48646
Crooked, unhealthy teeth can ruin the appearance of an otherwise attractive person. Oral health is important not only for our attractiveness, because the main function of teeth is to grind food. The condition of the stomach and intestines depends on this, which directly affects health and life expectancy .
Stages of bite formation in children
The process of developing a child’s bite can be divided into several important stages.
Each of them is characterized by changes in the structure of the jaw and has factors that influence the formation of pathology. Stages of bite development in children:
- Elementary.
From birth to six months of the child. The first teeth begin to erupt towards the end of the period. The cause of pathology at this stage is a genetic predisposition or improper latching of the nipple during breastfeeding. - The process of formation of the bite of primary teeth.
Lasts until the age of three; as a rule, by the end of the period, all 20 baby teeth are in their position. At this age, the presence of gaps between the teeth is acceptable, but twisting, too close a fit, and growth in an uncharacteristic plane are considered as deviations from the norm. In addition to the above reasons, the most common factor in the development of pathology is bad habits: thumb sucking, pacifiers, toys or eating disorders. The child's diet should include a sufficient amount of solid food. - Preparation for the development of permanent dentition.
The stage continues until the appearance of the first permanent teeth. With proper oral care, no external changes are observed during this period. Bad habits can cause malocclusion. It is necessary to ensure that the child does not chew hard objects: pencils, thick books, furniture, since baby teeth are very soft and easily deformed. - Changing the temporary bite to a permanent one.
The most critical stage. It is during this period that serious pathologies begin to manifest themselves as unpleasant changes: torsion, improper growth of teeth, discrepancy between the size of the jaw and the volume of bone units, etc. On average, this period lasts up to 12 years. Factors in the development of anomalies are physiological characteristics or untimely replacement of teeth. - Formation of a permanent bite.
The teeth complete their growth and occupy a certain position in the jaw.
You can start correcting your bite from the early stages. There are several hardware and manual methods for this. Treatment with braces begins after a permanent bite has formed.
Signs of malocclusion
For timely detection of maxillofacial defects, it is necessary to regularly examine the baby’s oral cavity. Here are a few signs by which you can identify a malocclusion in a child:
- obvious displacement of the lower jaw outward or inward;
- crooked, uneven teeth;
- vestibular or lingual growth of teeth - in front or behind the main row;
- diastema - spaces between the incisors;
- strong overlap of the lower teeth with the upper ones;
- non-closure of the upper and lower incisors with a formed bite;
- half-open mouth, replacement of nasal breathing;
- speech defects.
Signs of malocclusion
In addition to the visible signs, if you look closely, you can notice abrasion of the enamel on the front or back teeth, and gum injuries. The child complains of tension in the jaw muscles, difficulty chewing or swallowing food, and headache. These signs will help you understand that your child has a malocclusion and seek advice from an orthodontist.
Diagnostics
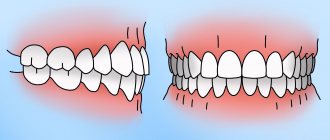
It is not difficult to determine the narrowing of the jaw in a child or adult during an external examination. Its clear sign is the “pressed-in” dentition in certain areas or along the entire length with partially expanded, crowded units. Another characteristic feature is malocclusion.
At the same time, it is necessary to distinguish pathologies of jaw development from atypical orthodontic and dental situations such as supernumerary units, macrodentia, individual structural features of the skull, etc. They can also be combined. Therefore, a preliminary diagnosis made visually is confirmed with the help of one or more additional studies:
- According to Pon-Linder-Hunt , where the difference between the normal and existing width of the dental arch for a given patient is calculated using a special formula. The method requires taking several measurements directly in the oral cavity and taking into account different indicators for representatives of individual nations. But it gives the attending physician a fairly accurate answer to the question of whether several units will have to be removed to level the entire row.
- According to Howell-Gerber-Gerbst - another relatively complex mathematical scheme that is well suited for measuring the shape, length, width and other individual parameters of a row.
- Teleradiography is a type of X-ray examination that allows you to take a picture of the entire skull. It gives a detailed picture of the deviation itself and reveals its causes, if they are embedded in the structure of other bones.
- Anthropometry is an accurate three-dimensional cast, on which it is easier to take the necessary measurements, especially when the upper or lower jaw of a child is narrowed.
- X-ray - used to assess the condition of the upper palate and its suture, bone structure.
- Orthopantomography - a classic frontal image, is now increasingly being replaced by CT (computed tomography) due to its improved clarity and expanded capabilities - such as obtaining 3D images.
In combination, these methods allow the orthodontist to study the current condition of the bone, the degree and direction of deformation when narrowing the upper and/or lower jaw.
When choosing a correction method, it is also important that they provide an opportunity to evaluate the resource for moving teeth into the correct position and straightening the bite.
Types of malocclusion
The curvature of the teeth does not always mean a pathology of the bite, which is understood as the closing of the jaws, ensuring the full, unhindered functioning of the masticatory apparatus.
Among the types of malocclusion in children are:
- Prognathia – distal occlusion.
This is a common reason for visiting an orthodontist in early childhood. The muscles of the lower jaw are not yet sufficiently developed, so outwardly it seems that the upper row of teeth protrudes strongly forward compared to the lower one. With the introduction of hard foods into the diet: hard fruits and vegetables, the problem may disappear without medical intervention. - Progenia – mesial occlusion.
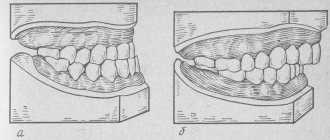
At an early age, this pathology is usually caused by genetic characteristics or improper latching of the nipple during feeding. The sooner the pathology is identified and treatment is prescribed, the fewer negative consequences the child will receive. - Deep bite.
Parents often confuse it with the distal one, however, with a deep bite, the lower jaw does not go back, but seems to sink inside. The upper front incisors overlap the lower ones by more than half. Obvious signs of pathology are speech defects and soft tissue injuries. - Crossbite.
It appears at the stage of replacement of milk teeth with molars. In this case, on the one hand, the upper jaw overlaps the lower jaw, on the other, the lower teeth come to the fore. - Open bite.
With this malocclusion pathology, there is a noticeable lack of closure between the teeth of the upper and lower rows. Most often, this disorder affects the incisors, but it also occurs on the posterior premolars and molars.
Types of Malocclusions
Malocclusions in children are diagnosed during annual examinations. It is important not to waste time and immediately begin preventive or therapeutic treatment.
Treatment options in adults
For patients over 18 years of age or with complex curvatures, more or less extensive surgical solutions are recommended. The simplest methods of treating narrowing of the upper jaw in adults:
- Installation of the Derichsweiler apparatus - a beam screw design for the upper jaw only. He breaks the palatal suture and sets its bones in a new, wider position. Then the teeth are straightened with braces.
- Normalization of the bite by removing several units in a row (in the vast majority of cases, the first premolars, 1 on each side). The method allows you to correct the bite and aesthetics of the smile without treating the narrowing of the jaw itself, if it is impossible or not necessary. Extracted premolars are not always redundant. But due to them, space is freed up for the remaining ones, and their location is again leveled with the help of braces.
In the case of the lower jaw, the layer of gum tissue is lifted, the bone is drilled in several places and the holes are connected with grooves. An expander is installed in them, with which the patient with a narrowing will need to go through several years, and the mucous membrane is returned to its previous position. This procedure is called jaw perforation.
Photos of children with pathological bite
In the presented images you can see the child’s malocclusion. The photo shows various pathologies that are often found in patients with baby or molar teeth. Detailed photographs of children with malocclusion captured in the photo during an orthodontic consultation will help parents in self-diagnosis of the pathology. However, the doctor chooses the effective therapy regimen.
Photo of a girl with an incorrect open bite
Photo of a child with an incorrect deep bite
Photo of a boy with an incorrect deep distal bite
The boy has an open bite
The girl has a deep distal bite
How to correct a child's bite
No matter how severe the pathology, the earlier treatment is started, the easier it is to achieve an effective result. To correct violations, there are three ways to correct bite in children:
- traditional – installation of braces;
- alternative (without braces) – mouth guards, plates, physiotherapy;
- cardinal – surgical intervention.
Until the final stage of permanent bite formation, only alternative methods are used, but is it possible to correct a child’s malocclusion with their help?
Removable orthodontic plates
Orthodontic plates
are structures consisting of a polymer jaw-expanding base and metal arches that serve to fix the plate and align the front row of teeth.
Removable orthodontic plate
These devices are made individually, based on casts of the jaw of a small patient. To adjust the load, the devices are equipped with screws and expanders. At an appointment with a doctor, the child’s parents will learn how to perform this procedure on their own, which will save time on visits to the orthodontist.
Plates for correcting malocclusion in children are designed to be worn constantly, but the removable structures are removed during meals or hygiene procedures.
Trainers for teeth
Trainers
To correct malocclusion in children, they are mouth guards made of dense silicone.
Trainer for correcting the bite
The trainer performs several functions:
- Self-corrects minor pathologies.
- Prevents further development of malocclusion and prevents complications.
- Helps get rid of bad habits that have caused crooked teeth.
Mouth guards for correcting malocclusion in children fix both jaws simultaneously in the correct position. But when using them, it is impossible to lead a normal lifestyle: talking, eating. Therefore, mouthguards are worn while the child is sleeping and for several hours during the day.
The process of correcting a bite with trainers is long and requires patience from the child and parents.
It has been noticed that in children who regularly use trainers before installing braces, the effect of therapy occurs faster.
Myotherapy
Myogymnastics
in orthodontics, it is a set of exercises to relax or develop individual facial muscles.
Myotherapy in orthodontics
The method serves as both a primary and an auxiliary method of occlusion correction. For each type of pathology there is its own set of exercises. The first lessons are carried out under the supervision of an orthodontist; as soon as the child learns to do gymnastics correctly, he continues to work at home independently or with his parents.
Conditions for performing exercises to correct bite in children:
- Systematicity and regularity.
- Sufficient application of force without jerking or pressure. The muscles feel resistance, but are not overloaded.
- Cyclicality. Exercises are performed in several approaches to achieve good results.
- Gradual increase in load and intensity.
Myotherapy is especially effective in correcting occlusion in combination with physiotherapy: electrophoresis, vibration massage, ultrasound, vacuum therapy, massage.
Alternative methods can correct mild pathologies of malocclusion in early childhood or slow down the development of complications and wait until the formation of the jaw is completed to begin basic treatment.
Braces
Braces
– the main way to correct uneven teeth and malocclusion in children from 12–16 years old and adults of any age.
Braces for correcting bite
They are a system of clasps fixed on the outer or inner surface of the teeth and a steel arch stretched between them.
Under the pressure of the arch, the teeth are aligned and placed in the correct position. With the help of braces, it is possible to correct almost all malocclusion pathologies. Treatment takes from 6 to 18 months and ends with the acquisition of a beautiful, even smile.
Varieties
This disease has several variants.
- Narrowing of the dentition along the entire length. Its typical sign is the appearance of a “horse” smile due to the fan-shaped incisors.
- Trapezoidal deformity. With it, the patient's jaw takes on the shape of a trapezoid with clearly visible visually defined angles in the area of growth of the 3rd incisor or 1st premolar.
- Narrowing in the anterior region. Here the incisors converge like a wedge and “climb” onto each other.
- Saddle defect. With it, the row is “dented” inward at the level of the premolars (4 and 5 units on each side) with 6 and/or 7 molars. And the incisors and “eights” are usually positioned correctly, or they may be moderately crowded and rotated.
- Asymmetry. This depression is observed only on one side, but, as a rule, affects both jaws. Often combined with normal occlusion in other areas.
All of them can be I, II or III degrees of severity. The pathology first appears in childhood, as temporary teeth are replaced with permanent ones. In adolescence and adulthood, consolidation of malocclusion leads to a change in the load on the mandibular joint, spreading secondary deformations to healthy areas.
The narrowing of the upper jaw is also accompanied by a deepening of the palatine vault and makes nasal breathing difficult. Plus, these processes provoke uneven wear of crowns and can lead to underdevelopment of units that do not have enough space.
Treatment of malocclusion in children of different ages
Anomalies in jaw development and tooth growth cannot be ignored. Early childhood is not a reason to refuse correction. The orthodontist will help you choose the most effective treatment method. The use of alternative therapy methods can completely restore jaw function or prevent the occurrence of health-threatening complications.
Let's look at how malocclusion is treated in children of different ages.
Children under one year old
At this age, parents' actions should be aimed at preventing the development of jaw pathologies. Effective measures include:
- maintaining the correct position of the head during feeding, it does not tilt back, the chin is not pressed against the baby’s chest, make sure that the nipple is grasped correctly;
- the use of orthodontic pacifiers that imitate the female nipple and promote the correct position of the jaws when sucking;
- preventing the development of bad habits;
- introduction of solid food into the diet with the appearance of the first teeth;
- adequate consumption by mother and child of foods containing fluoride and calcium or vitamin supplements designed specifically for nursing women;
- preventive examination at the dentist.
Most often, malocclusion in a child of the first year of life develops due to the use of a low-quality pacifier, so the choice of this accessory is very important.
Children from 1 to 2 years old
There are often questions from worried parents on the Internet: “My child is one year old, it seems that he has the wrong bite, what should I do?” First of all, if you suspect the development of pathology, you need to show the baby to a specialist. He will determine whether the feature is an age-related norm or a complication.
Malocclusion in a 1-year-old child occurs as a result of dysfunction of sucking (and then chewing). At such an early age, hardware correction methods are not yet available, so physiotherapy and the use of orthodontic pacifiers, which return the jaw to its normal position, are most often prescribed.
To correct malocclusion in a child 2 years of age and older, Hintz plates are used, which are similar in shape to a pacifier, but instead of a pacifier, a flap is placed in the mouth and clamped between the teeth. The longer the device is used, the faster the bite is corrected and bad habits are eliminated.
Children from 3 to 5 years old
Malocclusion in a 3-year-old child is corrected with special caps for correcting the position of the jaw, which are worn at night. You can also continue therapy using Hintz plates.
Another accessible method at this age is myogymnastics. A three-year-old child can easily cope with the exercises.
From 4 years of age it is allowed to use LM activators under the supervision of an orthodontist. And malocclusion in a 5-year-old child is corrected with the help of trainers and orthodontic plates.
The first thing to do when malocclusion is detected is to show the child to a qualified orthodontist.
Children from 6 to 14 years old
Malocclusion in a 6-year-old child should cause the greatest concern for parents, since when baby teeth are replaced, this pathology will certainly affect the growth of permanent bone units.
Therefore, careful adherence to the dentist's recommendations is necessary. At this age, all alternative methods are available; the doctor will select the most effective one.
Causes of malocclusion
Many factors influence jaw development. Among the main reasons for the formation of malocclusion in children are:
- heredity;
- incorrect position during breastfeeding, incorrect grip of the nipple or bottle nipple;
- bad habits;
- physiological features, for example, a narrow jaw;
- late transition to solid food;
- ENT diseases;
- metabolic disorders, lack of microelements;
- incorrect posture;
- intrauterine developmental pathologies;
- early loss of baby teeth or delayed loss of teeth;
- accompanying illnesses.
The habit of thumb sucking can cause malocclusion.
Before starting treatment, you need to make sure that the factor that caused the pathology no longer has an effect.
Correcting a child’s malocclusion without eliminating the cause is ineffective.
Reasons for formation
The development of the jaw in children occurs under the influence of the tongue, its chewing and facial muscles. When some pathology appears in the activity of these muscles, a modification of all parameters of the arches occurs.
Prerequisites for jaw reduction:
- If baby teeth have fallen out or been removed.
- The chewing load decreases and free space appears in the rows, which causes deterioration in the functioning of the jaw.
- Parents started feeding their child solid food late.
- Jaw growth occurs due to a decrease in chewing severity.
- Metabolic imbalance affecting osteogenesis.
- When children acquire the habit of sucking their cheeks, tongue, etc., this causes an imbalance in muscle activity.
- Mouth breathing.
- An extremely serious aspect that leads to countless failures.
- Pathologies leading to transformation of the dentofacial apparatus, resulting in problems with speech, swallowing, and breathing.
- Genes.
Diagnostic methods
The disorder is characterized by symptoms that make diagnosis difficult, but an experienced specialist often, after one medical examination, decisively declares problems and makes a diagnosis. But additional research may be required.
- Radiography. An x-ray of the palate, which determines the condition of the palatal suture, is extremely significant.
- In addition, teleradiography and orthopantomography are often performed.
2.1. X-ray is a frontal photograph of the jaws and face, which allows you to examine the interaction of a number of teeth in the desired direction.
2.2. An orthopantomograph shows the entire area, using a camera that moves around the circumference of the head.
- Anthropometry of the dentofacial apparatus. A cast of the jaw, constructed from a special plaster, is studied in 3 mutually perpendicular projections.
- Pon's method. The essence of the method is that the total width of the teeth in the mesiodistal direction is measured, and the usual row width in the area of the initial incisors is taken from the tables. By comparing the actual value with the reference value, the jaw contraction is calculated.
- Howley-Herbst diagram Howley-Herbst method. Consists in building the jaw arch. Applying this criterion, a curved line (ellipse or parabola) is constructed, the shape of which is specific, having the shape of an exemplary arc for a particular client
Indications for expansion
This procedure applies in the following situations:
- When the upper row of the jaw narrows.
- The aesthetic attractiveness of the face is impaired.
- Incorrect condition of specific teeth.
- Pathology of occlusion.
- Pathology of nasal breathing.
- If soft tissues are damaged.
- If the periodontium becomes inflamed.
- The functionality of chewing and swallowing is impaired due to jaw contraction.
- Hereditary defects.
- Lack of space in a row.
Devices
Their effects are mechanical. Slow displacement allows you to increase the arc due to the alveolar deflection of the incisors, without breaking the palatal suture.
If a larger increase is required, in this case it is performed by opening the palatal suture.
The expansion technology is carried out using a Derichsweiler apparatus with a Hyrex screw.
- Derichsweiler apparatus
It is compact - a non-removable configuration, consisting of a metal frame with a screw, and bushings fixed on the chewing elements. It is used to expand the HF along the entire length. When the screw is turned, the frame increases. Its action is based on the rupture of the palatal suture. Thus, the size of the nasopharynx increases and breathing is stabilized. The device is used when conventional methods no longer help, and there is a question about the operational impact. Often it gives the opportunity to cancel the operation
- Expansion plates
Design-expanding mechanisms: screw, spring three-wire arc. They are considered a gentle type, correcting an anomaly in a rapid or premature hybrid occlusion. The expanding plate fits closely to the palate, repeating its configuration. It is combined with the main components with clasps, which can be removed at any time. Plates are used for minor deviations.
- Surgical intervention
The procedure is used in the most difficult cases, if completely orthodontic and myofunctional therapy is ineffective.
Used in an ensemble with orthodontic correction.
Orthodontic surgical therapy is a three-stage procedure.
First is carried out:
- preoperative preparation for surgery;
- surgical intervention;
- orthodontic correction is completed.
The most important operations:
- Elimination of the tooth for unobstructed access during surgery.
- Perforation of the jaw bone.
It is carried out with the detachment of part of the mucous membrane. Holes are made in the jaw and connected by grooves. The wounds are then sutured and an expansion device is installed.
Result
| Click to sign up for a FREE consultation |
In small children, the expansion of the jaws in most cases proceeds rapidly (sometimes after a few months it also comes to an end). And it still ends well. The outcome of treatment with orthodontic appliances for older people is by no means so predictable (it can last for years).
A long period of treatment for narrowing of teeth can be avoided by taking preventive measures:
- The main thing is the current treatment of enterobacterial and viral infections of the nasopharynx, in order to normalize breathing.
- It is also necessary to wean children from those habits that can disrupt the formation of jaw bones. For example, finger sucking, which is quite common in children.
- The position of the baby during sleep sometimes also affects the formation of the jaws (when his head rests on his chest).
- Children's nutrition simply must be in accordance with their age. Being late in switching to solid food can disrupt the formation of the jaws due to underdeveloped muscle functionality. Also, in the baby’s food, parents should include all the elements necessary for the formation of the body.
Note! Regular preventative visits to the dentist will help identify narrowing of the jaw as soon as possible. And also, together, the father and mother are obliged to carefully monitor the formation of the dentofacial apparatus of their children. As a result of identifying deviations, it is necessary to immediately take the child to the dentist.
Consequences
What complications can arise if a child’s malocclusion is not corrected? Possible consequences:
- tooth abrasion, premature wear, increased risk of caries;
- difficulty chewing causes gastrointestinal problems;
- mucosal injuries, gum inflammation, periodontal disease;
- increased load on the temporomandibular joint, pain, inflammation;
- breathing problems, ENT diseases;
- pinched nerves in the cervical spine;
- aesthetic facial defects, asymmetry;
- psychological problems;
- violation of diction.
Thus, malocclusion in children is dangerous for the development of diseases. It directly affects the emotional state of the individual, self-esteem, and self-confidence. If the bite is not corrected in time, physiological, psychological and aesthetic problems may develop.
Bilateral and unilateral narrowing
Reducing the width and increasing the depth of the palate, closure disorders are a complication. According to statistics, the upper jaw is more susceptible to pathology. This flaw leads to complications in organs related to teeth:
- The cause of deterioration in breathing occurs due to a decrease in the volume of the nasal cavity.
- Due to the small space, diction deteriorates, as the tongue becomes inactive.
- Food begins to be chewed worse - loose teeth cause problems with digestion.
Prevention
Prevention of the development of malocclusion in children begins at an early age. By following simple recommendations, you can avoid problems and maintain your baby’s beautiful smile.
Dentists' advice:
- Correct attachment to the breast or bottle. Usually a new mother will be helped with this by a pediatric nurse or a breastfeeding specialist.
- Prevent the development of bad habits, gradually abandon the pacifier when the first teeth appear.
- Supplement your diet with solid food in a timely manner.
- Keep your mouth clean.
- Perform gymnastics to develop facial muscles.
The effectiveness of preventive measures can be monitored by a local dentist, whose consultation is recommended for children at least once a year.
The health of a child’s teeth affects not only the appearance, but also the functioning of the entire body. Incorrect bite is the cause of serious illnesses. Therefore, it is important to identify pathologies in time and correct them using methods available for a given age.
Diagnosis and treatment of narrow jaw
Deformed dentition, crowded teeth, malocclusion, unerupted teeth are consequences of an underdeveloped dental system. The earlier these abnormalities are diagnosed, the more effective the treatment will be. To expand the lower and upper jaws, therapeutic methods, mechanical expanders and plates are used. In rare cases, only surgery helps.
In children under 10-11 years old, jaw expansion gives the best results. This is a time of active growth and formation of bone tissue, so the defect can be corrected with the help of orthodontic structures.