{jcomments on}Treatment of victims with jaw fractures consists of repositioning and immobilization of jaw fragments, as well as drug treatment and physical therapy. Reposition involves aligning or moving facial bone fragments into the correct position. If it is not possible to compare the displaced fragments at once, they are reduced gradually, over several days, using elastic traction. Immobilization means securing the fragments in the correct position for the period necessary for their fusion (consolidation), i.e. until callus formation. On average, this period is 4-5 weeks for uncomplicated healing of a fracture of the upper jaw and a unilateral fracture of the lower jaw. With a bilateral fracture of the lower jaw, the immobilization period can increase to 5-6 weeks. Drug and physical treatment are necessary to prevent the development of complications during the period of consolidation of fragments (antibacterial, anti-inflammatory, antihistamines; medications that improve the rheological properties of blood and tissue microcirculation, immunostimulants, drugs that optimize osteogenesis). In addition, the question of the advisability of preserving teeth in the fracture gap and the need for therapeutic measures in relation to these teeth must be resolved.
Why is teeth splinting necessary?
There are various methods and technologies for splinting. However, they are united by their main function - ensuring the stability of the dentition. Several teeth are attached to each other using structures that provide solidity and prevent changes in the position of any tooth located in such a ligament. In some situations, splinting not only returns functionality to teeth, but also avoids their removal.
Indications
- Splinting teeth for periodontitis. Splinting of mobile teeth is carried out at an advanced stage of periodontitis, when bone tissue atrophy leads to exposure of the neck and loss of stability.
- For jaw injuries and tooth dislocations. It is necessary to ensure the immobility of the tooth/teeth and relieve part of the chewing load.
- Splinting of teeth after bite correction. Retainers are placed on the dentition, which prevent the teeth from returning to their original (abnormal) position.
- Temporary splinting of teeth during invasive operations in the jaw area to prevent changes in the position of the teeth (the procedure is performed in a limited number of cases).
Contraindications
- Periodontitis (inflammation, bleeding, infection in periodontal pockets).
- Poor condition or absence of supporting teeth.
- Caries and its complications.
- Poor oral hygiene.
How to eat after splinting
Hard splinting involves difficulties in eating, but at the same time, during this period it is especially important for the body to receive a large amount of vitamins, minerals, and nutrients required for the speedy regeneration of bone tissue. The patient's menu after splinting usually includes various nutritious broths, fruit, vegetable and meat purees (baby purees), semi-liquid and liquid porridges. It is necessary to monitor the content of large amounts of protein, calcium, phosphorus, and zinc in food. It is possible to replace some meals with infant formula or sports nutrition, since in both cases the content of substances necessary for the body is high.
It is strictly forbidden to drink any alcoholic beverages during treatment, especially if, in addition to the jaw, there is also a traumatic brain injury. In addition, you should not try to eat solid foods that require chewing. Firstly, it can cause severe pain. Secondly, it can lead to improper healing of damaged bone tissue.
If you receive injuries that have symptoms similar to a jaw fracture: acute pain, bleeding, immobilization of the jaw, and so on, you should immediately seek professional help. Attempts at self-treatment or complete lack of treatment cause irreparable harm and lead to loss of dental functionality.
Material for splinting teeth
Several types of materials are used for splinting teeth, the choice of which depends on the characteristics of a particular clinical case. The main ones are fiberglass, aramid threads, metal and ceramics. When it comes to retainers, removable silicone mouth guards can be used. Composite dental splinting materials are used to secure the splint. Separate splinting of teeth with composites is not carried out.
Fiberglass
Adhesive fiberglass tape is used as a splint. Splinting teeth with fiberglass tape offers a number of benefits. This is an aesthetic and hypoallergenic material that has the necessary strength for reliable fixation. The service life of fiberglass tape for splinting teeth is 3-4 years. Therefore, it is not suitable for long-term use. The average cost of splinting teeth with fiberglass ranges from 3,500 to 8,000 rubles, depending on the area of the jaw and the number of teeth.
Cable-stayed
An aramid thread is used, which is several times stronger than steel. It is much more durable than fiberglass, safe for fabrics and resistant to the external environment. It is not recommended to splint the front teeth with aramid, since the material has a rather noticeable yellowish tint. The cost of cable-stayed splinting of teeth with floss starts from 2000 rubles per tooth.
Byugelnoye
Splinting teeth with clasp dentures allows you to solve two problems at once - fixing mobile teeth and restoring lost units. The clasp prosthesis has a metal frame and a soft base. Attached to abutment teeth using clasps or micro-locks. Bugel splinting of teeth will cost approximately 35,000 rubles and more.
Retainers
This type does not belong to classic splinting. The primary goal of retainers is to prevent teeth from shifting back into the wrong position after braces are removed. Fixed retainers are usually made of metal or fiberglass and are essentially no different from a regular splint. Removable retainers can be in the form of trays or plates. You need to wear retainers for a long time (at least 5-6 years after removing braces), and sometimes for life. Cost: from 3,000 to 10,000 rubles per jaw, depending on the system.
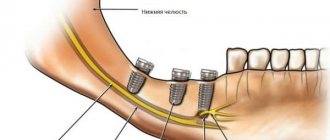
Splinting for jaw fractures
In case of jaw fractures, it is necessary to fasten the damaged areas of the bone and prevent the teeth from moving. The result is a rather bulky structure made of wire, hooks and silicone loops. The cost of the procedure can reach up to 20,000 rubles and depends on the complexity of the fracture.
Crowns
Installation of a fixed denture is also one of the types of splinting, since it allows you to ensure the stability of a section of the dentition with the help of artificial crowns. Splinting of 1 tooth is carried out using the single prosthetic method. To splint 2 or more teeth, a bridge is most often placed. The cost of single prosthetics starts from 8,000 rubles, multiple - from 30,000 rubles. This is the minimum price for metal ceramics; a prosthesis made from more modern materials will cost much more.
Therapeutic (permanent) immobilization using non-laboratory dental splints
Individual dental wire splints by Tigerstedt. Types of Tigerstedt dental splints: - smooth splint-bracket; — bus-bracket with a spacer bend; - tire with hook loops.
The splints are made of aluminum wire d=1.8-2.0 mm and 12-15 cm long. They are tied to the teeth using bronze-aluminum wire d=0.5-0.6 mm. The splint is bent individually for each patient using crampon forceps. General rules for applying dental splints . 0.5 ml of a 0.1% atropine solution is injected subcutaneously to reduce salivation, splinting is carried out under local anesthesia, it is necessary to remove tartar to freely pass the ligature into the interdental space, bend the splint from the side of the fracture, try it on the teeth in the mouth, and bend it outside the oral cavity, the splint should be adjacent to the neck of each tooth at least at one point, the splint is tied to each tooth with a ligature wire, which is twisted clockwise. The production of the splint begins with bending a large hook that clasps the first tooth, or a hook spike inserted into the interdental space. To try on a splint, it is applied to the teeth in the mouth.
Smooth splint.
It is used to treat fractures of the lower jaw, provided that the larger fragment contains at least four, and the smaller fragment contains at least two stable teeth.
Smooth splint
Indications for use : linear fractures of the lower jaw, located within the dentition, without displacement or with easily reducible fragments, fractures of the alveolar process, fractures and dislocations of teeth, tooth mobility in acute odontogenic osteomyelitis and periodontitis, fractures of the upper jaw (Adams and Dingman methods), to prevent pathological fracture of the lower jaw. After treatment, before removing the splint, loosen the ligatures and check the lack of mobility of the fragments by rocking them. The splint is removed after 4-5 weeks. The patient needs to take liquid food. The doctor should regularly examine the patient 2-3 times a week. In this case, it is necessary to monitor the state of the bite, the strength of fixation of the fragments, the condition of the tissues and teeth in the fracture gap. When the fixation of the splint on the teeth becomes loose, it is necessary to tighten the ligatures by twisting them. If the ligature bursts, it is replaced with a new one. The patient is taught hygienic measures to prevent the development of gingivitis. For this purpose, the patient should brush his teeth and splint with toothpaste and a brush 2 times a day, after each meal, remove food debris with a toothpick, and rinse his mouth with antiseptic solutions 3-5 times a day.
Busbar with spacer bend.
The spacer bend prevents lateral displacement of fragments.
Busbar with spacer bend
Indications for use : fracture of the lower jaw within the dentition and the presence of a bone tissue defect of no more than 2-4 cm, fracture of the lower jaw without displacement or with easily reducible fragments, if the fracture gap passes through the alveolar part, devoid of teeth.
Tire with hook loops.
The splint is most often used to treat jaw fractures. Two splints with hooking loops are made for the teeth of the upper and lower jaw.
Tire with hook loops
Indications for use : fractures of the lower jaw outside the dentition, within the dentition - in the absence of four stable teeth on the larger fragment and two stable teeth on the smaller one, fractures of the lower jaw with difficult-to-reduce fragments requiring traction, bilateral, double and multiple fractures of the lower jaw, fracture of the upper jaw (with the obligatory use of a chin sling), simultaneous fractures of the upper and lower jaw. When making a splint, its hook loop should be at an angle of 45° relative to the gum. The towing loops are bent on the tire so that they are located in the area of the 6th, 4th and 2nd teeth. If the patient does not have these teeth, then hooking loops are made in the area of other teeth that have antagonists. Usually, 3-4 hook loops are bent on the splint adjacent to the teeth of the larger fragment, and 2-3 hook loops on the smaller one. The base of the loop must be within the crown of the tooth. If the displacement of the fragments is large and it is difficult to bend one splint onto both fragments, splints can be made and secured to each of the fragments. After their reposition, rubber rings are put on the hook loops at an angle so that they create compression of the fragments, which significantly prevents their movement. Periodically (2-3 times a week) the patient is examined, ligatures are tightened, rubber rings are changed, the vestibule of the mouth is treated with antiseptic solutions, and the condition of the bite is monitored. 10-25 days after applying the splint, an X-ray examination is performed to monitor the position of the fragments. After fusion of the fragments, before removing the splints, it is necessary to remove the rubber rings and allow the patient to walk for 1-2 days without fixation, eating soft food. If the fragments do not move, the splints are removed. If there is a slight change in the bite, the rubber traction is retained for another 10-15 days.
Splinting using the A.P. method Vikhrov and M.A. Slepchenko.
The authors proposed using a polyamide thread to strengthen the attachment of the splint to the teeth. To do this, take a bronze-aluminum wire ligature, fold it in the form of a hairpin and insert both of its ends into one interdental space from the mouth towards the vestibule of the mouth. The ligature is tightened so that a small loop is formed on the lingual surface of the interdental spaces. A similar procedure is performed in the area of all interdental spaces. Take a polyamide thread with a diameter of 1 mm and pass it through all the loops on the lingual side, the ends of the thread are brought out into the vestibule of the mouth behind the last teeth on both sides. Next, a previously made splint is placed on the teeth so that it is located between the two ends of the same previously made bronze-aluminum ligatures, which are then twisted. According to the authors, the advantages of their method are the following: stronger fastening of fragments, reduction of splint fastening time, and absence of trauma to the gum mucosa.
Splinting using the Vikhrov-Slepchenko method
Tooth standard splints.
Good manual skills are required to make custom wire splints. Their production requires a lot of time and frequent fitting to the dental arch. It is especially difficult to bend them in case of malocclusion, dental dystopia, etc. Taking into account the above, standard splints were proposed, which are manufactured in the factory, do not require bending of the hook loops and simplify splinting. In Russia, standard belt tires were proposed by V.S. Vasilyev. The tire is made of a thin flat metal strip 2.3 mm wide and 134 mm long, which has 14 hooking loops. The tire bends easily in the horizontal plane, but does not bend in the vertical plane. The Vasiliev splint is cut to the required size, bent along the dental arch so that it touches each tooth at least at one point, and tied to the teeth with ligature wire. The advantage of the splint is the speed of its application . The disadvantage is the impossibility of bending it in a vertical plane, which does not allow to avoid injury to the mucous membrane in the lateral parts of the jaws due to the discrepancy between the splint and the curve of Spee. This splint is not suitable for single-jaw splinting due to its low strength. Abroad, there are various designs of standard tires made of steel wire (Winter tires) and polyamide materials that can be bent in any plane. Tires are manufactured with pre-made hooks.
Teeth splinting technique
Installation of permanent tires made of metal, fiberglass or aramid almost always follows a similar scenario.
- Consultation, determination of indications and contraindications.
- Professional teeth cleaning, etching of enamel with a special solution.
- Forming a groove in the enamel to attach the splint (in some cases this can be avoided).
- Primary fixation of the splint using dental glue.
- Application of composite material.
- Illuminating the composite with an ultraviolet lamp until it hardens.
- Tire grinding.
The splinting procedure for injuries and fractures is carried out under the guidance of a maxillofacial surgeon and differs from the classical technique in the design of the splint and the method of its fixation. Installation of a custom retention tray requires taking impressions.
Features of splinting chewing and anterior teeth
Conceptually, the splinting procedure is the same for molars and incisors, but from a purely technical point of view there are nuances. Splinting the lower anterior teeth allows the splint to be placed on the lingual side, whereas on the upper anterior teeth it is usually placed on the vestibular surface. This is why it is preferable to use more aesthetically pleasing fiberglass splints in the area of the upper anterior teeth. Splinting of lateral teeth (molars) requires installation of a splint on the chewing surface. Such nuances are explained by the anatomical and functional characteristics of various groups of teeth, which must be taken into account to achieve an optimal result.
Attention!
If the procedure was performed by a qualified doctor and went without complications, the effectiveness of the treatment will be high. The process of addiction may be accompanied by discomfort and problems with diction. Some patients complain that their teeth hurt after splinting. Within a few days, pain and discomfort should almost completely disappear. If this does not happen, you need to consult a doctor.
Therapeutic immobilization of jaw fragments using laboratory-made splints
Laboratory-made splints are classified as orthopedic immobilization methods. They perform both an independent immobilization function and can be an additional device for various surgical methods of fastening fragments. Removable orthopedic structures include supragingival splints (simple or inclined plane Weber supragingival splint, Vankevich splint, Vankevich-Stepanov splint) and Porta supragingival splint. Non-removable orthopedic structures include dental splints with fixing elements of various modifications. Indications for the use of laboratory-made splints : - severe injuries of the jaws with significant defects of bone tissue, in which bone grafting of the jaw is not performed; — the presence of concomitant diseases in the victim (diabetes mellitus, stroke, etc.), in which the use of surgical immobilization methods is contraindicated; — the patient’s refusal to surgically fix the fragments; — the need for additional fixation of fragments simultaneously with the use of wire splints. To produce laboratory splints, the following conditions are required: a dental laboratory, special materials. Dental work is carried out by dental technicians.
Simple Weber dentogingival splint.
Can be used independently or as one of the main elements when using the surrounding suture method for fractures of the lower jaw. The Weber splint is used for significant defects of the lower jaw as a result of traumatic osteomyelitis or after resection of the lower jaw for a tumor. In these cases, long-term wearing of the splint (for 2-3 months) can lead to the elimination of pronounced lateral displacement of the lower jaw after removal of the splint. The Weber splint is prepared in the laboratory, after taking impressions of jaw fragments. To prevent lateral displacement of fragments, an inclined plane is made on it in the area of the molars. You can make a splint directly in the patient’s mouth from quick-hardening plastic.
Bus Vankevich and bus Vankevich-Stepanova.
They are dental splints supported on the alveolar process of the upper jaw and the hard palate. In the lateral sections it has two inclined planes facing downwards, which abut against the anterior edges of the branches or the alveolar part of the lateral sections of the body of the lower jaw, mainly from the lingual side and do not allow fragments of the lower jaw to move forward, upward and inward. The Vankevich splint is used to fix and prevent lateral and rotational displacement of fragments of the lower jaw, especially with significant defects, due to the emphasis of the inclined planes on the anterior edges of the branches of the jaw. The Vankevich splint as modified by Stepanov differs in that instead of a maxillary base there is a metal arch, like a clasp prosthesis. The Port splint is used in case of a fracture of the edentulous lower jaw without displacement of the fragments and the patient does not have removable dentures and teeth in the upper jaw. The splint consists of two base plates for each jaw, similar to complete removable dentures, rigidly connected to each other in the position of central occlusion. There is a hole in the front section of the tire for food intake. The Porta splint is used in combination with wearing a chin sling bandage.
Dental splints with fixing elements.
Used for immobilization of fragments of the lower jaw in the presence of a bone tissue defect within the dentition, when the fragments have a sufficient number of stable supporting teeth. These splints consist of metal caps fitted to the teeth of the lower jaw. The caps are soldered together and fixed on the teeth of each fragment. With the help of various locks (pins, levers, etc.), after their reposition, the fragments are secured for the period necessary for consolidation. The teeth used for splinting are not prepared.