There are many myths surrounding the concept of “bad bite”. Many believe that the position of teeth can only be corrected in childhood, the anomaly causes only aesthetic problems, and dental clinics only have braces at their disposal. Is it so? Let's figure it out.
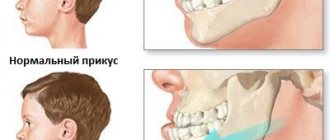
Bite – the arrangement of the teeth when the jaws are closed. With a normal bite, each upper tooth is in contact with its lower “antagonist”, the dentition is even, there are no gaps.
You can correct the position of your teeth not only during the period of active growth. Of course, the easiest way to do this is in childhood. However, it is quite possible to eliminate the anomaly in adulthood. For this purpose, not only brace systems are used, but also various surgical methods, as well as microprosthetics.
It is important to understand that the success of orthodontic procedures depends on the condition of the teeth, the type of bite and the degree of pathology. The stronger the anomaly, the more difficult it will be to correct it.
Types of occlusion defects and methods of their correction
Scientists have calculated that only 40% of the planet's inhabitants are the happy owners of an ideal bite. All others have deviations from the norm to one degree or another. Defects can be critical when they have a negative impact on human health, and practically unnoticeable, not leading to moral or physical discomfort.
The picture below shows occlusion anomalies:
Modern orthodontics includes several methods for correcting malocclusion:
- using braces;
- through surgery;
- using myotherapy (physical exercises) and non-braces corrective devices.
General conclusion
- 1. There is no universal way to correct a bite without the help of braces.
- 2. Each of the alternative methods may not be suitable in a particular clinical case.
- 3. Do not try to correct your bite on your own; be sure to have a personal consultation with an orthodontist!
To make a decision, contact our clinic with highly qualified orthodontists. Make an appointment with us for a consultation or call. Our clinic is located at St. Petersburg, Thorez Ave., 95.
Posted by:
At what age should you start correcting your bite?
Dentists believe that occlusion correction can be carried out at any age using appropriate techniques. Thus, children are not treated with braces because their skeletal system is in active growth, and the bones, including the dentofacial apparatus, have not yet formed. Therefore, young children, before they have permanent teeth yet, are treated with myotherapy, plates and trainers. Note: such methods are used in the presence of non-critical developmental defects. Complex congenital pathologies that have a negative impact on the health or quality of life of the baby are treated surgically.
The optimal period of treatment with braces is from approximately 12 to 16 years. At older ages, the process takes longer.
Important: some dental anomalies can be corrected without the use of braces. The possibility of such treatment is determined by the doctor.
Reasons for development
There are quite a few factors contributing to the occurrence of distal occlusion. Among them:
Hereditary predisposition. If one of the parents had prognathia, then with a high degree of probability the child will also have it.- Abnormal development of the jaws during fetal development. It's always difficult to say what caused the problem. This could be a pregnant woman taking certain medications, drinking alcohol, smoking, etc.
- Mistakes made during breastfeeding. When a baby nurses, his jaws form and develop correctly. If he is constantly bottle-fed, then the muscles are much less involved in the act of sucking. Hence the slow growth of the jaws. To avoid an abnormal bite, when artificial feeding you should use special orthodontic nipples with a small hole. They are shaped like a female nipple and ensure proper development of the facial skeleton.
- The habit of breathing through your mouth. It can develop due to existing diseases of the ENT organs and lung pathologies. From childhood, a person gets used to inhaling and exhaling air through the mouth. Because of this, his upper jaw becomes large and noticeably lengthens.
- Premature removal of milk units. Fangs play a special role in the formation of correct closure. If they are absent for a long time, the functioning of the dentofacial apparatus is disrupted.
- Habit of sucking and chewing on foreign objects. It is especially bad if the child constantly sucks his thumb.
It has also been proven that poor posture and rickets lead to prognathia.
Corrective exercises – myotherapy
As a rule, myotherapy is an addition to the correction of occlusion using various orthodontic devices or as the main method in the treatment of children from 4 to 8 years old. Physical exercises help develop and strengthen facial muscles, stimulate bone growth, and have a positive effect on trophic processes.
Let's look at some effective exercises:
- to correct a deep bite: stand straight with your chin raised as much as possible. Move the lower jaw forward, then return to its original position. Repeat 15 – 17 times;
- to correct open occlusion: take a pencil (you can put a rubber tube on it), squeeze it with your teeth with adequate force. Perform for 4 – 5 minutes;
- with a crossbite: open your mouth as wide as possible, move your jaw towards the defect, close your jaws in the correct position for 5 seconds, then relax, then repeat the exercise again;
- to correct mesial occlusion: use your tongue to press on the inside of the front part of the upper dentition. Perform the exercise for 5 minutes.
Important: when performing any exercises of the myogymnastics complex there should be no pain. After each approach, you need to let the muscles relax for 1 minute.
What is
The described pathology is also called prognathia. This is a type of improper closure of teeth that occurs due to overdevelopment of the upper jaw and/or underdevelopment of the lower jaw. In people with a distal bite, the upper teeth often overlap the lower teeth, so the chin looks disproportionately small.
Orthodontists determine the severity of the problem by the location of the sixth upper tooth. If it is in close contact with the opposing unit, then the curvature is minor. If, when the jaws close, the molar ends up in the area between the fifth and sixth teeth, then complex and lengthy orthodontic treatment awaits.
Records
Vestibular plates are removable orthodontic devices. This means that they can be removed for a while, for example, to eat or brush your teeth. The plate for correcting pathologies is made individually for each patient using personal casts of the jaws.
The base of the plate is a plastic base that is adjacent to the palate. Arcs, clasps and screws are integrated into it. The base color can be neutral or colored.
These devices are mainly used in childhood and adolescence, when the dental system is not yet fully formed and therefore the dental elements are able to move relatively easily under the influence of directed force. The plates are also used to correct pathologies in adult patients, but only in mild cases.
Is it advisable to straighten crooked teeth at home?
Teeth straightening occurs under the influence of aligners or braces. It is impossible to achieve the same result using the efforts of the tongue, or the influence of a finger, as well as various objects. The pressure of the devices occurs evenly, on the necessary points, for movement in the desired direction.
The trajectory was verified on a computer using three-dimensional models. There is no such equipment at home, and a non-specialist will not be able to correctly place the points of influence. And on your own - by placing your finger or tongue on a crooked tooth in order to move it - you will not get any results.
Trainers
Orthodontic trainers are removable silicone covers for the teeth. They are worn for several hours a day: at night and for 2–4 hours during the day. They are used to correct occlusion in children and in simple situations (for example, when there are gaps between dental elements) in adults.
There are several types of trainers:
- standard for the initial stage of treatment - made of soft pink silicone. This period lasts about six months. The main goal is to influence the position of the jaws and facial muscles;
- standard for the final stage - made from harder blue silicone. They directly influence the movement of teeth in the dental row;
- Lm-activators are trainers, the unique feature of which is that they can be used before all teeth erupt, when the process is just beginning. Their use allows the teeth to settle into place immediately after eruption;
- myobraises – allow for early correction in a natural way, from the age of 3 years. The system does not work on the consequence, but on the causes of the formation of malocclusion. Myobraises are worn for 1 hour during the day and worn throughout the night.
Methods of therapy for correcting bite
Correcting a bite most often means exclusively wearing braces. Indeed, they are often used (and not only for children), but other methods are also used in orthodontics. They can be divided into two groups - surgical and non-surgical.
Surgical methods
Surgical intervention is necessary in three cases:
- when there is high crowding, when it is necessary to remove quarter premolars to make room for other teeth;
- with serious jaw abnormalities;
- to speed up treatment.
Severe pathologies of the jaw bones, which lead to malocclusion and disturbances in swallowing and breathing, cannot be corrected without surgery. During the operation, the surgeon cuts the bone tissue in the places where the teeth need to be moved. At this time, the patient is under general anesthesia in the inpatient department. Rehabilitation after surgery takes up to three weeks. After the tissues are restored, the jaw will have to be developed. Most often, additional treatment is required: the doctor prescribes braces, which must be worn for at least six months. The type of braces, duration of wearing them, and location depend on the current state of the bite.
Surgery can also be used to shorten the treatment time for malocclusion. Orthodontists use what is called a corticotomy, a small operation performed after braces are installed.
About a week after installation, the patient comes to the periodontist, who uses a piezotome to make small incisions in the gums. The entire operation takes about 30 minutes and is performed under local anesthesia. Occasionally, sedatives are also used - general anesthesia is usually not needed.
After corticotomy, the patient will have to visit the orthodontist and periodontist several more times to remove sutures, monitor the condition of the gums and correct the braces. The operation significantly speeds up treatment – by 3–6 months.
Important: surgical intervention is prescribed only in adulthood, after the jaw is fully formed (usually after 16 years). There are a number of standard contraindications: HIV, cancer, heart disease, etc.
Treatment without surgery
If we are not talking about serious pathologies of the jaw, orthodontists and their patients do without surgical treatment methods. Correction of the bite occurs through the installation and long-term wearing of braces, mouthguards and other devices.
Braces are the most effective way to eliminate pathology. They are a power arch with brackets that are secured to the teeth. The arch provides constant pressure on the teeth, and they gradually move, taking the right place.
Braces are worn without interruption. They are removed only at an appointment with the orthodontist, during correction. Over the entire period of treatment (which ranges from 6 months to 3 years), several visits to the doctor may be required. The procedure and duration of treatment depend on the condition of the teeth and the chosen braces system. Thus, self-ligating ones do not require too frequent visits to the orthodontist.
In addition to braces, there are other methods of therapy. Thus, mouthguards are often used - removable devices made of transparent material, and if we are talking about three, microprosthetics (veneers) are chosen.
Mouth guards
Mouthguards, or aligners, are removable plastic or silicone transparent covers on the teeth. Made individually for a specific patient. They are worn constantly and are removed only for eating and hygiene procedures.
They are practically invisible, so they do not cause moral discomfort. The therapeutic effect is determined by a soft force effect on the dental elements, causing them to move in a given direction. The main disadvantage is the inability to eliminate particularly complex defects.
Important: the effectiveness of mouth guards for correcting malocclusion depends not only on the severity of the clinical case, but also on strict self-discipline. Failure to comply with the orthodontist's instructions will negate all efforts made.
Dental alternative - selection of aligners
If you decide to entrust your smile to professionals, remember: it is the patients who decide to resort to the help of orthodontists and get aligners that manage to get the coveted beautiful smile and eliminate bite defects at home.
In this case, there is no need to perform complex manipulations or exercises: it is enough to select aligners under the supervision of a doctor and follow the recommendations of a specialist, and the aligners will do the rest themselves!
Signs
You can understand that your bite needs to be corrected by the following symptoms:
The upper incisors protrude relative to the lower ones. Sometimes they stick out so much that there is no contact between the opposite units located in the smile zone (then doctors talk about the presence of a sagittal fissure).- Beveled bird profile. If you draw an imaginary line from the tip of the patient's nose to his chin, then the lips will not touch it. This profile is called “beveled bird profile”. With it, the lips seem to fall inward and seem very thin. If it is present, overweight people always have a pronounced double chin.
- Reduced height of the lower third of the face. The area from the base of the nose to the end of the jawline looks very small.
- Protruding upper row and lip. Looks like an aesthetic defect. Noticeably spoils the appearance.
- The presence of a deep chin fold. In this case, the lower lip seems to tuck under the incisors of the upper row.
Dentists can easily determine the presence of distal occlusion. All that is required of the patient is to consult a doctor in a timely manner so that he can prescribe effective treatment. The sooner orthodontic therapy is performed, the better.