentition | Types of occlusion |
| Sagittal | Side | 1.1. Distal occlusion 1.2. Mesial occlusion |
| Front | 1.3. Disocclusion 1.4. Reverse occlusion 1.5. Reverse disocclusion | |
| Vertical | Side | 2.1. Disocclusion |
| Front | 2.2. Incisal vertical disocclusion 2.3. Direct disocclusion 2.4. Deep incisal occlusion 2.5. Deep incisal disocclusion | |
| Transversal | Side | 3.1. Cross occlusion 3.1.1. Vestibulocclusion 3.1.2. Linguistic occlusion 3.1.3. Palatine occlusion |
| Front | 3.2. Transversal incisal occlusion 3.3. Transversal incisal disocclusion |
In the lateral areas, the normal closure of antagonist teeth corresponds to Angle class 1, when each tooth occludes two antagonists.
In the case when the lower dentition is shifted back relative to the upper one or the upper one is shifted forward relative to the lower one, and the teeth in the lateral areas close according to Angle’s 2nd class, a distal step is formed between the antagonist teeth with the formation of distal occlusion (Fig. 10.1).
Rice. 10.1.
Distal occlusion of the dentition
Mesial occlusion of the dentition is formed as follows: the lower dentition moves forward relative to the upper or the upper dentition moves backward relative to the lower dentition. In both cases, the teeth occlude according to Angle's 3rd class with the formation of the mesial step (Fig. 10.2).
Rice. 10.2.
Mesial occlusion of the dentition
Closing of anterior teeth with distal or mesial occlusion.
With distal occlusion as a result of protrusion of the upper anterior teeth or retrusion of the lower anterior teeth, their closure is absent, i.e. disocclusion of the anterior group of teeth is formed.
With mesial occlusion, there is an inverse relationship between the upper and lower groups of teeth: retrusion of the upper anterior teeth and protrusion of the lower ones leads to disocclusion (reverse incisal disocclusion). If, with the reverse relationship of the anterior group of teeth, closure exists, then this is diagnosed as reverse incisal occlusion (see Fig. 10.2).
Causes of open bite
One of the most common causes of open bite is the presence of bad habits in children. For example, such as: using a pacifier for a long time, placing the tongue between the teeth, sucking a finger or pencil.
A bad habit is putting your tongue between your teeth.
A bad habit is thumb sucking.
And it seems difficult to argue with this. Because mechanical impact on the dentition, of course, can lead to vertical disocclusion. But! This is a very superficial look at the cause of open bite. After all, thumb sucking and tongue thrusting are more likely a consequence than a cause.
And the cause of vertical disocclusion is always cranial problems (see “Cranial distortions”), that is, problems with the position of the cranial bones. And the resulting cranial dysfunctions are always reflected in the jaws (from which the teeth “grow,” as is known).
Treatment in installments
The Orto-Artel clinic offers installments for the entire process of treating any disease. Personal conditions are considered on an individual basis.
Find out more
or call 8 (495) 128-11-74
This is confirmed by thumb sucking in the womb. What bad habit are we talking about here? A bad habit is something acquired, something that appears throughout life. And thumb sucking while still in the mother’s womb is a subconscious act by which the child unconsciously tries to ensure the stability of the cranial bones. Thus ensuring the functionality of the cranio-sacral mechanism (for those who don’t know what it is, look at Wikipedia). After all, this mechanism is the most important factor ensuring the normal functioning of the central nervous system (CNS). That is, the main “computer” of the entire organism, regulating every single process taking place in it. And that is why every effort is being made to ensure the stability of this “computer”. Even in such a simple way as thumb sucking.
- Thumb sucking in utero during an ultrasound examination.
- Thumb sucking in early childhood, as a continuation of point 1.
- The figure clearly shows how the child unconsciously stabilizes the entire maxillary complex and adjacent cranial bones.
- As a consequence of cranial problems and “bad habits”.
As we see, tongue protrusion simply cannot but occur with such a vertical “gap” between the upper and lower teeth.
The tongue is too “curious” an organ to ignore such a tempting “hole”. And accordingly, tongue insertion, as well as insertion of other objects (including fingers and pencils), only aggravates the problem. That is, it is a “related product”.
Occlusion disorders: types, classification and treatment options
An incorrect bite is not as harmless as it may seem to an ignorant person, who considers the gap between the teeth to be simply an individual feature. Occlusion that is far from normal affects the beauty of the smile, disrupts the harmony of the face, and increases the load on the temporomandibular joints, which ultimately leads to health problems. This means that defects must be corrected as early as possible with orthodontic treatment.
The type of malocclusion depends on how the dentitions close; all anomalies are considered in three directions - sagittal, vertical and transversal.
Formation of occlusion with reduction of potential functional risks
Occlusion is often perceived as a difficult condition to achieve because the variability in clinical success or failure of its restoration largely depends on the individual needs of the patient. In cases of a wide range of adaptation, the possibilities of iatrogenic interventions are significantly expanded to achieve a comfortable occlusion. With a narrow adaptive range, the rehabilitation process becomes very complex indeed: sometimes the changes are so great that one strip of articulation paper is not enough for an adequate diagnosis. In this article we will look at the problems that the doctor faces in creating an adequate occlusal position of the jaws in patients with high risk of potential functional complications.
Analysis of high-risk signs in addition to the main symptoms of the disorder
One of the main difficulties in assessing occlusion is that it is necessary to use more than just the methods of a routine clinical examination to fully diagnose the risks. Indeed, to identify risk, it is necessary to analyze not only the existing expressed symptoms, but also individual signs of pathology. Sometimes, before the start of dental treatment, the patient may be characterized by the presence of low risk indicators, while any treatment provokes a change in the usual occlusal pattern and leads to a progressive increase in the corresponding negative parameters. Once the risk distribution is fully understood, further treatment should be aimed not only at restoring the appropriate occlusal pattern, but also at reducing the potential for future development of the initially diagnosed risks. The key problem is that any dental intervention can disrupt the patient's stable state of occlusion to which he has already adapted. To achieve a certain goal, the dentist must predict the amount of necessary corrections and changes in contact between antagonist teeth. Thus, reasoned correction of occlusal relationships helps not only to stabilize the functional state of the tooth-jaw apparatus, but is also part of the prevention of the development of potential risks into possible actual complications. The risks of occlusal complications can be expressed through disorders in the joint area (photo 1), masticatory muscles (photo 2), in the form of pathological abrasion (photo 3), chips and fractures of teeth (photo 4).
Photo 1. Palpation of the temporomandibular joint
Photo 2. Muscle palpation
Photo 3. Type of tooth wear.
Photo 4. Tooth fracture
The reasons for such symptoms are not that the teeth are in principle in contact, but in the degree of their interaction with each other. Parafunction is a condition in which the interaction of teeth occurs outside the boundaries of normal function. Essentially, problems with joints and muscles are determined by the time of presence of the disorder and the force of interaction, which is formed under parafunction conditions. To minimize the degree of functional disorders of the dentofacial apparatus, the first thing the doctor must do is to reduce the time of activity of the patient’s parafunctional activity. It is logical that to perform this task it is best to use methods that provide the most predicted result, but, unfortunately, even the most careful forecast sometimes does not meet expectations. If it is impossible to exclude the patient’s behavioral pattern, in the structure of which parafunctions are manifested, and to reduce the patient’s activity time in this state, it is necessary to at least minimize the effect of the forces that are formed during such a violation. Minimizing the emerging forces will reduce pressure on the joint and muscles, and will also prevent further progression of pathological tooth wear.
Two methods that minimize parafunction disturbances
To minimize the forces exerted during parafunctional activity, clinicians can use two methods: (1) directly reducing the applied force or (2) more adequately distributing the forces over a larger surface area. The latter method minimizes the force per square millimeter, thereby reducing damage to the cutting and occlusal surfaces of the teeth. To better understand the principle of reduction of acting forces, it is necessary to take into account the specificity of the action of the muscles that raise the lower jaw. The masseter, anterior temporal and medial pterygoid muscles act from a neurological impulse when compressing the distal teeth, and take part in transmitting pressure on periodontal tissue. Roughly speaking, this is how periodontal nerve cells communicate with the brain. Analyzing their signals, the brain begins to activate the corresponding muscle structures. When the function of the teeth contacts is impaired, the muscles continue to generate a certain activity, thereby provoking excessive clenching of the teeth. It is logical that in order to reduce the force transmitted to the joints, which are the weakest link of the dentofacial apparatus, it is necessary to reduce the activity of the masticatory muscles. First of all, by reducing the contact of the distal teeth (photo 5).
Photo 5. Disocclusion in distal areas
The success of canine insertion is not based on the inclusion of the canines in the occlusal scheme, but on the exclusion of contact between the teeth behind the canines. A doubling of muscle activity is observed already when the contact passes not only to the canine area, but also to the area of the first premolar, and when the contact reaches the second molar, muscle activity, according to EMG data, increases 5-10 times. The amount of force applied will depend on the size of the muscles and the unique muscular system of each individual patient. Leveling contacts in the area of premolars and molars leads to a decrease in the activity of the masticatory muscles, and therefore to a reduction in the force parameter that is generated by them. The occlusal contacts should then be spread over a larger area, similar to the principle of using snowshoes or more wheels for oversized trucks. The determining factor in such situations is the force per square millimeter of space. To calculate the force applied, variables such as weight, force, and surface area must be taken into account. To reduce the force per square millimeter, the total surface area must be increased. In this way, it will be possible to reduce the level of applied force to such a low level that tooth abrasion will take on a non-destructive form. It is logical that such an approach promotes biological protection of the joints, as well as a reduction in muscle-associated symptoms such as headaches, muscle fatigue while eating, and painful muscle strains. Relief of these symptoms returns the patient’s adaptive ability, ensuring the prevention of damage not only to teeth, but also to existing restorations. Thus, leveling the contacts in the area of the distal teeth during articulatory excursions helps to reduce the applied parafunctional forces, and increasing the area of contact of the teeth in the initial position helps reduce the load on a particular tooth (photo 6). Clinical methods for achieving similar results are described below.
Photo 6. View of the contacts present
Materials, tools and approaches for occlusion design
Equilibration in centric relation for repositioning and recontouring of the occlusal scheme
The term “equilibration”, as used in this publication, is defined as the process of reduction or recontouring of teeth, that is, what is normally referred to as enamel or odontoplasty. This term may also include the performance of restorations such as minimally conservative composite fillings, inlays or onlays. Equilibration also includes reposition, which in orthodontics is defined as the movement of teeth to a different position relative to each other, or their controlled disposition during orthognathic manipulations. According to the author, repositioning should involve minimally invasive interventions to correct occlusal relationships. The first step in equilibration is to use models fixed in the articulator to design the centric relation (also referred to as the “seated position of the articular head”) (Figure 7).
Photo 7. First point of contact on the plaster model
In the centric relation, it is possible to determine how the teeth of the lower jaw relate to the teeth of the upper jaw when the articular head is in the most comfortable position. In addition, the analysis of models in the articulator makes it possible to analyze the nature of movement and features of the interaction of teeth with different types of excursion of the lower jaw, as well as in the state of maximum fissure-tubercle contact. During equilibration, you also need to pay special attention to how the incisal edges of the teeth are compared, since during parafunction they can be subject to the greatest damage. In order to achieve equilibration, strips of articulating paper of different thicknesses can be used, from 20-24 to 90-200 microns. This variation in paper thickness allows for very precise determination of changes in the patient's occlusion. As shown in Photo 8, red marks identify excursion movements, and green, black or blue mark intercuspid stops.
Photo 8. View after registering the bite using articulation paper
Better than articulating paper, of course, is foil-based film, which more accurately helps to verify dispositions and contacts. Equilibration can be carried out using polishing strips or a finishing diamond bur. For very fine corrections, different types of grinding tools based on white or Arkansas stone are used. Some clinicians prefer to use special aesthetic trimmer burs for the same purpose. In any case, the main thing is to achieve adjustment and adequate polishing of the tooth based on the available instruments. To achieve adequate position of the articular head, a sheet calibrator can be used, which is a set of plastic spacers one-tenth of a millimeter thick, which are secured with a polytetrafluoroethylene clamp. To identify the first point of contact, a sufficient number of strips must be placed between the anterior teeth, thus creating disocclusion in the distal areas; After this, the patient should move his jaw back and forth, and then squeeze the calibrator strip with his teeth (photo 9). The sheet calibrator eliminates the need for bilateral manipulation and the use of composite in the distal teeth to form a Lucia jig.
Photo 9. Leaf calibrator to achieve centric ratio
Treatment planning and adjustment of three occlusal relationships
Occlusion design is based on three variables:
- minimizing the applied force,
- minimizing the activity of the muscles that lift the mandible,
- and creating conditions for the distribution of force on the front teeth.
The lower teeth contact the upper teeth in three ways: (1) through maximal fissure-tubercle contact (Figure 10), (2) through cusp-to-cusp contact (Figure 11), and (3) through interaction during mandibular excursions (Figure 12). .
Photo 10. Maximum intercuspid position (maximum fissure-tubercle contact).
Photo 11. Position of the jaws when the cutting edges of the front teeth contact.
Photo 12. Position of the jaws during excursion.
The classic treatment approach begins with determining the position of maximum fissure-tubercle contact. But in some situations it is necessary to start with an analysis of the “tubercle-to-tubercle” contact, and this should be carried out after achieving the fissure-tubercle contact and further excursion, after which the necessary type of “tubercle-to-tubercle” interaction is formed. When planning treatment in the aesthetic area, the desired position of the upper incisors is determined by the position of their cutting edges in the structure of the overall facial profile (photo 13).
Photo 13. View of teeth with free lips.
The position of the lower front teeth is formed to achieve edge-to-edge contact. If there is a need for a crown lengthening procedure, then this manipulation should be performed before occlusal corrections to achieve maximum fissure-tubercle contact. That is, aesthetically-oriented interventions are first performed, and only after that the occlusion “tubercle to cusp” or “edge to edge” is recreated. The goal is to result in the formation of wide, flat contacts when the upper and lower teeth touch their edges, or incisal areas, in a protrusive position and lateral movements (Figure 14). Maintaining the incisal spaces allows the lower teeth to move freely during excursion (Figure 15). Recreating disocclusion at the distal site reduces the amount of force the patient can generate during parafunction. For this purpose, you can use a red articulating 40-90 micron strip in the frontal area with maximum coverage of the cutting edge.
Photo 14. Crossbite.
Photo 15. Shape of interdental spaces.
Once edge-to-edge occlusion has been achieved, the next step of treatment is to achieve maximum fissure-tubercle contact. In this case, all teeth must contact the antagonists while maintaining the appropriate position of the articular head. Taking into account the central ratio, the necessary position of the lower jaw becomes clear to the doctor. Correction of occlusion based only on the position of maximum fissure-tubercle contact can only help move the jaw to another position, which can also inherently remain destructive in relation to muscles, joints and teeth. In conditions of already affected areas of the joints that cannot achieve full compensation, it is necessary to proceed from individual clinical capabilities, taking into account the limited adaptive potential of the patient. In such cases, it is necessary to achieve uniform light contact between the teeth, regardless of whether they are in contact during excursion or under conditions of strong compression. In this case, the loading of the teeth should occur only along the long axis, and separate inclined contacts are undesirable. The tilt of the teeth in any direction opposing the articulatory movement can provoke fracture of the tubercle. The classical occlusal scheme assumes the absence of a sliding effect with an adequate position of the articular head, and in order to achieve contact between all teeth, the movement of the lower jaw must be projected along the usual and non-stop articulatory path.
Articular head position and contact design methods
There are three options for choosing the position of the articular head. The formation of a particular one is based on the parameters of muscle activity, the position of the teeth and the plan for future orthopedic treatment. It is impossible to accurately determine the required position of the articular head and disc in the glenoid fossa, so the clinician must proceed from the understanding that the patient constantly bites in approximately the same position and can adapt to small changes in the occlusal pattern. Intercuspid position is predictable when treating a small number of teeth, in particular those that are not characterized by a higher risk of functional complications compared to others. The patient illustrated in this article did not experience significant tooth wear. If the patient has a higher risk of functional complications, the number of teeth requiring replacement exceeds the permissible norms, or the teeth requiring treatment are those that determine the main degree of functional risk (for example, a tooth that is the first point of contact, with adequate articular position heads) centric relation parameters should be used to correct occlusion. The physician must also ensure that, in terms of anatomy and the risk of possible inflammatory complications, the articular head-disc complex is functionally stable. In patients with significant decompensation of the temporomandibular joint, the required occlusal position should be determined directly during treatment, since it may differ from the previously compromised centric relation. It is necessary to understand that, based on the maximum fissure-tubercle contact, we can predict the functional stability of the teeth themselves, based on the central relationship - the position of the disc and the articular head, based on the position determined during the treatment of a patient with joint disorders - the state of the muscles, corrected by the contact of the teeth . Indeed, often, when the centric relation or muscle-oriented position of the jaws is achieved, the doctor has to re-form the occlusal pattern of tooth contact with the maximum number of points of contact. In any case, correction of the occlusal scheme should be minimally invasive, based on known recontouring techniques. Based on the maximum fissure-tubercle contact, the adjustment process begins from those teeth that are already in contact. The goal is for the posterior contacts to look like those on the mandibular buccal cusps and distal marginal ridges, forming the first class of occlusion. Correction in patients with the second or third classes of occlusion will be carried out in slightly different positions, restoring three-point contacts of the teeth, or cusp-fissure contact to distribute the load along the long axis of the tooth. To form such contacts according to the cusp-fissure type, it is logical that it is necessary to ensure the use of at least two initial markers - a burgh and a fissure. The contact itself should be designed on the top of the cusp, and the area receiving the load should be on a flat surface (photo 16).
Photo 16. View after checking occlusion with articulation paper.
Contacts that are formed at an angle should be excluded. When biting, the loads should be in an exclusively longitudinal direction, since their oblique projection provokes corresponding periodontal complications. Once the “correct position” of the teeth, occlusal planes and curves of Spee and Wilson are achieved, there is a high chance that this occlusal scheme has a good prognosis, and may even be considered aesthetically acceptable. When reaching contacts between teeth, it should be remembered that the load is distributed evenly between the antagonists, therefore, correction should also be carried out in the area of both teeth, achieving the required shape. If one of the teeth is planned to be restored, then the correction should be carried out only on it, taking into account that its occlusal surface will still be adapted prosthetically in the future. Test equilibration is performed using an articulator. Before articulating the models, it is also necessary to determine which teeth will be removed in the future. These teeth should be marked with an X on the model. The doctor must also indicate on the model which teeth will be restored using prosthetic restoration. For each of these restorations (inlays, onlays, crowns) there are specific designations. At the same time, the doctor must remember that some reduction of teeth in the laboratory that are subject to further orthopedic rehabilitation is carried out in order to take into account the portion of wax that is used during the modeling of different types of structures.
Contact adjustment and postural shift control
One important point when considering adjustments to teeth or a model (or teeth on a model) is that intercuspal position will subsequently influence disclusion during excursive movements of the jaw. During the adjustment, two teeth are always involved: one protrudes into the contact area as the tip of the cusp, the second as the area that receives the load. If the cuspal apex is shortened, the clinician must also ensure that excursion interactions are eliminated, thereby relieving distal disocclusion. When modifying the receiving area, the problem is more complex, since deepening the fissure does not in any way facilitate either excursion or lateral movements of the jaw. One way to study the necessary information about jaw displacement is to analyze the protrusive (lateral) movements of the jaw in a semi-adjustable articulator, thus suggesting the possible position of the articular head in the fossa. The doctor can study how much space is thus formed between the teeth, and what is the degree of true disocclusion. During the implementation of such a method, however, it is difficult to make a mistake on which side should be shortened or shifted the top of the tuberosity, and on which side the fissure area should be deepened.
The process should be repeated until the contacts are adjusted enough to appear uniform and provide longitudinal load transfer to the tooth. The answer to the question of whether correction should be continued until full contact is achieved between all front teeth depends on several factors. If the patient has an anterior open bite, stability of the condition should be assessed. If a lack of contact occurs after recently completed orthodontic treatment, the teeth may move slightly to form the necessary contact, as this condition is inherently unstable.
In parallel, the doctor must answer the following questions:
- Is it necessary to continue correction until the contact between the canines is formed, if the goal of treatment is to achieve the canine route of insertion, and in the existing conditions the canines are not in cusp-fissure contact?
- Is it necessary to carry out a complete restoration of the teeth, or does the treatment plan involve restoration of only the incisal edge, or the vestibular incisal third of the lower anterior teeth?
- Are there plans to restore the lingual side of anterior teeth affected by wear, erosion or abrasion?
- Does the patient have older restorations with pre-existing occlusal height deficits?
If it is necessary to carry out restorative interventions in the area of the anterior teeth, the doctor must analyze the specifics of the excursion from the point of first contact to the point of stable cessation of movement. In the course of such an analysis, it may be determined that the restoration should be postponed to a period of time when it is possible to achieve excursion stopping points in the distal areas, which will ensure axial transmission of the masticatory load. If the canine route of insertion is to be achieved, a stable stopping point must be formed on the canine. Thus, with maximum fissure-tubercle contact in the area of the anterior teeth, slightly less intense stable stopping points may be observed, which may even go somewhat out of the general occlusion. It is also necessary to remember to control postural displacement (under the influence of gravity). Most equilibrations are performed with the patient lying in the dental chair. Therefore, when checking occlusal transmission, the patient should be positioned in a sitting position and checked for new complex contacts in the frontal region that may arise as a result of gravitational distribution on the moving system of the mandible. To check contact in the frontal area, you can use the jitter effect. The doctor can place a finger on the vestibular part of the front teeth, and asking the patient to clink his teeth, determine the presence or absence of vibration in these teeth when biting. If there is vibration, the contacts between the front teeth can be loosened a little. In general, the use of tremor testing, as opposed to articulating paper correction methods, helps to adapt dental occlusion for adequate postural movement during function.
Correction of excursion movements: canine route of insertion or group function
The final occlusal positions that need to be adjusted are the excursion movements (right, left, and protrusion). The introduction scheme is determined by which teeth should be in contact during excursions of the lower jaw. These contacts become working ones. All other teeth should be removed from contact, as they will disrupt the normal course of jaw movement, thereby causing muscle hyperreactivity. There are two methods for adjusting excursion movements. The first is the formation of a canine path of insertion, that is, in this case, when the jaw moves to the left or right, the canines are the only teeth that are in contact. In this case, the distal teeth do not touch either the working or balancing sides.
The advantage of canine insertion is that the activity of the levator mandibular muscles is minimized since the distal teeth are completely separated. The disadvantage of this approach is that the entire load falls on the fangs, and in their absence, the implementation of such an algorithm becomes more complicated. Of course, the problem can be solved by installing an implant in place of the fang, but not always. On the other hand, if the canines have been previously endodontically treated, they may no longer provide adequate stability support during canine insertion. If it is not possible to achieve canine insertion (with class II occlusion, for example), you can use the group function. The latter involves the inclusion of teeth only on the working side. The term balanced occlusion is a condition created by the dentist in which the teeth are in contact on both the working and non-working sides. The group function involves contact of more than one tooth on the working side, such as a premolar and a canine, or both premolars and a canine, or all teeth up to the second molar. The more teeth are included in occlusion in the distal area, the greater the force generated by the masticatory muscles. At the same time, the group function does not essentially increase the clenching force, but only helps to simultaneously distribute it over several teeth, and thus change the load on the joint area.
You should also consider the protrusive movement, in which the jaw moves forward while balancing relative to the midline. In this case, the contacts on the left and right sides relative to the middle line should look the same. During protrusive movement, the doctor himself determines the starting and final point of movement in the area of the central teeth, ensuring disocclusion of all the others. The doctor can also correct the movement starting from the fangs and moving it to the incisor area. The distal teeth are also in a state of separation. In rare cases, protrusion can begin from the premolar area, which sometimes happens in patients with class II relationships. Personally, the author uses red articulation paper to analyze excursion movements. The intercuspid stop areas must be re-marked before any corrections are made, since marks from other colored articulation paper (green, blue, black) may simply overlap the red registration points. Areas where the red markers are not overlapped by any other color are excursion areas. Excursion movements can be marked using paper 200 microns thick, so the doctor will know for sure that these contacts need to be leveled. Paper 40-90 µm thick can be used to mark intercuspid contacts. The use of articulation paper of different thicknesses allows the doctor to differentiate the areas of thin and complex contacts in different positions of the jaw. After correction, all areas must be thoroughly polished.
conclusions
The principles described in this article are valid when performing single restorations, total occlusal rehabilitation, or when treating patients with temporomandibular joint disorders. The approach is similar when restoring occlusion after orthodontic treatment. Reducing the level of muscle activity through the appropriate distribution of contacts, achieving the maximum fissure-tubercle ratio and the formation of adequate excursion movements are topics that should be taken into account at all stages of occlusion correction. The formation of a physiological occlusal scheme is possible with sufficient justification for certain iatrogenic interventions, the implementation of optimized approaches, the selection of precise methods, extensive visualization and the provision of appropriate instruments.
Posted by Lee Ann Brady, DMD
Sagittal malocclusions
Sagittal abnormalities include mesial and distal bites.
- A mesial (progenic) bite looks like an extended lower jaw, which forms a kind of step. In this case, the upper incisors overlap the lower ones, and an abnormal occlusion is formed. There may be several reasons that provoke the appearance of a mesial bite: birth trauma and respiratory tract diseases, genetic features of the structure of the jaws and problems with artificial feeding, a short frenulum and a violation of the size and shape of the tongue.
- A distal (prognathic) bite visually looks like a protrusion of the front row of teeth, due to which the upper jaw appears overdeveloped. With a detailed study of the pathology, it is possible to diagnose difficulties with closing teeth, detect a clearly defined chin fold, and record a visual enlargement of the nose.
Sagittal malocclusions can be temporary or permanent. Temporary ones can occur in preschool children with a dentition of about twenty milk teeth. To eliminate violations, orthodontists use stimulation of the growth of an underdeveloped jaw or retardation of the development of an overdeveloped jaw, and correct the area where the teeth should meet using various methods.
Vertical dental anomalies
Vertical malocclusions are characterized by teeth that are too high or too low, causing the jaws to fail to close. In case of vertical deviations from the norm, insufficient or excessive height of the dentition may be a consequence of incomplete teething, elongation of the tooth in the lower jaw due to the prolonged absence of an antagonist in the upper jaw (and vice versa). These manifestations depend on a number of etiological factors provoking the disorder, on the severity and the immediate area of the dentition - the localization of the disorder.
A characteristic type of vertical anomaly is disocclusion - when trying to close the upper and lower jaws, a noticeable gap is formed, which does not allow chewing food thoroughly, interferes with the reproduction of individual sounds and the development of correct speech in general. Orthodontists distinguish between anterior and lateral disocclusion, bilateral and unilateral, true and false, gnathic and dentoalveolar. And they consider it one of the most difficult malocclusions, difficult to correct.
When treating vertical anomalies in children, the doctor first of all tries to eliminate the etiological factors - the root cause of the disorders. As for disorders in adults, they are treated with removable aligners and fixed orthodontic appliances, with the help of Angle arches and Katz guide crowns.
Transversal anomalies
Transverse occlusion disorders are characterized by disproportion of the dentition - the upper one is much narrower than the lower one or vice versa. Sometimes this discrepancy is complicated by lateral displacement of the jaw. A typical representative of a transversal anomaly is a cross bite, which is also sometimes called a scissor bite.
Once a doctor diagnoses a crossbite, treatment begins immediately to prevent asymmetrical development of the facial skeleton and temporomandibular joints. A patient with a crossbite undergoes opening of the dentition. In the case of excessive narrowing of the jaw in adults and children, plate devices with the possibility of expansion, with special mobile screws and strong springs on the trays, are installed. In some cases, these devices have an inclined plane, which is more efficient. Modern activators and regulators of Frenkel functions are also used.
All these measures must be taken promptly, otherwise the anomalies will become more pronounced, the deformities will become more complex, and surgical intervention will be required to correct the abnormalities.
Modern practices in the treatment of occlusion disorders in Moscow
It is easier to prevent a malocclusion than to treat it later - hardly anyone will argue with this. Therefore, experts strongly recommend that parents of babies closely monitor teething, avoid disturbances in feeding, maintain physical activity, and consult a doctor promptly if the first signs of respiratory tract diseases or poor posture occur. Prevention helps to minimize risks and prevent the development of malocclusion. But if the moment was missed, and the dentist diagnosed a violation of occlusion, the sooner the visit to a specialist, the better.
In childhood and adolescence, the maxillofacial region of the skull is just forming, and therefore this time is considered the most favorable for the treatment of malocclusions. Correcting occlusion in adults takes longer, but this does not mean that the goal will be partially achieved, or even not achieved at all. Occlusion can be corrected at almost any age - this is guaranteed by modern technologies and the skill of orthodontists.
To determine the severity of the anomaly, the orthodontist measures the distance that separates the point of closure of the teeth from the norm. The magnitude of this distance determines the degree of malocclusion.
- I degree - no more than 5 millimeters of closure separation;
- II degree - from 5 to 9 millimeters;
- III degree - over 9 millimeters.
But this is not the only way to determine the complexity of the upcoming task. The doctor may invite the patient to chew a special mass in order to assess the quality of chewing food, consider the result, calculate the percentage of grinding and draw a conclusion about the use of certain treatment methods.
Only after determining the type and degree of curvature of the dentition and establishing the causes of the disorder, the doctor will prescribe treatment, focusing on the patient’s age and general health.
If there are malocclusions, but they are mild, treatment can be reduced to recommendations from the doctor, which the patient will follow independently. If the appearance of the dentition is noticeably deformed, the functions of chewing and speech are impaired, the treatment will be more intensive.
In any case, the treatment regimen is selected individually, taking into account the structure of the patient’s dental apparatus and the degree of impairment. The duration of treatment is also determined individually.
- During the period of changing teeth and temporary occlusion (children under 12 years of age), orthodontists use myogymnastics and removable orthodontic devices of mechanical action.
- In the treatment of adults and adolescents over 12 years of age, modern braces and other orthodontic structures of varying levels of complexity are used.
- In the most difficult cases (with traumatic occlusion, for example), surgical methods can be used - alone or in combination with orthodontic structures.
Deep incisal overjet, deep bite, deep traumatic bite
Treatment of deep bite
Treatment tactics depend on the form of deep bite, but the main tasks are as follows:
- promote dentoalveolar elongation in the lateral areas of the lower jaw, stimulate the eruption of chewing teeth by separating them,
- create a distal inclination of the lateral teeth,
- elimination (intrusion) of an existing dentoalveolar elongation in the anterior region or delay in the eruption of anterior teeth,
- when retruding the anterior teeth, create their vestibular inclination,
- in case of sagittal discrepancy of the dentition, correction of prognathia (more often) and progenia.
Treatment is carried out in various ways and methods, taking into account the pathogenesis of the clinical form of the anomaly, the age period (deciduous, mixed, permanent dentition). During the period of primary and early mixed dentition, it is necessary to normalize nasal breathing, eliminate existing bad habits, and perform myogymnastics. The following exercises may also be recommended:
- slowly push the lower jaw forward until the cutting edges of the lower incisors are positioned in front of the upper ones; hold in this position for 10 seconds, then slowly return to the starting position;
- A rubber tube is put on a wooden stick and placed between the front teeth, which are compressed and unclenched. Considering that a deep bite is often combined with a distal bite, you can add exercises from the corresponding complex.
In case of defects in milk teeth, their timely elimination by filling or prosthetics with inlays; in case of premature removal of milk or permanent teeth, prosthetics with appropriate structures or the use of devices that help preserve space for teeth that erupt later.
To eliminate a deep bite with a neutral relationship of the dentition (I class according to E. Engle), plates with a bite platform are used. The authors consider it necessary to emphasize that not with an inclined plane, but with a bite platform, since this does not require moving the lower jaw forward, but only a vertical adjustment of the bite. To prevent the lower jaw from moving forward or to the side, it is better to make the bite pad not smooth, but with imprints of the antagonist teeth. The most optimal way to fix a removable device is an Adams or A. Schwarz clasp, which are made of wire with a diameter of 0.8 mm.
The effect of these devices is manifested when biting with the lower front teeth in increasing the load on them, as a result of which the bone tissue of the jaws is rebuilt and dentoalveolar shortening occurs in this area. At the same time, the lateral teeth become separated and their dentoalveolar elongation (extrusion) occurs due to the fact that stratification (apposition) of bone tissue occurs over the entire periodontal surface of the sockets. Therefore, the ratio of the inside and extra-alveolar parts of the lateral teeth does not change significantly, since the teeth do not move forward, but grow together with the alveolar process towards each other on both jaws. However, more often only the lower teeth need to be moved. The bite block must be used constantly, and this must be continued to avoid relapse, even when the normal vertical dimensions of the lower third of the face are restored.
Vertical movement of teeth is possible due to intermaxillary traction, lever-like action of arches, the potential force of the NiTi arch itself, and compensating bends. In a mixed bite, a utility arch, rectangular, with a diameter of 0.40 x 0.40 mm, in brackets with a groove of 0.45 mm (0.18 inches) can be used to move teeth. But when using it, great caution and careful monitoring should be observed.
G.B. writes about risk factors and the need to control the amount of force. Ospanova, discussing the problem of root resorption during vertical movement of teeth, in particular with the help of an intrusive utility arch. Since only the first molar is used as a support, it is necessary to ensure that there is no significant extrusion of it. Due to the significant length of the arc, the load is dissipated and the initial force of the intrusion is weak, but its activation when placed in braces increases the force on the incisors, in particular in the direction of their vestibular inclination. This can be avoided by additionally creating oral torque on the incisors, but this will increase the extrusion of the molars. If you bend the utilitarian arch over the distal end of the tube on the molars, then their mesial displacement is possible, which is also undesirable. Therefore, it is better to wait for the formation of a permanent bite and then use intrusive arches. For complete optimal control of the anterior and lateral segments, the use of purstone segmental arches can be recommended.
If there is retrusion or crowding of the anterior teeth, it is necessary to first eliminate these disorders, and then proceed directly to deep bite therapy. Previously, and even now, removable devices with protracting springs are used for this purpose. Currently, if it is planned to use functional devices in such patients, and it is impossible to immediately move the jaw into a constructive bite position, the dentition should first be corrected using braces. The bite block does not interfere with the fixation of braces on the lower incisors.
You can first use a round wire arch to change the torque of the front teeth or heat-activated nickel-titanium arches, and then rectangular steel arches with a diameter of 0.45 x 0.45 mm. By the end of the second month, the dentition is usually aligned. In conjunction with these arches, if the deep bite is combined with prognathia or progenia, an appropriate intermaxillary rubber band can be applied while the growth process continues. As the sagittal anomaly is corrected, the incisal overlap may also decrease due to tooth extrusion. Before determining the constructive bite, the teeth should be open to better control the amount of movement. It is better to move the lower jaw forward no more than 3-7 mm, that is, until the front teeth come into direct contact.
The degree of separation of the dentition when eliminating supraocclusion of the lower and infraocclusion of the upper anterior teeth is determined by the size of the free interocclusal space. Typically, the bite pad is modeled in such a way as to separate the dentition by 2-6 mm, but this is purely individual, depending on the size of the incisal overlap and the interocclusal space at rest. With this disconnection, the chewing muscles will be in a moderate isometric contraction, and the entire load falls on the teeth in contact with the bite pad.
An Andresen activator is used, slightly modified in such a way (recommendation by W.poffit) that the linings on the upper lateral teeth and lower anterior teeth prevent their displacement in the direction of the occlusal plane, and the lateral areas of the lower jaw should not be limited in their movement. The R. Fränkel function regulator (FR1) can be effective in the treatment of deep bites with neutral occlusion of the first permanent molars.
A very important circumstance in the treatment of deep bite is the change in the inclination of the anterior teeth, since the creation of incisal-tubercular contact is considered a prerequisite for preventing the recurrence of the anomaly. Orthodontic treatment for the dentoalveolar form of deep bite, with a vertical position of the anterior teeth, is aimed at their vestibular deviation, which changes the depth of overlap. However, this is advisable in cases where the initial (before treatment) overlap was no more than 5 mm. With a larger incisal overlap, before making their vestibular deviation, it is necessary to reduce the supraocclusion of these teeth. It should be noted that with an incisal overlap of more than 8 mm, it is impossible to achieve incisal cuspal contact and depth of overlap, as with an orthognathic bite.
Orthodontic treatment of patients with deep skeletal bite is aimed at:
- change in the shape of the dentition and position of the front teeth,
- increase in interalveolar height,
- change in the depth of the incisal overlap.
Since almost all patients with this form of anomaly have a steep (vertical) position of the anterior teeth and a narrowing of the dentition, by expanding them, the orthodontist simultaneously achieves vestibular deviation of the anterior teeth, increasing the interalveolar height and reducing the depth of the incisal overlap by ~ 2-3 mm. Then, using removable and non-removable devices, grinding, you can further rebuild the vertical relationships.
With premature loss of primary molars and lack of timely prosthetics, resulting in mesial displacement of the first permanent molars, treatment is necessary as early as possible. Otherwise, the outcome of such a situation, in the absence of early treatment, is often the subsequent removal of premolars.
With an overlapping deep bite, characterized by a predominance of the size of the upper jaw, infraocclusion of the upper teeth and supraocclusion of the lower teeth of the same name, with retraction of the anterior portion of the lower jaw, a sharp inclination of the upper central incisors is often encountered orally, and the lateral ones vestibularly. The latter are often also rotated around the longitudinal axis. Patients come to the clinic not so much because of a deep bite, but more because of the incorrect position of the upper incisors. This form of anomaly in children with mixed dentition is difficult to treat, to speed it up Z.F. Vasilevskaya recommends a combined technique (surgical + orthopedic).
Schematic diagram of supervision: the vestibular part of the interdental gingival papillae on both sides of the lateral incisors is peeled off, the alveolar process is intersected with a thin fissure bur No. 3 in the vestibulo-oral direction to a height of ¾ of the length of the roots of the teeth being moved; it is necessary to ensure that the cutting line of the alveolar process is located at the same distance from the cortical plates of adjacent teeth; 5-7 days after surgery and postoperative phenomena have subsided, an arch can be applied. After moving the lateral incisors, the arch is replaced with a removable device with an inclined plane.
When treating a deep skeletal bite that is not accompanied by a change in the height of the lower third of the face, treatment is aimed at correcting the shape of the dental arches, the position of individual teeth, and eliminating supraocclusion of the lower anterior teeth. It is necessary to carry out treatment in such patients without disconnecting the dentition, preferably with the help of braces or other fixed devices.
Prosthetic treatment of patients with deep bite should be aimed at leveling the occlusal surface of the dentition by grinding and prosthetics with various structures. Indications for such treatment include:
- skeletal forms of anomaly that are not subject to orthodontic treatment and the patient’s refusal of surgical treatment;
- in the absence of a large number of teeth,
- ineffectiveness of orthodontic treatment or impossibility of its implementation for various reasons (severe general condition, remote place of residence, etc.) or refusal of the patient.
Prosthetic treatment is most effective for skeletal deep bites, when there is a large interocclusal space and it is possible to significantly change the interalveolar height. Preference should be given to fixed one-piece dentures and removable dentures with a metal base. A prosthesis with a plastic base requires more space; it is not applicable for multiple small defects or narrowing of the jaw. The same type of treatment should also have priority in cases of deep bite against the background of systemic periodontal diseases, since a prosthesis with a cast metal base allows better distribution of chewing pressure and prevents contact of the mucous membrane of the gingival margin with the prosthesis base.
In the process of orthodontic supervision of a patient with a deep or deep traumatic bite due to periodontal diseases, a partnership with a periodontist is necessary. Appliances and dentures must be modified taking into account the degree of pathological mobility of teeth and the amount of bone tissue resorption, the depth of the periodontal pocket, and the width of the attached gum. In other words, the preservation of bone tissue and the crown-to-root ratio have a significant impact on the prognosis when choosing abutment teeth for appliances and prostheses. The latter can be changed by preparing the tooth, using endodontoendossal implantation, or a specific design of removable dentures. In particular, for greater unloading of the remaining teeth with varying degrees of mobility, especially with terminal defects, it is preferable to use removable dentures with Roach clasps.
With favorable crown-to-root ratios, it is possible to regulate the load on the supporting teeth, even with a certain degree of pathological mobility, the correct distribution of the supporting and retention parts of the prosthesis, as well as the way they are connected to the base. In case of bone tissue atrophy, preference should be given to teeth with a crown-to-root ratio of 1:2.
A deep bite is often combined with other types of anomalies (most often with upper prognathism), which must be corrected before its immediate treatment. To treat a deep bite in combination with a distal bite, you can use the A.Ya. medical bite block. Katz, Andresen Goipl activators, R. Fränkel type I and II regulators, various bionators. In particular, the palters bionator, which also resembles an activator, but has practically no palatal base. In young patients with a deep bite, combined with a distal bite and a tendency to narrow the dentition, it is still better to use functional appliances than a facebow, since this sometimes stimulates growth and achieves an anterior position of the lower jaw. In addition, monoblock devices, especially the addition of additional elements (screw, spring), allow you to simultaneously expand the jaw.
Applying force to the first molars through a facebow with extraoral head or neck traction speeds up the treatment process. The choice of the type of extraoral traction depends on the nature of jaw growth and the direction of movement planned by the orthodontist during the treatment process. It should be kept in mind that when using a facebow with a cervical traction, the force applied to the maxilla will be downward and distal, and when connected to a head cap, it will be distal and upward. With their combined action and equality of forces, the direction will be purely distal, since the vertical components will be mutually destroyed, as if they are multidirectional.
Companies produce sets of ready-made face bows with intraoral components of various sizes, which should be pre-fitted according to plaster models, making the necessary adjustments. This treatment method is one of the most important components of the Vari Simplex Discipline, which uses the term “retractor” to refer to the face bow, which in turn consists of an internal and external part. The internal arch is inserted into special ring sleeves on the first molars of the upper jaw. The bushings can be placed closer to the gum or occlusal surface. In a gingival position, the advantage is that the force is applied closer to the center of rotation of the tooth, thus reducing its inclination. This position is preferable if only “distalization” of the molar is planned, without affecting the remaining teeth. RG Alexander recommends the occlusal placement of the sleeve, emphasizing its advantages: easier insertion into the tube for the patient and greater hygiene, as it is easier to clean.
The outer bow, attached to the head cap, neck strap or a combination of both, should be a few millimeters from the cheeks (5-10 mm) and end with hooks. The latter are necessary for fixing elastic or better spring rods. If the arc presses on the cheeks, the patient experiences discomfort, and if the distance is too large, it is difficult for the patient to sleep. The exception is situations when there is a need for different force effects of the arc on each side. For example, the dentitions close on one side along the first class. Angle, and on the other, according to class II, then with the latter more pressure is required and the outer arc on the same side bends almost at a right angle to the inner one. The length of the inner archwire should be slightly longer to increase the force applied to the upper first molar on that side.
The face bow (retractor) should be positioned so that the junction of the outer and inner bows is slightly anterior to the point of lip closure. It must be borne in mind that the fitting of the internal (dental) arch requires the closest attention. Sometimes it is necessary to adjust its loops, which need to be compressed or expanded to achieve this. The neck strap is adjusted in such a way that the initial force transmitted through the device is no more than 200-230 grams, and after adaptation it can be increased to 400-450 grams. After some time, the belt is pulled out and requires activation or replacement.
The patient must be taught how to use such devices and should not participate in mass games, ride a bicycle, etc., in order to avoid injury or damage to parts of the device. When using an arch, it is necessary to remember that all its sections are located in the same plane, the bends of the intraoral and extraoral parts must be symmetrical. A plastic coating is usually applied to the extraoral parts of the face bow, the color of which gives information about its size: yellow 83, pink 90, red 97, green 104, blue 111.
It should be borne in mind that in adult patients (in fact, after puberty and even somewhat earlier, in 12-14 year olds), with the action of extraoral apparatus, one can only count on the movement of teeth and partially alveolar processes; rotation of the lower jaw may also occur as a result of reciprocal action on the chin. It is useless to act on skeletal disorders in this way.
In the final period of the replacement and initial period (9-12 years) of the permanent dentition, they strive to use physiological processes in the formation of occlusion. The same orthodontic devices are used, but emphasis can also be placed on fixed devices: A. Katz guide crowns, E. Engle arches, brace systems.
In permanent dentition, it is advisable to carry out sequential disocclusion. The essence of this treatment is that a group of teeth is “excluded” from occlusion, initially 23 teeth, most often molars on the side that is not involved in chewing. This can be done by applying a mouthguard, and with the modern level of development of dentistry, it is much easier to apply bonding materials, preferably colored ones, so that they are more noticeable when they are ground off during the treatment process, as the deep bite is “opened”. Teeth excluded from occlusion “lengthen” and come into contact with antagonists, and teeth “released” from the aligner or after grinding off the composite, the teeth become separated and also “lengthen.”
Once a sufficient number of teeth are in contact and established at the new level, active treatment can be discontinued. This method is especially indicated for the elimination of anomalies associated with periodontal diseases, because it does not create additional load on the front teeth, as, for example, when using a bite block.
In permanent dentition, non-removable vestibular arch devices, including those with intermaxillary traction, are used to eliminate pronounced forms of anomaly. The system bracket can be used in combination with different types of bite blocks for the upper jaw. To accelerate the reorganization of bone tissue in the hypertrophied area of the alveolar process in the anterior region in adults, a complex method can be used: surgical (compactosteotomy) + orthodontic equipment.
When treating deep bites in adults, attention should be paid to issues of orthopedic treatment, that is, various types of prosthetics and combined, restructuring of the myostatic reflex (stretch reflex). The latter can be briefly explained as follows. In patients with a deep bite with central occlusion, the fibers of the masticatory muscles have a certain initial value, characteristic of excessive incisal overlap. When the bite is separated, for example, by a bite block, the fibers of the muscles that lift the mandible (mm. masseters, tstrongporales, pterygoidei medialis) are stretched, which increases their tone and causes the appearance of impulses in muscle receptors.
A reflex contraction of the levator muscles occurs, which through the periodontium creates tension in the area of the anterior teeth in contact with the bite pad. This constant tension increases during chewing and accelerates the restructuring of bone tissue. For retention after correcting a deep bite, you can use the same bite block as a retainer, but in an inactive state, that is, without separating the lateral teeth.
The goals and objectives of treatment of patients with secondary deep bite are determined by the reasons that caused this deformation (lack of teeth, systemic diseases of periodontitis, pathological abrasion). Treatment can be prosthetic or combined, and its choice is determined by the pathogenesis of secondary deep bite.
Concepts of occlusion in modern dentistry. History, terminology, clinical significance
This article is devoted to the history and development of the concepts of occlusion, as well as their clinical significance in dental practice. A critical assessment of occlusal theories requires an understanding of their development at the stage of formation and improvement of dental rehabilitation models. Despite significant interest in gnathology among leading members of the dental profession and the importance of occlusion to dental treatment, it was not until the 1970s that general recognition of the importance of occlusal aspects and the inclusion of occlusion in the training of dental students occurred. It should be noted that in our country (Russia) the study of gnathology remains the preserve of enthusiasts. At the same time, interest in gnathology and occlusion on the part of patients has increased significantly, which is facilitated by a general increase in public awareness. Despite the increasing demands of patients primarily for the aesthetic result of dental treatment, dentists must pay great attention to restoring the function of the masticatory apparatus. History and terminology First of all, it is necessary to define “gnathology”. This term was proposed in 1924 by the famous clinician and researcher of his time, Stallard. Mosby's Dental Dictionary defines gnathology as “the study of the functional and occlusal relationships of teeth.” The Glossary of Orthodontic Terms gives the following interpretation of this term: “Gnathology is a field of dentistry that studies the anatomical, histological, physiological and pathological aspects of the static and dynamic interaction of occlusion, the TMJ and the masticatory system as a whole, as well as issues of diagnosis and treatment violations in this system." Dentists have been thinking about solving the problem of fully restoring chewing function and articulation since the formation of the dental specialty in its modern sense. In the middle of the 19th century, Bonwill, based on numerous anthropometric studies, showed that the centers of both heads of the lower jaw form an isosceles triangle with an average length of legs of 10 cm between themselves and the contact point of the medial angles of the central lower incisors (Bonville triangle). Based on his measurements, Bonville designed in 1858 an articulator with horizontal condylar paths and an intercondylar distance of 10 cm. He did not limit himself to determining the static indicators of occlusion and strongly recommended studying its dynamic component, to denote which he introduced the term “articulation”. One of the first gnathological societies (California Gnathological Society) was created in 1926 by McCollum, who, together with Harlan, developed the first effective method of localizing the transverse (transversal) horizontal axis and transferring the registration impression to the articulator using the facial arcs of Snow. The Gnathological Society quickly expanded to 15 and then 24 members, who gathered together for meetings of a kind of discussion club. At these sessions, participants discussed the study and documentation of occlusion and eccentric movements of the mandible. It should be noted that this was one of the most responsible scientific approaches, and the club members continued their observations for more than ten years. However, even earlier, Dr. Gysi began using an articulator to model the occlusal surfaces of artificial teeth. His theory of facet-tubercle contacts was used in the manufacture of complete dentures and foreshadowed the concept of balanced occlusion, which prevailed in dentistry until the last third of the 20th century. In the 1890s. Technologies for replacing missing teeth with artificial ones have been developed, which required the formulation of certain concepts about the characteristics of teeth closure - occlusion. Dr. Edward Angle (1855–1930) published his articles on the classification of malocclusions, which placed great emphasis on the correct natural occlusion of the teeth. Engle classified the occlusal relationships of intact dentition and formulated the concept of ideal occlusion. In 1900–1901 In St. Louis, Dr. Engle and 12 of his colleagues founded a group studying the possibilities of tooth movement, which led to the formation of a new dental specialty - orthodontics. Subsequently, on the basis of this organization, the American Association of Orthodontists was created. Representatives of the American gnathological school adhered to the principle of balanced occlusion when restoring teeth, since they considered such an occlusal scheme to be the most natural. The ideological inspirer of this school was McCollum. In 1955, McCollum and Stewart published a “research report” in which they formulated the principles of mandibular movement, the transversal horizontal axis, the maxillary-mandibular relationship, and an arcon-type articulator designed to reproduce oral conditions. The purpose of using the articulator was to accurately simulate the relationship of the upper and lower jaws, including reproducing the border movements of the lower jaw and recording the parameters of the occlusal surfaces. Registration of horizontal and sagittal displacements of the lower jaw made it possible to determine the maximum height of the tubercles and the depth of the fossae, as well as the correct placement of ridges and fissures. More details on this concept can be found in the anatomical illustrations of McNorris and Schillingburg. Stewart denied the validity of the concept of balanced occlusion, since he noted uneven wear of the buccal and lingual cusps with the formation of deflective occlusal contacts, which led to changes in the pattern of jaw closure, while patients complained of loss of chewing efficiency and biting of the cheeks and tongue. The main gnathological concepts include: occlusion, centric relation, anterior guide, vertical occlusal distance, intercuspal position. In addition, the determinants of movements of the lower jaw, recorded using special equipment, are of great importance. From a practical point of view, gnathological concepts are most often used when performing fixed prosthetics. The basics of gnathology and occlusion are described in detail in the books “Principles of Occlusion” (Pokorny, Blake, Anaheim, Denar Corp, 1980) and “History of Gnathology” (Stuart, Golden, Ventura, Stuart Instruments, 1984). Currently, the most common concepts of occlusion are: • The concept of balanced occlusion • The concept of group function on the laterotrusive side • The concept of canine guide • The concept of myocentric occlusion • The concept of functionally generated path (Functionally Generated Path) according to Pankey, Mahan, Staehle. • Modified canine guide concept. The Pankey-Mann-Schuyler (PMS) theory for complete reconstruction of the occlusion assumed the creation of simultaneous contacts of the canines and lateral teeth on the laterotrusion (working) side during lateral movements of the lower jaw, and during protrusion movement only the anterior teeth are in contact. • The concept of sequential occlusion In gnathology, terms are used that require precise and correct interpretation. A clear understanding of the terminology allows the clinician to navigate and understand this multitude of concepts and choose the best one for a particular clinical case. Occlusion Many dentists understand occlusion as the simple closure of teeth. However, this interpretation of the term is very limited, since in fact occlusion refers to the relationship between teeth, masticatory muscles, TMJ and central nervous system within the framework of the functioning of the masticatory apparatus. Much confusion is caused by the existence of many definitions of the term “occlusion”, some of which are presented below. According to Wolfgang B. Freesmeyer, “occlusion is the contact static and dynamic relationship of the teeth.” Klineberg (Iven Klineberg) meant by occlusion “the dynamic biological interaction of the components of the masticatory system, which determines the relative position of the teeth.” The Glossary of Prosthodontic Terms gives the following interpretation: occlusion – 1) the process or fact of closure, overlap or exclusion; 2) a static relationship between the occlusal surfaces of the teeth of the lower and upper jaw. In the Dictionary of Orthodontic Terms, occlusion is understood as “the relationship between the teeth of the upper and lower jaw when they are closed in functional contact.” Mosby's Dictionary of Dental Terms gives the following interpretation of this term: “occlusion - 1) the process of closure or the result of the process of closure; 2) any contact between the cutting edges or chewing surfaces of the teeth of the upper and lower jaws. From a clinical point of view, occlusion is of great importance in all areas of dentistry. When restoring or changing the position of teeth, it is necessary to understand how teeth contact and relate in the frontal, sagittal and horizontal planes during various functional and parafunctional activities. The main goal of dental care is to achieve optimal functional and aesthetic results, including normalization of chewing function and the height of the lower third of the face. According to epidemiological studies, functional disorders of the masticatory apparatus occur in 60–80% of the population, while 15–20% of the entire population have complaints related to these disorders (McNeill, 1990). When the lower jaw moves forward, it makes a protrusive movement, or protrusion. Retrusion of the mandible means reverse movement. It is believed that there is a most posterior physiological relationship of the mandible to the maxilla into and out of which a person can make lateral movements of the mandible. This position is usually called the central ratio (CR). As is known, when the lower jaw moves, its head rotates around three axes. The CS is characterized by a certain spatial position of the heads of the lower jaw. The Dictionary of Orthopedic Terms gives the following interpretation: “central ratio is a relationship of the jaws in which the head of the lower jaw is in the most posterior, most superior and most internal position in the articular fossa.” Preston et al. (1999) define the centric relation as follows: “it is the relationship of the mandible (or jaws) in which the condyles occupy an anterior-superior position and contact the central part of the articular disc (a thin, avascular surface) located opposite the articular tubercle. This position is not determined by the contact of the teeth.” Dawson noted that disharmony between dental articulation and centric relation has a negative impact on all aspects of clinical dentistry. According to Rudolf Slavicek, in the interpretation of the term central ratio there is a certain dogmatism, which is expressed in confusion with formulations (there are more than 30), the promise of stability, non-acceptance of reality, and intolerance in discussions. Professor Slavicek proposed replacing the controversial term central relation with the term “initial position.” Reference position The reference position is a “controlled” unforced posterior position of the lower jaw, in which the TMJ tissues are not stressed (Slavichek). Anterior guidance Anterior guidance is a fundamental component of the gnathological concept of mutually protected articulation of Stewart and Stallard (or the so-called “circular protection”. According to this concept, contacts in the anterior teeth protect the posterior teeth during eccentric (excursive, non-working) movements of the lower jaw, and the chewing teeth protect the anterior teeth during working (chewing) movements of the lower jaw and when the teeth are closed in the maximum intercuspal position. At the same time, during movements of the lower jaw, no deflecting (displacing) occlusal contacts or obstacles should arise. Intercuspal contact ( IBC) is the contact between the cusps, pits and cutting edges of antagonist teeth. The intercuspal position, or intercuspal position (IBP), is a position of the jaws in which the teeth are in the IBC. The goal of adequate dental rehabilitation is the formation of unhindered occlusion and the corresponding concept of organic occlusion. Ideally, organic (organized) occlusion presupposes the presence of the following characteristics: - disocclusion (opening) during excursion movements of the lower jaw; - ratio of tubercle to fossa; — stable occlusion in the CS with a uniform distribution of occlusal contacts; — physiological distribution of occlusal load along the central axis of the tooth; — three-point occlusal contacts; — double central contact to ensure lateral stability of the tooth; — small area of occlusal contacts; - maximum cusp height and fissure depth with correct secondary anatomical features. Vertical distance of occlusion (vertical distance of occluson) The vertical distance of occlusion (VDO), or height of bite (VP), is the height of the lower third of the face when teeth contact in the MBP. This spatial relationship is most often measured when conducting phonetic tests, as well as when determining the interocclusal distance in the resting position (from the contact of the cutting edge of the lower jaw incisor to the lingual tubercle of the corresponding upper jaw incisor) and aesthetic parameters of the face and teeth. The incisal relationship determines the anterior landmark for the VRO. Resting position and VRO are among the most difficult parameters to evaluate, and the results obtained are extremely subjective. According to Desjardins, all methods for determining the resting position are to a certain extent unscientific, so the analysis of VPO should not be limited to any one technique (Desjardins RP. Clinical evaluation of the wax trial denturi. J Am Dent Assoc 1982; 104; 184 –90). Centric relation A gnathological term that has been widely used for many years in dentistry, particularly in dental prosthetics, to determine the reproducible position of the lower jaw. Despite the existence of several interpretations of the term CS (which causes considerable confusion), it is generally believed that the CS characterizes the relationship of the upper and lower jaws when the heads of the lower jaw are positioned in a physiologically stable position, independent of occlusal contacts. The CS is described as: 1. The relationship of the lower jaw to the upper, when the lower jaw is in the most posterior, relaxed position from which lateral movements can be performed, at any angle of opening of the jaws. This position is also called “ligamentous” because it is determined mainly by the TMJ ligaments. 2. The relationship of the upper and lower jaws, in which the heads of the lower jaw are in contact with the thinnest non-vascularized portion of the corresponding disc, when the disc and head complex is located in the most anterior and superior position relative to the slope of the articular eminence. 3. The maximum anterior position of the heads of the lower jaw in the articular fossa with the correct position of the articular discs. In the presence of dysfunction of the masticatory system, it is sometimes impossible to determine the true central relationship of the jaws. Central occlusion, or maximum intercuspal position, or habitual occlusion (centric occlusion, intercuspal position, habitual occlusion) The position of the lower jaw, which is determined by the maximum (habitual) intercuspal contacts of the teeth of the upper and lower jaws. This position depends on occlusal contacts and does not depend on the position of the heads of the lower jaw. Functional or physiological occlusion (functional occlusion, physiological occlusion) A static or dynamic occlusal relationship that ensures minimal load on the TMJ, optimal functioning of the orofacial complex, stability and aesthetics of the dentition, as well as protection and healthy periodontal health. Overlap, or vertical overlap (overbite, vertical overbite) The degree of overlap of the lower jaw incisors with the upper incisors. Usually measured perpendicular to the occlusal plane in millimeters or as a percentage of the total height of the lower incisor crowns. Traumatic vertical overlap (impinging overbite) Extremely pronounced vertical overlap when the lower incisors come into contact with the mucous membrane of the palate behind the upper incisors. This condition often occurs in patients with severe class II occlusion of the 2nd subclass. Negative (reverse) vertical overlap, or open bite (Negative Overbite, Open Bite) congenital or acquired anomaly of the occlusion characterized by the absence of vertical overlap of the front teeth of the upper and lower jaws (anterior open bite) or the absence of occlusion in the field of chewing teeth (side open bite bite ). Local open bite, i.e. Including a small number of teeth, can develop as a result of fingers or the influence of other local factors (dental open bite), and can also be caused by the divergence of skeletal planes (skeletal open bite, or aperturenatia). Positive overlap (Positive Overbite), characterizing the fact of the presence of vertical overlapping of the lower incisors of the upper. Positive blocking is inherent in both ideal occlusion and a pronounced abnormal deep overlap. Sagittal overlap (Overjet, Sagittal Overbite) The distance between the vestibular surface of the lower incisors and the palatine part of the cutting edge of the upper ones is usually measured in parallel to the occlusal plane. In most cases, in the absence of an indication of another, this parameter is determined in the area of the most strongly protruding central incisors. The severity of sagittal overlap mainly depends on the vestibular-speaking position and inclination of the upper and lower central incisors. Only in a small number of cases, this indicator directly affects the front-and-item skeletal ratio. Bucket sagittal overlap (Buccal Overjet) the distance between the buccal surfaces of the upper chewing teeth and their antagonists. This "unofficial" term determines the tendency to cross bite in the lateral teeth. Negative, or reverse, sagittal overlap (Negative Overjet, Reverse Overjet) is usually associated with anomaly of class III occlusion, in which the upper incisors are closed lingually relative to the lower incisors. Positive sagittal overlap (Positive Overjet) a term denoting the closing of the upper incisors more pagan than the lower anomaly of class I or II class II. The medotype (non -working) side contact of the teeth occurs when the lower jaw is displaced to the right or left on the opposite side, while the medotype side moves to the middle line. Laterotruse (working) side contact occurs when the lower jaw is displaced to the right or left, on the side of the displacement. The movement of Bennett (latterotrosis) is the movement of the head of the lower jaw on the working side laterally and up during the side movement of the lower jaw. The angle of Bennett is formed by the horizontal axis of the head of the lower jaw and the sagittal plane on the medotorus (non -working) side when the head of the lower jaw moves down and medially. Features of the main occlusal schemes are a non -monatological (1964) ratio of occlusion to the CS and MBP Occramlia to the CS coincides with the MBP and is characterized by the presence of three -point contacts of the contacts during excursion movements of the lower jaw, the fang guide during lateral movements, the opening of the chewing teeth in any excursion movements. Circular protection of occlusal contacts is provided. Comments Adequate scheme in the absence of a pronounced horizontal component when slipping from the OTC to MBP. Strict followers of this concept insist on using a fully adjustable articulator and other devices necessary to achieve the required result. -Clousing scheme for iodide (YouDelis, 1977) The ratio of occlusion to the CS and MBP Occramlisia in the CS coincides with the MBP and is characterized by the presence of three -point contacts of the contacts during excursion movements of the lower jaw as well as in a mental scheme, but are programmed in such a way that during abrasion or displacement of fangs There was a group function. Comments useful option if it is impossible to control the parafunctional excursion movements of the lower jaw or in the non -optimal state of fangs. -Clousing diagram on the punk -Mannu -Shuler (Panky -Mann -Schuyler, 1963) The ratio of occlusion to the CS and MBP Freedom Zone between Occlusia in the CS and MBP (<0.5 mm). Functionally determined form of occlusal surfaces. Contacts with excursion movements of the lower jaw of the front guide is finally simulated using temporary restorations. Either a fang guide or a group function. Comments high risk of error when using the methodology of a functionally determined path that determines the shape of the occlusal surfaces of chewing teeth. -Wear in central occlusion (1982) the ratio of occlusion in the CS and MBP Freedom Zone between Occlusion to the CS and MBP (0.5 mm ± 0.3 mm); Fissure-tubercle contacts. Contacts with excursion movements of the lower jaw Fang guide or group function. The front guide is involved with a slight delay due to freedom in central occlusion. Comments useful option for a pronounced horizontal component of slipping from the OTC to the MBP before treatment. The freedom zone must be carefully checked. -Balanced occlusion (1960) The ratio of occlusion in the CS and the MBP zone of freedom between occlusia in the CS and MBP. Contacts with excursion movements of the lower jaw balanced workers and non -working contacts during lateral movements. Balanced contacts in the area of the anterior and chewing teeth during occlusal movements. Comments ensure the stability of removable full prostheses with excursion movements of the lower jaw, but it is difficult to achieve in the presence of natural teeth due to high risk of excessive load on the non-working side. -Sema along Naiman and Lind (Nyman and Lindhe, 1983) the ratio of occlusion to the CS and MBP uniform occlusal contacts in the CS and MBP (0.5 mm ± 0.3 mm). Contacts during excursion movements of the lower jaw bilateral balanced contacts during excursion movements are first verified using provisive (long -term) restorations and subsequently reproduced at the final restorations. Comments are used in creating bridge prostheses located on both sides of the jaw, in the presence of periodontitis of a severe degree, but subject to stabilization of the state! Balancing contacts allow for the stability of bridge prostheses fixed to mobile supports.
“All-round occlusal protection” means that in the MBP, the posterior teeth take on the maximum occlusal load, while the anterior teeth are out of contact (with minimal clearance). During excursion movements of the lower jaw, the anterior teeth provide anterior guidance, leading to the opening of the chewing teeth, which avoids lateral loading on them. To avoid blocking the heads of the mandible in the CS, the anterior guide should start relatively shallow with a gradual increase in steepness. The “zone of freedom” (“freedom in central occlusion”) is designed to prevent blocking of the heads of the mandible in the CS.
Source: https://forumstom-kz.com/