Alveoloplasty methods
Correction of the alveolar process
It is used before the start of rational prosthetics, for the convenience of the patient while wearing a removable denture.
Relocation of the inferior alveolar nerve
The operation is performed when there is not enough space to place an implant; this situation often occurs in the lower jaw.
Graft transplant
Transplantation - increasing the volume of the mucous membrane or bone tissue. The need for this method arises after the removal of teeth or anatomical features of the body in order to comply with the conditions for implantation.
Gingivosteoplasty
This method is used for periodontal diseases with varying degrees of severity. Gingivosteoplasty is intended to correct gum recession.
Structure
The anatomical structure of the crest includes the base of the process with alveoli, separated by septa. This is where teeth develop and grow. The ridge consists of two walls - the outer one on the side of the cheek and the inner one, turned towards the tongue. The surface is lamellar, it is adapted to support row units of different types, differing in structure and loads.
The process of the maxilla is located between the plates, it acts as an integral part of the cancellous bone. Between the individual alveoli of the structure there are partitions that separate the tooth sockets. At the same time, the cells of the area constantly take part in the formation and resorption of bone, this process is compensatory, in this case it proceeds normally. The features of the ridge allow it to adapt to different conditions, which makes the functioning of the dentition correct.
The crest of the lower jaw has an unpaired and symmetrical structure. Externally, the site forms an arc with a main center and two branches. Alveolar axons are located on each side in an amount of 8 pieces. The sockets can have different shapes and sizes, depending on the position of the units, but most often they are cone-shaped alveoli. For areas where teeth with multiple roots develop, there are partitions that separate the canals.
Diagnostics
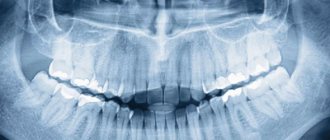
The fracture is diagnosed by an oral and maxillofacial surgeon. An x-ray may show different degrees of damage:
- partial damage - damage to part of the bone, not complete detachment;
- non-displaced fracture – damage to all parts of the bone;
- complete fracture - the x-ray shows a gap between the separated part and the skull;
- fracture in different places - damage to the alveolar process in different places, bone fragmentation;
- fracture with deformation - a completely torn off part, displaced at a different angle.
Advantages of the method
The horizontal augmentation method allows you to obtain the optimal bone thickness for implantation of a metal implant. It is considered low-traumatic compared to other types of bone grafting, since it does not require the collection of donor material.
This method allows you to:
- achieve rapid restoration of bone tissue width;
- effectively eliminate atrophy and other jaw defects;
- grow tissue with a density suitable for forming a bed for the implant;
- accelerate the implantation of the titanium rod into the jaw.
Restoration of dental-alveolar defects: a multidisciplinary approach
Correction of alveolar ridge defects is a complex clinical task from a functional and aesthetic point of view, which dentists have to solve at the stage of preparation for the dental implantation procedure. The bone crest of the jaw performs two important functions for a dental implant: biological - by essentially providing a “shelter” for intraosseous support, and aesthetic - by supporting the architecture of the peri-implant soft tissues.
Furhauser et al developed a special pink aesthetics score that measures the success of the aesthetic component of treatment using single intraosseous supports. High rates of pink aesthetics are achieved due to the complete immersion of the implant into the structure of the bone ridge, while maintaining (or restoring) the proper contours of the gingival papillae and the entire gingival profile. Gingival parameters that have been recorded around completely intact teeth are used as initial criteria during the development of the pink esthetics parameter. With an adequate approach to the restoration of residual ridge defects, the doctor is also able to provide a more natural contour of the soft tissues in the peri-implant area, thus maximizing the overall success rate of the treatment.
Defects in the area of the bone structure of the jaws arise either due to the inability of bone tissue to regenerate normally, or as a result of progressive destruction. The inability to adequately form the bone structure is associated with two main factors: the congenital absence of teeth in a certain area of the alveolar ridge, which limits the conditions for the growth of alveolar bone tissue in principle, and the phenomenon of tooth ankylosis, which, in turn, stops the possibility of further growth of bone tissue. Destruction of the alveolar bone can develop due to infection of the intervention site, trauma or tooth loss. Infection of bone tissue can be caused by a tooth root fracture, errors during endodontic treatment, or pathologies of periodontitis or peri-implantitis.
If the size of the bone defect reaches critical values, such lesions are not amenable to spontaneous regeneration and require additional interventions. In such cases, they speak about the limited potential of ridge regeneration, and the need to implement hard tissue augmentation approaches. The problem is that the doctor, with large ridge defects, has to restore the contour of the ridge almost anew, taking into account all the necessary vertical and horizontal parameters. The predictability of bone augmentation procedures depends on the fact that a number of biological principles are implemented: wound closure under primary intention, ensuring sufficient blood supply, maintaining the required volume of space, and the stability of the regeneration process. A sufficient level of blood supply to the intervention area ensures the supply of necessary cells, growth factors and other agents that induce a cascade of osteogenic biomineralization. Osteocytes enter the wound area, differentiating from bone marrow stromal cells, as well as from progenitor cells that circulate in the blood. During angiogenesis, a new blood network of capillaries begins to form in the structure of the bone defect, which grow directly from the walls of the defect. The bone graft used during manipulation allows one to retain the required amount of space, initiates the process of tissue resorption during remodeling, and is a chemical attractant for angiogenesis. The success of bone augmentation depends on ensuring a closed state of the space under which tissue regeneration takes place, and the level of tissue vascularization in the area of intervention.
Restoration of horizontal bone defects is more predictable, since in such cases there are walls that limit the defect, from the structure of which capillary ingrowth will occur. When reconstructing vertical defects in the bone tissue of the jaws, the situation is somewhat different: the longer the distance over which the capillaries need to migrate, the more difficult it is to achieve complete vascularization of the bone defect (photo 1).
Photo 1. In the blood and bone marrow there are so-called differentiation clusters - CD34+ stem cells, which are capable of differentiating into osteoblasts and endothelial cells. These cells migrate to the affected area and initiate the process of its restoration by triggering a cascade process of formation of new bone tissue and blood vessels. In addition, CD34+ cells release vascular endothelial growth factor (VEGF).
Distraction osteogenesis is a modification of the guided bone regeneration (GBR) procedure and has demonstrated successful results in the restoration of complex bone crest defects. In fact, the movement of teeth during orthodontic treatment is also a variant of distraction osteogenesis. This procedure is also used during periodontal-orthodontic rehabilitation of patients in order to reduce the size of intraosseous defects around problem teeth. The use of distraction osteogenesis allows the clinician to reduce the initial size of the bone tissue defect, which subsequently simplifies the bone augmentation procedure. After all, the rule is the same for everyone: the smaller the bone defect, the easier it is to restore it. In the clinical case described below, we illustrate the concept of using orthodontic techniques during targeted correction of the area of future implantation.
Clinical case
A 28-year-old patient sought dental care with a complaint about implant mobility in the area of the 22nd tooth (photo 2-3). In the area of the 23rd tooth, the patient had congenital adentia. The 22nd tooth erupted in place 23, leaving free space in the area of the natural position 22, where the procedure for installing a dental implant was previously carried out. The implantation took place in December 2002. In February 2005, the patient went to the dentist with signs of implant mobility and symptoms of peri-implantitis. X-ray diagnostic data confirmed the destruction of the residual ridge area around the installed intraosseous support. During the treatment, the problematic implant was removed, and careful curettage was performed in the area of the formed defect (photo 4-5). During the healing process of the problem area, a defect in the jaw bone tissue was formed with loss of the level of clinical attachment in the projection of the distal surface of the 22nd tooth and the medial surface of the 21st tooth (photo 6-7). Thus, the bone loss in this clinical case was caused by both congenital adentia and the inflammatory effect of peri-implantitis. Considering the amount of bone loss in the area of teeth 21 and 22 adjacent to the defect, it was proposed to remove them and ensure adequate formation of the bone contour for the subsequent implantation procedure. This intervention required a massive guided bone regeneration procedure, for which bone graft could be harvested from the chin area. After 6 months, the edentulous area could be restored with a bridge or single crowns on implants.
Photo 2. Front view of the affected implant in the area of the 22nd tooth.
Photo 3. X-ray of the affected implant in the area of the 22nd tooth before treatment.
Photo 4. Vertical defect of the bone tissue of the ridge in the area of the 22nd tooth.
Photo 5. Horizontal defect of the bone tissue of the ridge in the area of the 22nd tooth.
Photo 6. View of the bone and soft tissue defect after removal of the implant.
Photo 7. X-ray of the defect area in the area of the 22nd tooth.
However, at the same time, such an approach is characterized by the risk of developing significant biological and aesthetic complications. To restore adequate gum contour, it was necessary to raise the level of the underlying bone tissue, only in this way would it be possible to achieve the proper height of the interdental papillae. This was the main problem, because the predictability of vertical augmentation surgery is less than that of horizontal reconstruction of the bone crest. In the process of vertical augmentation of the jaw bone, an autogenous graft in the form of blocks is successfully used, but the level of its effectiveness is determined by a number of factors, including ensuring primary wound closure, minimizing the risk of secondary infection, creating conditions for stabilizing the graft, and leveling the possibility of developing paresthesia after surgery. From an aesthetic point of view, the removal of two teeth and the placement of three implants means that it is quite difficult to achieve the proper height of the interdental papilla in the area between the three intraosseous structures. When using two implants, it is much easier to restore the proper papilla, however, in the area of the cantilever part of the prosthesis, it will be necessary to carry out certain periodontal intervention to correct the relationship of the prosthetic structure with the surrounding tissues. Thus, taking all of the above into account, the approach of natural tooth extraction and placement of three implants was categorized as excessively risky in terms of the potential for potential biological, aesthetic, biomechanical and occlusal complications.
Another possible treatment approach involved minimizing the length of the defect through orthodontic tooth movement. First we had to move the 22nd tooth into its proper position. In this way, it would be possible to limit the ridge defect to the volume of one tooth. After this, it was planned to carry out extrusion of 21 teeth (with further extraction), which would make it possible to “pull out” the level of the bone crest from the distal side of the defect. After this, 22 would need to be moved distally to the place of tooth 21, then forced orthodontic extrusion and subsequent extraction would also be carried out. Thus, it would be possible to reduce the size of the bone defect and form appropriate bone walls around it, from the area of which the process of angiogenesis would subsequently be ensured. The area of the defect at the site of tooth 21 could be restored using a mineralized lyophilized bone allograft and membrane. Orthodontic tooth movement, which, in essence, is a subtype of distraction osteogenesis, would allow the restoration of the proper vertical parameters of the height of the bone crest, eliminating the need for autogenous bone replacement material. In addition, correct positioning of the premolar during the orthodontic phase of treatment would allow the creation of a more harmonious occlusal scheme, ensuring the formation of an occlusal relationship protected by the premolars. Such a scheme ensures the normalization of the loads applied to the implant strictly along the axis of the intraosseous support.
After discussion, the second rehabilitation approach described above was chosen. Before the start of the orthodontic phase, soft tissue augmentation was performed in the area of teeth 21 and 22 to correct the mucogingival defect. For this purpose, a free gingival graft was used, which allowed the formation of the required thickness of attached and keratinized gums. Thus, we minimized the risk of developing loss of gingival coverage in the area of 21 and 22 teeth during their orthodontic movement (photo 8). The orthodontic phase of treatment was aimed at creating such a state of the bone ridge in the area of the 23rd tooth, which would be most suitable for the dental implantation procedure (photos 9-11). In addition, orthodontic correction made it possible to balance the patient's existing occlusal pattern. At the same time, in the area of individual teeth, their shape was corrected using composite restorations (photos 12-13).
Photo 8. View of sufficient volume of keratinized and attached tissue after soft tissue augmentation.
Photo 9. Orthodontic distraction osteogenesis to form a site for implantation in the area of the 23rd tooth.
Photo 10. Radiograph during orthodontic distraction osteogenesis.
Photo 11. X-ray after forming the area for implantation in the area of the 23rd tooth.
Photo 12. View of the formed occlusal relationship and canine route of insertion.
Photo 13. Bonding on teeth 7-9 after the orthodontic stage of treatment.
Photo 14. Registration of the presence of bone tissue in the interproximal areas of the 21st and 22nd teeth after orthodontic treatment.
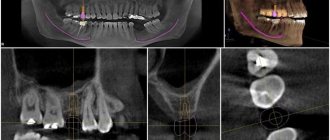
After moving the 22nd tooth to its proper position, periodontal status was monitored. At this point, the decision was made to discontinue continuous extrusion of teeth 21 and 22 because there was a distinct difference in the levels of clinical mucosal attachment around these teeth (Figure 14). Thanks to the use of computed tomography and wax modeling capabilities, it was possible to establish the most prosthetically favorable position of the future implant. The results of the CT scan confirmed that the level of bone tissue was sufficient for the installation of an intraosseous support (photo 15-16). To correct residual signs of the bone defect, it was necessary to perform only a minimal procedure of directed bone regeneration. The implant was installed after complete separation of the flap (photo 17). During the operation, dehiscence was noted in the area of the roots of teeth 21, 22, 24 and 25, as well as signs of bone dehiscence in the area of the natural position of tooth 23 (photo 18). After installation of the implant, the cortical plate was perforated to induce the process of angiogenesis (photo 18).
Photo 15. Planning of implant installation in the area of the 23rd tooth according to CT scan data. Bone dehiscence in the area of the 23rd tooth was restored.
Photo 16. Cross-sectional view of the area of the 23rd tooth prepared for the installation of a dental implant after orthodontic correction.
Figure 17. SurgiGuide surgical template (Materialize Dental, Leuven, Belgium) supported on teeth.
Photo 18. Installation of a dental implant. Perforation of the cortical plate to stimulate angiogenesis.
To cover the area of dehiscence, a mineralized lyophilized bone allograft treated with platelet-derived growth factor was used, which was placed into the structure of the defect and covered with a membrane (Figure 19). The flap was repositioned more coronally to ensure complete primary wound healing (Figures 20-21). 4 months after implantation, provisional structures were fixed to the implants and the soft tissue area was augmented using a connective tissue graft. To complete the orthodontic correction of the teeth position, implant structures were used as additional support. The goal of orthodontic treatment at this stage was to achieve the required position of individual teeth, normalize their occlusal relationship and form an optimal distance between their roots. At the final stage of treatment, zirconium abutments (photo 22) and all-ceramic structures (photos 23-25) were fixed to the implants.
Figure 19: Mineralized freeze-dried bone allograft hydrated with platelet-derived growth factor was used to cover the area of dehiscence.
Photo 20. Closure of the wound area by primary intention.
Photo 21. X-ray of the implant in the area of the 23rd tooth immediately after installation.
Photo 22. Fixation of the zirconium abutment on the implant.
Photo 23. X-ray after fixation of the zirconium abutment.
Photo 24. Final restoration in the area of the 23rd tooth.
Photo 25. View of the final restorations in the area of teeth 7-9 and 23.
This clinical case illustrates an example of the correction of a dentoalveolar defect resulting from bone crest destruction through the application of the principles of orthodontic, periodontal and restorative dental treatment. This approach made it possible to normalize the patient’s occlusal scheme, as well as to achieve proper restoration of the defect area with minimal consumption of bone replacement materials. Thus, it was also possible to simulate the necessary contour of the soft tissues, ensuring their natural aesthetics. The restoration of the coronal part was carried out using all-ceramic single restorations on zirconium abutments.
Authors: Brian S. Vence, DDS George A. Mandelaris, DDS, MS David P. Forbes, DDS, PhD
Possible pathologies and injuries
The most common problem encountered in dental practice is atrophy affecting the alveolar ridge. The reasons for this phenomenon:
- injuries, mechanical damage to the area;
- osteoporosis;
- lack of treatment in the form of prosthetics, if there are indications for this;
- fragility, weakening of the bone.
Before you begin installing the prosthesis, you need to correct the process. The bone thickens in the necessary places, the structure becomes reliable, durable, and able to withstand loads. The procedure for performing the operation depends on the condition of the tissues and the cause of the damage.
Most often, correction is needed as a result of damage to the appendix after injury. The most common ones include:
- fractures of the alveolar part;
- physiological aging, that is, natural processes;
- destruction of the ridge for various reasons.
This is not only impacts and other damage, but also a congenital weak bite, in which the tissues are subject to natural increased wear. If timely measures are not taken, there is a likely risk of tooth loss. Therefore, regular preventive examinations come first, especially in cases of bone fragility.