The current state of affairs and the rapid development of dentistry and plastic maxillofacial surgery require detailed knowledge of the blood supply to the face, including the upper and lower jaws (HF, LF). In the literature over the past 40 years, we have not found any works devoted to the study of blood supply to the HF and LF. Meanwhile, this knowledge is necessary for various surgical interventions on the jaws, fractures, wounds, to interpret the paths of spread of purulent-inflammatory processes on the face.
The HF is supplied with blood by a large number of large arteries, which widely anastomose with each other [2, 4]. As for the sources of blood supply to the NP, expert opinions differ. Some authors [5] consider the inferior alveolar artery to be the main and only source of blood supply to the NP. According to others [1-3], in addition to the inferior alveolar artery, additional arteries are involved in the blood supply to the NP.
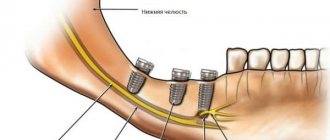
The LF is supplied with blood from a number of additional extraosseous (extraosseous) arteries: the temporal, arteries of the pterygoid muscles, masticatory, facial, lingual and mylohyoid. The main arteries supplying blood to the NP are considered to be 6 intraosseous (intraosseous) arteries: maxillary, inferior alveolar, lingual, transverse facial artery, masticatory and facial.
The purpose of the study is to study the main and additional sources of blood supply to the HF and LF - extraosseous and intraosseous arteries, to study their participation in the blood supply of the jaws and their relationship with facial tissues.
Material and methods
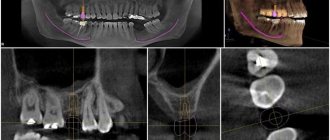
The work is based on the study of 130 isolated NP preparations removed from corpses in Tver morgues, and 20 embalmed corpses of people aged 20 to 70 years, studied at the Department of Topographic Anatomy and Operative Surgery of the TSMA.
The following methods were used: morphometric measurements, contrast radiography, decalcification, preparation, recording and photography. Using 16 NP preparations, experimental ligations of the inferior alveolar artery in the initial part of the mandibular canal were performed to identify additional intraosseous arteries involved in the blood supply to the NP.
For contrast angiography, injections were made through the external carotid or inferior alveolar artery of lead, diluted in petroleum jelly and turpentine in the following ratio: lead - 60 g, petroleum jelly - 15 g, turpentine - 15 g.
Arteries, veins and nerves of the upper and lower jaw
This article describes the following anatomical landmarks and their relationship to oral implant surgery: external carotid artery, maxillary artery, pterygopalatine fossa, capitis veins, and trigeminal nerve.
External carotid artery
The arteries supplying the face, upper and lower jaw mainly originate from the external carotid artery. However, branches of the ophthalmic artery (a branch of the internal carotid artery) supply blood to the forehead, scalp, upper eyelid and nose. The external and internal carotid arteries (Figures 1-1 and 1-2) arise from the common carotid artery at the level of the superior border of the thyroid cartilage. The external carotid artery has eight branches:
- Three anterior branches: superior thyroid artery, lingual artery and facial artery.
- Two terminal branches: the maxillary artery and the superficial temporal artery.
- Two posterior branches: the occipital auricular artery and the posterior auricular artery.
- One medial branch: ascending pharyngeal artery.
Figure 1-1 Main branches of the aortic arch
Fig 1-2 Main branches of the external carotid artery
Maxillary artery
The maxillary artery (Figure 1-3) arises from the external carotid artery in the parotid gland as a terminal branch. The branches of the maxillary artery can be divided into three parts:
- Part I or mandibular part (located within the parotid salivary gland and in front of the external auditory meatus): In this part, the maxillary artery gives off branches to the ear, dura mater, temporomandibular joint, mandibular teeth, and mylohyoid muscle.
- Part II or pterygoid part (located in the infratemporal fossa): The branches here mainly go to the muscles involved in the process of mastication, the skin and mucous membrane of the cheek, and also to the buccal muscle through the buccal artery.
- Part III or pterygopalatine part (branches in the pterygopalatine fossa after entering through the pterygomaxillary fissure): the branches here mainly go to the hard and soft palate through the descending palatine artery, to the molars and premolars of the maxilla through the posterior superior alveolar artery, to the upper part of the pharynx and the tympanic cavity through the artery of the pterygoid canal, to the nasopharynx and sphenoid sinus through the pharyngeal artery and to the anterior teeth of the upper jaw through the infraorbital artery.
Figure 1-3 Course of the maxillary artery
The maxillary artery ends with the sphenopalatine artery on the nasal septum after dividing into nasal branches. Figure 1-4 shows in detail the branches of all three parts of the maxillary artery.
Arteries of the tooth
The supply of nerves and blood to the jaws depends on the nerves and blood vessels that supply them. The upper jaw is considered to be part of the middle zone of the face, and the lower jaw is the lower part of the face, respectively, they have a separate blood supply. Although in the alveolar bone the maxillary and mandibular nerves and vessels are mirrored in relation to each other, there are anatomical differences with additional branches and adjacent structures such as the mandibular mental foramen or the greater palatine foramen in the hard palate.
How are teeth supplied with blood?
The maxillary arterial vessel supplies the deep structures of the face, including the teeth. Branching from the external carotid arterial vessel, it approaches the neck of the mandible. The superior alveolar arterial vessels (anterior and posterior) supply the upper teeth. Smaller branches extend from these vessels, providing blood supply to the teeth, gums and socket walls. A branch of the inferior alveolar arterial vessel supplies the lower teeth, located in the mandibular canal, where it forms dental and interalveolar branches. Through the tops of the foramina, dental arterial vessels enter the root canals of the teeth and then branch into the dental pulp.
All arteries are accompanied by veins of the same name, which are responsible for draining blood from the teeth into the pterygoid venous plexus.
Arteries responsible for blood supply to teeth
- Maxillary artery. From a topographical point of view, the maxillary artery has three parts: mandibular, pterygoid and pterygopalatine. The maxillary artery is the large terminal branch of the external carotid artery. Starting below the temporomandibular joint, it runs along the outer or inner side of the lateral pterygoid muscle, after which it branches in the pterygopalatine fossa.
- Inferior alveolar arterial vessel. It lies between the medial pterygoid muscle and the branch of the mandible. Then it goes along the mandibular bone canal, reaching the mental foramen.
- Dental branches. Suitable for tooth roots.
- Masticatory arterial vessel. It goes above the notch of the lower jaw and supplies blood to the muscle of the same name.
- Mylohyoid branch. It originates near the opening of the lower jaw and, together with the mylohyoid muscle, runs in the groove of the same name. This branch connects to the mental arterial vessel.
- Buccal arterial vessel. Located in the buccal muscle. Responsible for blood supply to the cheeks and gums.
- Posterior superior alveolar artery. Entering its branches into the alveolar canals, it supplies blood to the upper molars, gums and mucous surface of the maxillary sinus.
Features of blood supply in the facial area.
Features of blood supply in the facial area.
The maxillofacial area is supplied with blood by the branches of the external carotid artery, which form a group of anterior, middle and posterior branches.
The anterior group includes the thyroid, lingual and facial arteries.
The middle group consists of the ascending pharyngeal artery, superficial temporal and maxillary arteries.
The posterior group is formed by the sternocleidomastoid branch, the occipital artery and the posterior auricular artery.
Branches of the external carotid artery.
1 – superficial temporal artery; 2 – occipital artery;
3 – maxillary artery; 4 – external carotid artery;
5 – ascending pharyngeal artery; 6 – internal carotid artery;
7 – muscle that lifts the scapula; 8 – trapezius muscle;
9 – suprascapular artery; 10 – brachial plexus;
11 – thyrocervical trunk; 12 - common carotid artery;
13 – superior thyroid artery; 14 – lingual artery; 15 – facial artery;
16 – anterior belly of the digastric muscle; 17 – buccal muscle; 18 – middle meningeal artery.
The outflow of venous blood from the organs and tissues of the maxillofacial region is carried out into the internal jugular vein, which receives blood from the facial vein, pterygoid venous plexus, lingual, thyroid and mandibular veins.
Lymph from the head and neck area collects in the jugular lymphatic trunks, which also receives lymph from the mastoid, parotid, submandibular, peripharyngeal and mental regional nodes.
Regulation of blood circulation in the vascular system of the maxillofacial region is carried out by the nervous and humoral pathways. In addition, the vessels have their own basal tone (myogenic regulatory mechanisms).
The vasomotor center of the medulla oblongata sends impulses along nerve fibers through the cervical sympathetic nodes to the vessels of the maxillofacial region.
The vessels of the face form an abundant network with well-developed anastomoses, so wounds on the face heal quickly.
When carrying out all procedures , you should be as careful as possible to avoid intra-arterial and intravenous administration of the drug.
It is safe to inject the drug into the periosteum using cannulas, which are less dangerous than needles.
DANGEROUS AREAS FOR INSTRUCTION OF FILLERS.
Projection of the bony openings of the facial part of the skull.
- supraorbitalis (supraorbital foramen) - the place of exit of the supraorbital SNP - the place of intersection of the upper bony edge of the orbit with a vertical line drawn through the medial edge of the iris. SNP is covered by m. orbicularis oculi, direction of movement - up under m. corrugator and m. frontalis.
- infraorbitalis (infraorbital foramen) – the exit point of the infraorbital SNP – the intersection of a point 1 cm below the lower bony edge of the orbit with a vertical line drawn through the medial edge of the iris. SNP is covered by m. orbicularis oculi and m. levator labii superioris direction of movement is downward and medial.
- mentalis (mental foramen) – the place of exit of the mental SNP – the place of intersection of the mid-height of the lower jaw at the intersection with a vertical line drawn through the medial edge of the iris. SNP is covered by m. depressor labii inferioris, the direction of travel is upward and medial.
Deep injections into the projection of the neurovascular bundles can lead to compression of blood vessels and disruption of blood supply, can be painful and cause changes in skin sensitivity.
The nasal region contains many terminal arteries.
When correcting this area, it is important to take special care, because the terminal branches of the arteries pass there, and the injection of Hyaluronic acid can have catastrophic consequences.
With increasing scientific evidence regarding embolization of small facial arteries following filler injections, nasal procedures should only be performed using cannulas.
From the ophthalmic artery Dorsal nasal artery Vessels of the angle of the nose Lateral nasal artery
From the external carotid artery to the columella artery.
Interbrow area.
When injecting fillers into the glabella area, local necrosis may develop due to the small number of vessels in this area.
In the area delimited by the points of fixation to the bone m. orbicularis oculi from the sides, m. corrugator supercilii above and m. procerus from below, the distribution of the filler is difficult (especially drugs with high viscosity HA), creating a high local pressure of the drug on the tissues and vessels.
Temporal and periorbital regions.
The superficial temporal (sentinel) vein is located in the temporal region behind the artery of the same name and follows its course. Crossing the temporal region 1-1.5 cm above the zygomatic arch, the vein in the layer of subcutaneous fatty tissue is directed to the auricle.
At the medial edge of the orbit, the angular vein is located superficially ; it communicates through the veins of the orbit with the cavernous sinus of the dura mater.
Careless injection of filler into the lumen of the vein or its excessive amount can lead to thrombosis, hematoma or later complications of an infectious nature.
temporales (temporal branch) of the facial nerve in the temporal region lies under the SMAS and goes to the tail of the eyebrow.
The place of its surface occurrence is located in the projection of a triangle, the apex of which is located 2 cm above the end of the eyebrow, and the base is along the lower zygomatic arch.
The parotid salivary gland is in the shape of an inverted triangle with its base on the zygomatic arch and its apex in the area of the angle of the mandible.
The duct of the parotid salivary gland lies below and parallel to the zygomatic arch under the SMAS layer, it horizontally crosses m. masseter and, entering the buccal muscle, appears in the vestibule of the oral cavity.
Damage to the duct leads to the development of chronic local inflammation of the adjacent soft tissues.
transversa facies (transverse artery of the face) is located in the zygomatic region. Parallel and superior to the parotid duct. The vessel supplies blood to the soft tissues of the area, including the skin and subcutaneous tissue through perforator vessels; the permanent perforator is located in the middle of the distance between the wing of the nose and the ear canal or 3 cm medially and 3.5 below the orbital edge.
When performing procedures with a cannula in the zygomatic region, damage to the permanent perforator should be avoided. transversa facies.
marginalis mandibulae (marginal branch of the mandible) of the facial nerve is located under the SMAS and descends first behind the branch and angle of the mandible and, not reaching the posterior edge of the m. depressor anguli oris, extends onto the face, located at this point on the bone.
Deep bone injections in this area should be carried out with caution, because this branch innervates the muscles of the lower lip and part of the subcutaneous muscle of the neck.
Educational phone numbers : 8-812-248-99-34, 8-812-248-99-38, 8-812-243-91-63, 8-929-105-68-44
Application for ordering products here
Seminar schedule here