Pathological occlusion is a violation of the relative position of the dentition, observed when the upper and lower jaws are completely closed. Today, most people have a different bite than normal. However, as a rule, such violations are not critical and do not require correction.
In turn, serious anomalies in the structure of the bite can lead to disruption of the functions of the dentofacial apparatus, other organs and systems of the body, and cause morphological and aesthetic disruptions. Such violations require timely detection and correction using modern orthodontic structures and devices.
Types of pathological bite
Modern orthodontics identifies five key forms of pathological occlusion:
- mesial (mandibular bone protrudes significantly forward);
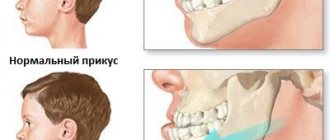
- distal (the front part of the upper row of teeth protrudes significantly forward);
- deep (mandibular incisors are overlapped by upper incisors by more than ½ length);
- open (in this case, part of the teeth on both jaws cannot close, forming a gap);
- cross (one or both sides of one of the jaws are underdeveloped).
Some researchers include in this classification such disorders as diastema and dystopia. Dystopia is a pathology of occlusion in which individual teeth are located outside their standard position in the dentition. In turn, the term diastema refers to such a violation of the position of the teeth, in which a gap is formed between adjacent central incisors, having a width of up to 6 mm.
Prevention
Malocclusions are various types of deviations from the normal arrangement of the dentition relative to each other. Such deviations can appear both in adults (for example, after the eruption of wisdom teeth or as a result of injury), and in children during the period of growth and formation of the dental system.
The severity of an abnormal bite can vary significantly - depending on the severity of the pathology, grades I, II and III are distinguished. However, even fairly minor malocclusions sometimes create very serious problems for a person’s normal life, ranging from psycho-emotional ones to problems with eating.
What are malocclusions?
Orthodontists use Engle's classification in their practice. He identified 3 types of bite, depending on how the first molars (that is, the so-called molars) close together.
The first class according to Engle is considered the norm of occlusion, a kind of standard that the orthodontist tries to achieve if there are any deviations from the normal relationship of the teeth. It was revealed that it is the closure of teeth according to the first Angle class that is the most physiological for the entire human dental system.
Today, orthodontists classify occlusion deviations in the lateral part of the teeth as sagittal anomalies, and deviations in the anterior part of the dentition as vertical malocclusions.
Malocclusions also include such pathologies when, with normal closure of the teeth, the following defects are present in the lateral region:
The median diastema is the gap between the first incisors of the upper jaw. In the early mixed dentition (from 2.5 to 4.5 years), diastema is a normal physiological condition when the frenulum of the upper lip passes between the temporary central incisors. During normal development, during the eruption of the lateral incisors and canines, this gap closes, and the attachment of the frenulum is displaced and woven into the mucous membrane of the upper lip. In some cases, the cause of a diastema may be the presence of a supernumerary tooth in the area of divergence of the central teeth of the upper jaw (this pathology can be identified by the results of an x-ray examination).
Teeth crowding – this malocclusion occurs when the size of the teeth and dental arches do not match. Approximately 60% of European children have some degree of dental crowding. In this situation, the loss of a permanent or temporary tooth can cause adjacent teeth to move into the area of the defect to fill the void. Crowding of the lower teeth during adolescence is mainly due to the eruption of wisdom teeth and the pressure they place on the dentition.
Trema – spaces between teeth. It is important to understand that in a mixed dentition, the presence of three is a normal phenomenon, caused by the fact that the baby teeth move apart and prepare space for the permanent larger teeth. Tremas can appear with microdentia - small sizes of the teeth themselves. In any case, the child’s parents should pay attention to such spaces between the teeth, as food gets clogged in them, which, if hygiene is poor, can lead to caries and gum inflammation.
Transposition or dystopia of teeth - these similar terms refer to the eruption of a tooth in an unusual place for it. There are several reasons for this phenomenon. For example, this may be an abnormal position of the tooth germ due to a hereditary factor, pathologies of the fetus during pregnancy, illness of the mother in the first stages of pregnancy, birth trauma of the child, the use of forceps during obstetrics, etc. The cause of dental dystopia may be another - lack of space in the dentition causes them to erupt outside the dental arch: in the cheeks, in the lips, causing injury to the child when chewing and forming a source of inflammation, because sometimes it is quite difficult to reach such a tooth when brushing.
Let's take a closer look at the following malocclusions.
Distal bite.
Distal occlusion is the most common malocclusion pathology among the European population. Many people associate its occurrence with the nature of the food we eat - we began to eat more soft food, and therefore the need for chewing and effort disappears. The lower jaw decreases in size, no longer moves forward as much, and the upper jaw prevails over the lower jaw. Distal occlusion is a class II anomaly according to Engle's classification.
In the distal bite, two subclasses are distinguished depending on the inclination of the maxillary incisors.
Class II, subclass I - the upper incisors are inclined towards the upper lip. The reasons for the formation of this phenomenon may be the habit of thumb sucking, prolonged sucking of the pacifier, the habit of placing the tongue between the teeth, as well as hyperactivity of the muscles of the upper lip and the orbicularis oris muscle.
Facial signs of this type of occlusion are a concave profile, unclosed lips, and compensatory pulling of the lower lip forward and upward. Sometimes there are cases of excessive activity of the lower lip (for example, with the habit of biting the lower lip), then the upper incisors move forward, and the lower ones fall back from the normal position.
Class II, subclass II - the upper incisors are inclined towards the palate. A provoking factor may be the habit of biting the upper lip, as well as the infantile, that is, childish type of swallowing with tension in the muscles of the lips and cheeks. In such cases, when examining the patient, the lips are closed, the lower lip is thickened, and a deep fold is visible on the chin.
Distal occlusion is often accompanied by speech disorder, inability or difficulty biting food, difficulty breathing, as well as pain and dysfunction in the temporomandibular joint.
Mesial bite
Compared to the distal bite, with the mesial bite the opposite situation is observed - when the upper jaw lags behind the lower jaw in size. This is the third class of malocclusion according to Angle's classification.
The reasons for the development of mesial occlusion may be:
- birth injury;
- early removal of upper teeth;
- genetic predisposition - for example, the child inherited a massive lower jaw from his father and a small upper jaw from his mother.
Often, with this anomaly of occlusion, one can see a phenomenon called dentogingival compensation: the teeth on the upper jaw are crowded, while on the large, forward lower jaw they are located evenly, there may be gaps between them (three).
Facial signs of mesial occlusion: a convex profile, a noticeably protruding chin, recession of the upper lip and protrusion of the lower lip.
Mesial occlusion contributes to the development of disorders of the temporomandibular joint - due to the anterior position of the head of the upper jaw in the articular fossa, there is a constant stretching of the TMJ ligaments, tension in the temporal and masticatory muscles, and possible development of pain when eating, as well as headaches. Sometimes patients complain of injury to the upper lip by the teeth of the lower jaw while eating.
Open bite.
An open bite is a non-occlusion of the teeth in the anterior region, which causes a gap to form between them. Normally, the upper incisors should overlap the lower incisors by one third of the crown size. With an open bite, there is no overlap at all or minimal.
The following types of open bite are distinguished:
- anterior open bite – there is no overlap in the anterior part of the dentition with the lateral teeth closed;
- lateral open bite - when the teeth in the anterior part overlap, the lateral teeth do not close.
Among the reasons for this anomaly are described:
- hereditary factor;
- mouth breathing - in this case, the child needs to consult an ENT doctor, because it is important to understand why the child breathes through the mouth. Perhaps there was an injury and there is a curvature of the nasal septum, or the presence of adenoids. Sometimes a weakened immune system and frequent colds can also make it difficult for a child to breathe through the nose;
- habit of thumb sucking, prolonged sucking of pacifiers and other objects;
- infantile type of swallowing and the habit of inserting the tongue between the teeth;
- congenital malformations – cleft of the alveolar process of the lip and palate;
- endocrine disorders;
- tumors of the maxillofacial region.
Facial signs of an open bite: the mouth is half-open, but if it is possible to close the mouth, then the face is tense.
Patients complain of the inability to fully bite and swallow food, and often experience a lisp.
There are 3 degrees of severity of open bite depending on the size of the vertical gap: I degree - up to 5 mm, II degree - from 5 to 9 mm, III degree - more than 9 mm.
They also pay attention to which teeth meet in the lateral sections.
Deep bite.
A deep bite is one in which the upper teeth excessively overlap the lower teeth. Sometimes the lower teeth rest with their cutting edges on the mucous membrane of the palate, then they speak of a traumatic deep bite.
Possible causes (etiology) of deep bite:
- early loss of chewing teeth (due to injury or complications of caries leading to their removal, or their primary absence - adentia);
- violation of nasal breathing;
- incorrect type of swallowing;
- speech dysfunction;
- bad habit of sucking various objects;
- violation of the timing of teething, especially in the lateral parts of the dentition;
- early wear of temporary teeth.
As in the case of open bite, three degrees of deep bite are also distinguished, depending on the severity of the anomaly (that is, on the amount of overlap of the lower dentition with the upper one).
Facial signs of deep bite:
- turning the lower lip outward;
- expressiveness of the chin fold;
- shortening of the lower third of the face (sometimes doctors use the term “bird face”).
As a rule, with this malocclusion, patients complain of difficulty biting and chewing food, and pain in the temporomandibular joint often occurs, and headaches are possible. Very often a speech defect occurs - patients speak through their teeth.
Crossbite.
As the name suggests, in a crossbite, the teeth intersect each other when they meet.
With a crossbite, there is a discrepancy in the size of the jaws in the lateral region. Orthodontists classify this type of bite as a transversal anomaly, and the pathology can be unilateral or bilateral.
Crossbite occurs in both the anterior and posterior regions.
With a lateral type of bite, orthodontists distinguish the following types of this anomaly:
- when the lower jaw is displaced towards the tongue - lingual crossbite;
- towards the cheek – buccal crossbite;
- and towards the palate - palatal crossbite.
Causes of the anomaly:
- bad habits (listed above);
- trauma or damage to the jaw, including birth trauma;
- application of forceps during obstetrics;
- absence of individual teeth;
- disorders of the temporomandibular joint (TMJ) – ankylosis, habitual dislocation of the joint, underdevelopment of the joint on one side;
- indestructibility of the surfaces of baby teeth;
- violation of the sequence and timing of teething.
Frequent complaints from patients and parents:
- the presence of an aesthetic defect with a noticeable discrepancy in the size and position of the jaws;
- difficulty eating;
- violation of sound pronunciation;
- gum disease due to possible injury during chewing and speech;
- problems with the gastrointestinal tract.
As a rule, vertical malocclusions are combined with anomalies in the sagittal direction.
Causes of pathological bite formation
Any malocclusion occurs under the influence of the following factors:
- injuries received during childbirth;
- bad heredity;
- a number of diseases suffered by a woman during pregnancy;
- chronic diseases of the nasopharynx;
- mistakes when feeding a baby with a bottle or breast;
- multiple carious lesions of teeth;
- formation of mouth breathing;
- inadequate, unhealthy diet;
- relative lack of fluoride or calcium;
- exchange failures;
- injuries of the dental system;
- the child adopting an incorrect position during sleep;
- pacifier abuse at an early age;
- habit of sucking collar, finger, toys;
- incorrect posture;
- rickets;
- uneven wear of temporary teeth;
- prolonged replacement of temporary teeth with molars;
- long before they are replaced with permanent ones, removal of temporary teeth.
Signs of a deep bite
Signs depend on the severity of the abnormality.
Mild degree
Often the patient does not notice the external manifestations of the pathology, because with a mild degree, the abnormal bite may not even distort facial features and speech. The main signs are small chips and microcracks of the upper front teeth.
Average degree
In addition to small cracks and chips, the following violations appear:
- increased abrasion of the enamel of the upper teeth on the inside;
- difficulties in pronouncing the sound “s”;
- the lower third of the face visually moves away, its height decreases;
- the act of biting is distorted, which leads to disruption of the entire chewing process;
- problems in the functioning of the temporomandibular joint (clicking, crunching and sometimes pain; it is difficult for the patient to open his mouth wide);
- the lips close unaesthetically - the lower or upper lips come forward strongly.
Severe degree
The most severe consequences of improper jaw development manifest themselves, namely:
- Violations of facial proportions.
Often such distortions are called a “bird” face, when the chin goes back strongly and the upper lip hangs excessively over the lower lip. The lower third of the face is also reduced.
- Trauma to the palate.
Due to the distal bite, the lower incisors reach the upper palate. Soft tissues are subject to mechanical friction not only during eating, but also at rest.
- Deformation of the upper jaw.
The upper teeth protrude forward, and the distribution of the load during chewing becomes completely uneven.
Malocclusions: consequences and complications
Unfortunately, if left untreated, malocclusion can become one of the factors provoking the development of a number of pathological processes in the body. In particular, malocclusion can be a consequence of:
- changes in the principles of functioning of the dental system;
- increasing the load on some teeth and weakening it on others;
- accelerated abrasion of the enamel layer of teeth;
- noticeable increase in tooth sensitivity;
- changes in the shape of the face, loss of its symmetry, appearance of aesthetic defects, disturbances in facial expressions;
- speech dysfunction;
- increasing the risk of injury to the tongue, cheeks, gums;
- increasing the risk of periodontal disease;
- TMJ damage;
- the appearance of inflammatory processes;
- problems arising during prosthetic and implantation procedures;
- the appearance of night apnea;
- respiratory dysfunction;
- the occurrence of diseases of the nasopharynx, digestive organs, and respiratory tract.
Dental bite: what is it?
Teeth bite is the position of the dental rows relative to each other with full closure and maximum contact.
An experienced doctor can easily determine the presence of pathology by only asking the child to close his mouth and clench his teeth tightly. If the teeth grow correctly, the child develops according to his age and without deviations, then the closure will be correct and physiological. In this case, the chewing load on the teeth is distributed evenly, the smile looks aesthetic, and the dentition is even.
Any closure error indicates a pathological, incorrect bite. The pathology requires mandatory correction, as it negatively affects not only the appearance, but also the general health of the child.
There are three stages of bite formation:
- temporary - all milk teeth;
- replaceable - some of the milk teeth have already been replaced by molars;
- permanent - only molars.
Malocclusion can develop at any age, but pathological occlusion is more often diagnosed in children. This is for the best, since in childhood it is much easier and faster to correct a bite.
Rodikova Tatyana
Why is malocclusion harmful in young children? The answer can take a long time... But first of all, it is harmful and dangerous because it does not allow the child’s jaw to develop correctly. And as a result, problems grow like a snowball. Pathologies of primary occlusion lead to improper growth of permanent teeth - new displacements, crowding. Therefore, I always ask you to bring your children for preventive examinations - so that they can be seen, monitored, and corrected in time.
The main stages of correcting malocclusion
Orthodontics deals with the correction of pathological occlusion. In this case, the therapy program includes several successive stages.
- Diagnostic measures. To make a correct diagnosis and prepare a treatment program, doctors may need radiovisiography, orthopantogram or CT data. The resulting images help to assess the severity of changes that have occurred in the structure of the dental system.
- Dental sanitation of the oral cavity (professional hygiene, treatment of caries).
- Fight against accompanying pathological processes.
- Installation of braces or other corrective structures.
- Retention measures that allow you to consolidate the results obtained during orthodontic treatment (wearing dental retainers).
Correcting a bite is a difficult, lengthy and expensive procedure that requires the patient to have great patience and a responsible approach to compliance with all medical instructions. However, only in this way can one achieve preservation of the aesthetics of the dentition and prevent the development of a number of pathological processes.
Braces. Bite correction
To correct bites, dentists use the following systems:
- removable structures (mouth guards, plates, etc.);
- non-removable – vestibular braces (metal braces, sapphire braces and ceramic braces) and lingual braces.
Bite correction (orthodontics) is not a painful procedure, but it requires patience and time, and then in due time you will certainly get an excellent result. Nowadays, having a beautiful smile is no longer a luxury, but an affordable pleasure. Agree, having healthy teeth is important, but their aesthetic appearance is no less important. A beautiful smile immediately puts its owner at ease and makes him a charming and pleasant conversationalist. Of course, to correct uneven teeth you will need patience and some time, but it is worth it. Today, even adults get braces because they want to have straight teeth and it’s never too late to make this dream come true. We can offer installation of various types of braces:
- classic braces;
- transparent aesthetic sapphire braces;
- lingual braces (installed on the lingual side);
- ceramic braces.
The lingual brace system is completely invisible, as it is located on the surface of the teeth that faces the tongue, where its clasps are attached. When correcting a bite, one of the main difficulties of working with lingual braces is that, unlike vestibular braces, they are very difficult to place immediately on the teeth in order to begin treatment to correct the shape of the teeth. Therefore, first, braces are attached in a dental laboratory to plaster models of your teeth, and only then, in their final form, are they moved to your teeth. This type of braces requires special education from an orthodontist and a fundamentally different set of tools to install. The entire installation procedure lasts 2-3 hours. This, among other things, explains the considerable difference in price compared to vestibular braces. Lingual braces also have their disadvantages. For example, they are less convenient than their counterparts to use - when eating, talking and brushing your teeth. It usually takes 3-4 weeks to get used to orthodontic equipment. There are also contraindications for installing the system - small dental crowns and multiple missing teeth, as well as the individual characteristics of the patient’s body (according to the indications of the orthodontist). Sapphire braces are very popular due to their transparency and invisibility on the teeth. True, they usually cost more than standard braces, but the result is much more beautiful. Our specialists will install braces for you in compliance with all the necessary rules and so that the result is achieved within the required time frame. We are waiting for you in our clinic for an orthodontic consultation and installation of braces that will change your appearance and give you a beautiful smile.
The cost of correcting the position of teeth is from 15,000 rubles.
You can receive detailed information about the cost of treatment after consulting a dentist.