Mandibular defects occur due to bone loss due to surgery, chronic inflammation, acquired trauma, gunshot wounds, or congenital anatomical abnormalities.
The architecture of the skull is the most complex among all human bone structures. Of particular importance is the only movable bone of the skull - the lower jaw. With defects of the lower jaw, significant anatomical and functional disorders of the masticatory apparatus, pharynx and larynx occur.
Causes of formation of defects of the lower jaw
Defects of the lower jaw are more often acquired than congenital. Violations of the integrity of the bone tissue of the lower jaw are observed for the following reasons:
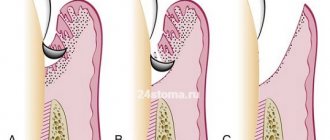
- Large loss of bone tissue can prevent the regeneration of the alveolar process (bone edge); fusion of the edges does not occur due to the large gap, forming bone defects.
- In the case of a small loss of bone tissue (up to 10 mm), fusion of fragments of the lower jaw does not occur due to atrophy of soft tissues or the presence of foreign bodies, and a false joint is formed.
Why does the jaw move forward - how to fix it?
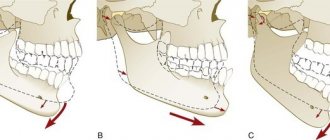
In the structure of dental diseases, anomalies in the development of the dentofacial system today make up a significant proportion. They can affect not only the position of the teeth, but also the structure of the jaws. This causes maximum discomfort to patients, as it deforms the proportions of the oval of the face and seriously affects the appearance. Men and women are equally susceptible to anomalies. Most often, when talking about a protruding jaw, they mean a mesial bite. This anomaly is characterized by the fact that the lower jaw is pushed forward, the lower incisors overlap the upper ones. In some cases, patients are bothered by a protruding upper jaw. In this case we talk about distal occlusion. The lower jaw is inexpressive, the lower lip sinks, and the mouth may look slightly open. The diagnosis is made by the doctor based on the results of an examination of the oral cavity and analysis of x-rays. Sometimes the situation is complicated by crowded teeth. This aggravates the aesthetic problem and can also provoke periodontal disease. The key to proper occlusion is the simultaneous treatment of crowding and distal/mesial occlusion.
Classification of defects of the lower jaw
The classification of defects is influenced by the clinical characteristics of the lower jaw, how many fragments of the lower jaw there are, the presence or absence of teeth in the areas, the location of the defects, etc.
Defects are classified according to their size:
- small (up to 2 cm);
- medium size (2-6 cm);
- subtotal (up to 10-12 cm);
- up to half the length of the jaw;
- total, can be with preservation of continuity of the bone tissue of the lower jaw (cavitary, perforated, cystic and marginal).
Based on the condition of the adjacent soft tissues, defects of the lower jaw can be divided into two types:
- defects without damage to soft tissues;
- defects with loss of soft perimandibular tissue (most often occur during removal of a tumor of various etiologies or as a result of a gunshot wound).
All these defects can be located in different places of the jaw.
Correction methods
Treatment is prescribed depending on the cause and severity; these are cosmetic, orthodontic, conservative or surgical methods. In some cases, therapeutic exercises and massages are indicated.
Cosmetic procedures are indicated for hypertonicity and involve the injection of Botox-based drugs into the muscle area. They relieve stress, give the face a confident, calm expression and restore visual symmetry.
Therapy using conservative methods involves treating root causes such as pulpitis, periodontitis and others. To do this, antibiotics are prescribed to eliminate the infection, analgesics for severe pain, antiseptics and other drugs. The dosage regimen and medications are selected based on diagnostic data.
Massage is performed in rare cases; it is usually part of complex therapy and allows you to solve the following problems:
- relieving hypertonicity or swelling, toning, muscle relaxation;
- elimination of pain syndrome;
- nerve stimulation;
- activation of blood supply to tissues.
Manual therapy will be effective in childhood and in the early stages of diagnosing the problem. In other situations, there will be little benefit from massage.
Orthodontic correction methods help with malocclusions. For therapy, splints, braces, removable or fixed devices are used. If they do not show effectiveness, surgical treatment is prescribed, divided into the following types:
- dental (opening of suppuration, removal of affected tissue);
- otolaryngological (ectomy of formations in the form of cysts);
- maxillofacial (removal of phlegmon, lavage, endoprosthetics);
- to eliminate complications after injuries (bone tissue regeneration, splinting, tying with a ligature).
Complications
The complexity of the consequences depends on the degree of pathology, corrective measures taken and other reasons. In some cases, the problem can be quickly eliminated with a small correction or cosmetic methods. But in case of complications, surgery is necessary, since destruction of the TMJ is likely. Risks also include dysfunction of the dentition and the formation of malignant tumors. Complications develop in the absence of contact with a doctor, non-compliance with the treatment regimen, or complete ignoring of the problem. Over time, the situation worsens and becomes more difficult to correct.
Prevention
To eliminate complications and the development of the problem, the following preventive measures are recommended:
- daily brushing of teeth using special brushes and pastes;
- removing food debris with irrigators;
- eradication of bad habits, teaching the child the features of oral hygiene;
- Regular visits to the dentist to monitor the condition and timely treatment.
A nutritious diet and giving up bad habits, such as smoking, are mandatory. When wearing mouthguards, you should refrain from eating solid food to eliminate the risk of jaw row injuries.
Diagnosis of defects of the lower jaw
Diagnosis of pathology primarily consists of examining the bite - the presence, number and stability of dental units on jaw fragments are noted, and the immune state of the body is also taken into account.
In addition to a visual examination and studying the patient’s medical record, it is necessary to conduct a number of clinical examinations to help determine the correct treatment tactics.
Diagnostic methods consist of:
- X-ray examination;
- MRI, CT of the jaw;
- CT scan of the jaw 3D - performed if it is necessary to create individual clamps to connect the broken ends of the jaw.
Microsurgical operations of maxillofacial surgery
Microsurgery is a universal method used in almost all surgical disciplines to eliminate a defect in a particular tissue. In the human body, there are more than 400 donor sites with an axial type of blood supply, from which taking tissue does not cause any harm to the further blood supply of the entire organ. In the reconstruction of the jaws, the main place is played by the property of the flap with the presence of such a quantity and quality of bone that will make it possible to recreate the anatomical integrity of hard tissues and in the future the possibility of use for dental implantation and prosthetics .
For total and subtotal defects of the mandible, a fibular skin-bone flap . The fibula has sufficiently large supporting properties, having a fairly large amount of cortical component, and can be easily modeled to recreate anatomical contours. An iliac or otherwise inguinal skin-bone flap is optimal for the reconstruction of small defects of the lower jaw; in the latter cases, it is sometimes possible to use a free iliac bone.
For total and subtotal defects of the upper jaw, radial skin-bone and fibular skin-bone flaps are optimal. In cases where the defect covers the zygomaticomaxillary buttress in combination with a defect in the alveolar process, it is possible to fill the bone defect with corticocancellous parietal grafts and mandibular grafts taken from the ramus and mental region with free grafts of mesenchymal origin, which is optimal for reconstruction of the middle zone faces.
Of course, the dominant algorithm remains aimed at engrafting the flap on a vascular pedicle. If you have to choose between convenience for subsequent dental implantation in the form of the presence of a cortical plate of the bone component of the autograft in the area of the recreated alveolar process for subsequent implantation and this somehow reduces the reliability of the vascular anastomosis, it is necessary to choose the reliability of engraftment. Disputes often arise between implant surgeons and reconstructive surgeons about how the iliac bone should be positioned in the defect area, but experience shows that there can be no compromises, since in case of thrombosis of the vascular anastomosis, the entire flap is lost. It is also necessary to understand that the location of the spongy component in the area of the alveolar process does not interfere with subsequent implantation, since a new one is formed within 6 months.
To return and normalize chewing function and the ability to eat, it is necessary to have:
- 1. Lips and complex of swallowing organs.
- 2. Presence of jaws.
- 3. The presence of teeth and a bite that provides adequate chewing.
- 4. Presence of buttresses.
- 5. Stabilization of the TMJ.
- 6. Synchronicity of the masticatory muscles.
- 7. Mental balance of the patient.
In the literature, we did not find a specific algorithm or approaches aimed at returning such vital abilities as sucking and swallowing, chewing and normalization of speech function. To normalize the patient's nutrition, the presence of lips is necessary, otherwise salivation occurs, followed by maceration of the skin and the inability to receive and send food into the esophagus. Patients with defects of the soft tissues of the perioral area constantly suffer from gastritis, inflammation of the oropharynx, since the vacuum property of food evacuation into the esophagus is reduced, many adapt to swallow with an open mouth, throwing their head back; in the latter, the absorption of carbohydrates is impaired, since saliva takes part in cleansing the oral cavity from food residues, plaque and bacteria, thanks to its buffering properties, it neutralizes the negative effects of strong acids and alkalis within the buffer capacity, provides the supply of ions necessary for the remineralization of teeth, and has antibacterial, antifungal and antiviral properties. Claude Bernard proved that we recognize the functions of an organ by identifying the consequences of its absence. From the point of view of the functional return of the ability to eat, the second place in our algorithm is the presence of jaws. To eliminate defects in part or the entire jaw, we use preoperative planning.
Preoperative planning of the jaws is carried out using 3D visualization programs that allow modeling the sizes and shapes of autografts, taking into account the positioning of the condylar processes of the lower jaw in the temporal fossae (in the anterior-superior position in the articular cavities) according to CT scans. Despite the fact that we perform reconstruction in the previous bite, most often we have to deal with an already remodeled TMJ and a broken bite. Therefore, planning is necessary taking into account the subsequent achievement of centric occlusion in the centric relation. A functional study of occlusion consists of comparing central occlusion (CO-occlusion in which there is maximum contact between the teeth of the upper and lower jaw) and the central ratio (CO-condition in which the heads of the lower jaw occupy an anterior-superior position in the articular sockets). If there is a significant difference, a description of the differences is required. Thus, a significant difference between these conditions is more common with asymmetric deformations and with Angle class II deformities. Determining the CA is important for correctly drawing up an operational plan.
When planning the elimination of maxillary defects, we take into account the need to restore the buttresses, as well as the air supply of the upper jaw. Buttresses are the most important component for supporting the alveolar process, otherwise mobility of the upper jaw occurs after prosthetics.
Although restoration of the lost maxillary cavity and mucous lining is not possible, restoration of anatomical proximity is necessary, therefore filling the zygomaticomaxillary buttress with ilium is incorrect. It is optimal to use free split mandibular or parietal auto-bone blocks in shape in combination with bone with vascular nutrition. In the future, perhaps with the development of technologies for the use of stem cells, we will learn to restore the true mucous lining of the maxillary or paranasal sinuses.
In the reconstruction of the upper jaw, we use a fibular autograft for the reconstruction of total defects and a radial one for subtotal defects. When a radial skin-bone flap is subsequently used to place dental implants, it becomes necessary to reconstruct the second cortical-spongy layer of the alveolar process on the lingual side, which can be done using parietal or mandibular free autoblocks.
In maxillofacial microsurgery , when it is necessary to recreate bone curves, in the choice of grafts with bone, we are limited to iliac, fibular, and radial flaps, since only the latter allow 3D modeling of the bone component congruent with the defect.
of one-stage reconstruction after resection still remains open in the country . It is necessary to understand that if the reconstruction is not performed simultaneously with the resection of the jaw and even a temporary titanium structure is not applied to maintain the bite, remodeling of the temporomandibular joint occurs, both from the healthy and from the pathological side, and a violation of the trophism of the masticatory muscles. In these cases, before placing dental implants and before prosthetics of the implant, orthodontic fixation of the bite is performed in the form of braces and mini-implants, as well as muscle relaxation of the masticatory muscles on the part of the healthy jaw using Botex therapy or myotronic.
HISTORY OF THE PROBLEM
In our opinion, microsurgical autotransplantation for the purpose of jaw reconstruction has gone through several stages in its development:
Stage 1 – high-quality autograft collection, minimal modeling, and transfer to the recipient area. The main objective of this stage was to ensure graft engraftment (from 1978 to 1990).
Stage 2 included better modeling of autografts using conventional radiographs and wax templates. The main task of this stage was to restore facial aesthetics. The impaired function of the lower jaw was restored after a series of additional corrective operations and removable dental prosthetics (from 1990-1995). Stage 3 - computer modeling of the lower jaw and restoration of chewing function using prosthetics using dental implants. The main goal of this stage is to restore facial aesthetics and chewing function of the lower jaw without the use of additional corrective surgeries (from 1995 to 2011). Stage 4 - restoration of not only an ideal bite and stabilization of the TMJ, but also elimination of the imbalance of the masticatory muscles (in fact, this article opens the 4th stage in the history of maxillofacial microsurgery).
We have developed an algorithm for treating patients with jaw defects: 1. Preoperative 3D planning and production of stereolithographic and bite templates. Planning taking into account subsequent dental implantation and prosthetics. Selecting the optimal flap. 2. Restoration of buttresses, if possible, and the anatomical contours of the alveolar process of the jaws using free and pedunculated bone grafts. 3. Remodeling of the TMJ when eliminating subtotal defects of the lower jaw. 4. Dental implantation and prosthetics.
Microsurgical operation: resection of the lower jaw affected by the tumor with simultaneous reconstruction with a fibular graft on a vascular pedicle
| 1. Resection of the lower jaw affected by the tumor within healthy tissues | ||
| 2. Stage of control of resection according to the preoperative template | ||
| 3. Harvesting the fibula on a vascular pedicle | ||
| 4. Stage of modeling the harvested transplant using the author's device Karayan A.S. and Nazaryan D.N. | ||
| 5. Control of the simulated transplant on the preoperative template | ||
| 6. Fixation of the graft on the vascular pedicle to the remaining healthy fragments of the lower jaw | ||
| 7. Microsurgical stage: under a microscope, the vessels from the lower leg and the external carotid artery, jugular vein are sutured, after suturing the vessels, the clips are removed and the tissue taken from the leg is filled with blood, i.e. the flap becomes alive, but on the jaw. | ||
| 8. Control of blood supply - the final stage of microscopic surgery | Watch the video | |
| 9. The patient’s appearance before and after the operation will be practically unchanged; thanks to one-stage reconstruction, after 6 months the person will be completely rehabilitated | ||
In the scientific and clinical department of maxillofacial and plastic surgery of the Federal State Budgetary Institution NCCO FMBA of Russia under the leadership of Professor Karayan A.S. and Ph.D. Nazaryan D.N. Unique surgeries are performed to eliminate jaw defects. Such operations are performed only in 3 medical centers in Russia.