Preface
The goal of root canal therapy is to remove the contents of the root canal space and then fill it. Proper treatment requires knowledge of both the external and internal anatomy of the tooth to reduce the risk of failure and the possibility of iatrogenic biological damage.
Understanding the coronal morphology of the tooth allows us to make endodontic access in the most conservative manner; The shape of the access cavity is described for all teeth. Studying the morphology of the root canal system and its several variations makes it obvious why there are operational difficulties during instrumentation, as shown in the iconographic part. From the morphological and histological tables of Hess, the complexity of the entire root canal system is visible, which confirms the difficulty of completely removing pulp tissue from the endodontic space and encourages the search for new methods and technologies in endodontics.
The microscopic anatomy section summarizes the interaction of the root dentin wall structure with mechanical (files, ultrasound), chemical (irrigants) and physical (lasers) factors during therapy. In particular, in order to understand the different effects of lasers on tissue depending on the wavelength, it is very important to carefully study the ultrastructure and histology of dentin in the canal.
Anatomy of primary teeth
The macroscopic anatomy of primary teeth is very similar to that of permanent teeth, with some differences between them outlined in this section.
Ernst Zurcher (1922), Walter Hess school in Zurich, carried out the first scientific work on pulp morphology in primary teeth.
The endodontic morphology of primary teeth is very similar to the endodontic morphology of permanent teeth, but is smaller in size. Primary teeth are usually shorter and smaller than permanent teeth; the roots are narrow, while the roots of permanent teeth are thicker, especially in the cervical third. However, the width of the crowns of primary teeth is more pronounced compared to their height. The roots of temporary molars, in addition to being thinner than permanent roots, diverge to the sides to ensure the eruption of permanent premolars, first of all during their formation, and then during eruption.
Primary upper and lower molars often have a fourth canal in the mesiobuccal root of the upper molar and in the distal root of the lower molar.
As the child grows, the length of the roots of primary teeth decreases due to physiological resorption (exfoliation) (Fig. 1.1 and 1.2). Sometimes resorption of the floor of the pulp chamber at the furcation precedes apical root resorption (Fig. 1.3ad).
Rice. 1.1 Primary upper molar: root resorption starting in the apical region (arrows)
Rice. 1.2. Primary lower molar: root resorption affecting all parts of the root from apex to crown
Rice. 1.3. Primary upper molar: radicular resorption is more obvious at the floor of the pulp chamber in the area of the furcation, which in this case precedes apical resorption; (a) root apices are intact; (b) resorption in the area of the furcation of the pulp chamber; (c) palatal root resorption (arrows); (d) mesial view of furation resorption (arrows)
Unlike permanent teeth, the loss of primary teeth explains why canal filling at the end of endodontic treatment requires the use of resorbable materials that allow gradual root resorption.
At what age do they appear?
Statistics show that the beginning and completion of the change from temporary teeth to molars in most children occurs at approximately the same time. There are minimal differences only among children in different regions. The warmer the climate, the sooner the child will have permanent teeth.
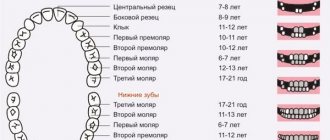
The table shows age parameters that can be used to determine the approximate beginning of the eruption of molars according to several well-known authors.
| Set of teeth | Period of eruption of permanent teeth in children (in years) | ||
| according to Vinogradova | according to Lukomsky | according to Novak | |
| Central incisors | 5-6 | 6-9 | 6-9 |
| Lateral incisors | 7-9 | 7-10 | 7-10 |
| Fangs | 12-13 | 9-14 | 9-14 |
| First premolars | 9-11 | 9-13 | 9-13 |
| Second premolars | 9-11 | 9-15 | 10-14 |
| First molars | 4,5-7 | 7-8 | 5-8 |
| Second molars | 12-13 | 10-15 | 10-14 |
| Third molars | 18-25 | 15-24 | 18-20 |
The differences in the age at which permanent teeth appear depending on the author are due to the fact that they present the results of studies in different regions that were carried out with a serious difference in time (several decades).
Permanent teeth
Macroscopic anatomy
Human permanent teeth consist of a crown and one or more roots. The endodontic space, created by the dentin of the root and pulp chamber, is very complex and is classified differently depending on the crown-root relationship and canal morphology.
Weine (1996) classified the root canal system into four types when considering the relationships between the pulp chamber, root canals and their apical termination (Fig. 1.4).
Rice. 1.4. Weine's classification of the root canal system takes into account the relationship between the pulp chamber, root canals and their apical termination.
Vertucci (1984) identified eight main types. Later, the Vertucci classification was expanded to include other morphological classifications by Gulabivala et al. (2001 and 2002) and Sert and Bayirili (2004) (Figures 1.5, 1.6 and 1.7).
Rice. 1.5 and 1.6 Graphic display of the morphological classification of Gulabivala endodontic system
Rice. 1.7 Graphic display of the morphological classification of Sert and Bayirili endodontic system
Schneider analyzed single-rooted human teeth and classified them according to the degree of root curvature as straight, with a curvature less than or equal to 5°, with a moderate curvature between 10° and 20°, and with a strong curvature between 25° and 70°. Lautrou [1987] also described and classified various morphologies of root cross sections (Fig. 1.8).
Rice. 1.8 Graphical representation of Lautrou classification of morphology in root cross sections
Zidell (1985) and Ingle and Taintor (1985), in addition to the degree of root and apical curvature, also considered the complexity of the anatomy, including the presence of bifurcations, the presence of accessory canals, and the presence of lateral and accessory canals.
Various studies and texts later described the anatomy and morphology of permanent human teeth and their countless possible shapes.
In paragraphs about a particular tooth, the age of eruption considered is according to Logan and Kronfeld, slightly modified by Schour and included in the text by Ash. The dimensions of human teeth described in this textbook are instead taken from various texts.
Mineralization of teeth and why is it needed?
Not only adults, but also children are currently faced with dental problems. In children, dental problems can arise from a lack of minerals and vitamins during fetal development, when the fetus is developing teeth. When teeth erupt, the period of primary mineralization of enamel begins. At this stage, the tooth enamel is still immature. As the tooth functions, minerals are transferred from saliva to the enamel. After 2-4 years, the optimal content of mineral substances is observed in it and its layer is compacted. The general mineralization of the tooth is constantly maintained due to the mineral composition of the oral fluid, that is, saliva. The most important function of which is mineralizing. Thanks to this function, the “enamel maturation” of erupted teeth occurs.
Enamel is the hardest and most mineralized component. It covers the outside of the tooth crown. Its thickness varies depending on the location on the crown and the shape of the tooth. It reaches its greatest thickness on the cutting edge of the anterior (frontal) and on the tubercles of chewing teeth (molars and premolars). In the area of fissures (recesses), the lateral surfaces of the tooth crown and in the area of the necks of teeth, the thickness of the enamel is much less.
Here we can see the connection between the thickness of the enamel and the areas of its demineralization. The hardness of enamel is due to its high content of mineral salts. The mineralization process is significantly influenced by the nature of nutrition, disorders of phosphorus-calcium metabolism (rickets), fluoride content in drinking water, and the general condition of the body.
The condition of permanent teeth can be influenced by diseases of the endocrine system, impaired digestion of food (with celiac disease, dysbacteriosis), diseases of the gastrointestinal tract, excessive consumption of sugars, insufficient oral care, lack or, conversely, excess of certain minerals, changes in the composition of saliva (its mineralizing capacity).
Saliva plays a vital role in maintaining the balance of the processes of mineralization and demineralization of tooth enamel. If the mineral composition of the enamel is disturbed, the resistance (stability) decreases and the risk of demineralization of the enamel increases.
One of the methods for correcting disorders is enamel remineralization. This procedure is carried out both for the purpose of prevention and for teeth that already have significant damage to the enamel. All means for remineralizing enamel can be divided into two groups. The first group includes products based on fluorine compounds. The second group includes products without fluoride, but containing hydroxyapatite particles or calcium compounds.
The remineralization procedure can be carried out both at home and after professional oral hygiene. Before carrying out remineralization therapy, it is important that the teeth are cleaned of any type of plaque. A qualified specialist must assess the condition of the dental tissues and decide which methods are indicated in each specific case. After professional oral hygiene, a specialist can use a highly effective polishing paste based on a high concentration of nanohydroxyapatite, and also prescribe it for home use, applied to the teeth after daily brushing, or used in mouth guards. For isolated areas of enamel demineralization, teeth are coated with varnish.
There are also complexes that contain an anhydrous fluorine compound and a highly dispersed calcium compound, which ensures deep penetration of particles with the formation of submicroscopic crystals of calcium fluoride, which provide long-term protection for 1 year.
During enamel treatment, deep penetration of substance ions into micropores occurs, due to which remineralization occurs. The procedure of deep mineralization is relevant if the active development of caries begins, as well as for the mineralization of “immature enamel”.
It is important to strengthen a child’s enamel from the beginning of the eruption of baby teeth until the end of the formation of a permanent bite, until about 11-12 years of age. Remineralization is indicated after professional oral hygiene, after a whitening procedure, for demineralization of enamel (white spot), during and after orthodontic treatment, and increased sensitivity of enamel.
Preserving the integrity of enamel in childhood is the key to healthy teeth in the future.
Upper incisors
Central upper incisor
The central upper incisor erupts (one per quadrant) between the ages of six and seven years, and the complete formation of the apical third occurs after 2 or 3 years. The average tooth length is 22-23 mm.
The crown has a triangular shape, about 10.5 mm long, the base extends in the mesial-distal direction, corresponding to the anterior edge of the tooth, up to 9 mm in size, and its buccal-palatal size is 7 mm (Fig. 1.9).
Rice. 1.9 Upper central incisors: palatal view of the crown
The root is usually straight (75%), but according to Ingle, a slight curvature may be present in a small percentage of cases. Lateral canals may be present in more than 20% of cases, and an apical delta is also common (35%).
The coronal pulp space also has a triangular shape, especially in the region of the cervical radicular third, with the base facing the vestibular wall and the apex located palatally, after which it gradually becomes a round canal until the apex.
The access cavity is triangular and follows the shape of the pulp space (Fig. 1.10).
Rice. 1.10 Upper central incisor: graphical representation of the access cavity
Lateral upper incisor
The eruption of the upper lateral incisor (one in the quadrant) occurs 1 year after the central one, and its complete formation takes approximately 3 years.
It is approximately 1 or 2 mm shorter than the central incisor, its mesial-distal size is smaller - about 7 mm, and the vestibular-palatal size is only 5.5-6 mm (Fig. 1.11).
Rice. 1.11 Upper lateral incisor: palatal view of the crown
Normally there is only one root canal, straight in 30% of cases, and often it is curved distally (53%), in a small percentage of cases there is curvature in other directions. The shape of the canal is ovoid in the cervical region, with a tendency to become more rounded in the apical region; the access cavity has a similar structure (Fig. 1.12).
Rice. 1.12 Upper lateral incisor: graphical representation of the access cavity
Lower incisors
The lower incisors, two per quadrant, are very similar to each other, with some peculiarity retained.
Lower central incisors
The lower central incisors are the first permanent teeth to emerge in children's mouths, usually between 6 and 7 years of age, and are fully formed by 9 or 10 years of age. The lower central incisor is approximately 21.5 mm long. The apical third of the root is straight in 60% of cases and curves distally in 23% of cases.
The crown has a trapezoidal shape with a large base corresponding to the cutting edge and a smaller base that continues into the cervical third of the root. Its mesio-distal size is 5.5 mm at the greatest width of the incisal edge and gradually decreases to 3 mm at the cervical level (Fig. 1.13).
Rice. 1.13 Lower incisors: lingual view of crowns
The lower central incisor has a buccal inclination. In the root, it is possible to have a second canal located lingually in relation to the main canal in 18-23% of cases (Fig. 1.14).
Fig 1.14 Lower central incisor: graphical representation of the access cavity
Lower lateral incisor
The lower lateral incisor is similar to the central incisor, but slightly larger - about 1 mm, usually erupts 1 year after the lower central incisor and completes its formation after 3 years.
Root examination confirms the presence of two canals in 15% of cases.
The access cavity of the lower incisors is formed in a buccal-lingual direction to search for a second canal located lingually (Fig. 1.15a-c).
Rice. 1.15 (a - c) Lower central incisor: buccal, lingual and proximal views
Teething sequence
Almost all parents believe that the first molars should be incisors, which replace temporary elements of the dentition. But this opinion is wrong. Even before baby teeth fall out, at the age of 5-6 years, children receive their first molars, which are not on the list of primary teeth.
After this, the sequence of formation of a permanent bite is almost no different from the order of eruption of primary teeth:
- the lower and upper central incisors grow;
- lateral incisors appear on both jaws;
- lower and upper first premolars;
- fangs;
- upper and lower second premolars;
- second and third molars (you must understand that the so-called “wisdom teeth” sometimes do not penetrate the surface of the gums at all).
Teeth cutting in this order does not happen just like that, because it ideally corresponds to the speed of development and formation of the maxillofacial system. If the optimal sequence is followed, correct bite development occurs.
Fangs
Upper canine
The upper canine, one per quadrant, erupts at approximately 11-12 years of age and completes its formation after 3-4 years.
This is the longest tooth in the arch (about 27 mm or more).
The crown has a diamond shape with a peculiar sharp cusp, which on the vestibular side divides the mesial and distal sides of the crown. The crown is 10 mm high (length) and has a maximum mesial-distal diameter of 7.5 mm at the point of proximal contact and decreases to 5.5 mm cervically. The buccal-palatal diameter is wider (8 mm), and it remains up to 7 mm at the cervical level due to the presence of a prominent marginal ridge (Fig. 1.16).
Rice. 1.16. Upper canine: palatal view
The long root, like the crown, is narrow in the mesial-distal direction and more pronounced in the buccal-palatal direction. There is almost always only one root canal with lateral canals at different levels in 24% of cases. The apical third is straight in 40% of cases, and is often curved distally (32%) and/or vestibularly (13%) (Fig. 1.17).
Rice. 1.17 Upper canine: graphical representation of the access cavity
The pulp space at the level of the cervical third and the root middle third has an oval shape in the buccal-palatal direction; often two canals are present with a tendency to merge into one common round canal in the apical third (Fig. 1.18a, b).
Rice. 1.18 (a, b) Upper canine: buccal and proximal view
The endodontic access cavity is oval-shaped, extending from the cusp to the marginal ridge of the coronal cervical third to gain access to the radicular space without obstruction that could cause instruments to create steps or transposition of the apical foramen (see Fig. 1.19).
Rice. 1.19. Anatomical pictures from Hess and Keller: the endodontic space of the upper canine at the level of the cervical third of the canal is represented by one oval canal, and in the middle third it is divided into two different canals and often merges into one round canal in the apical third
Lower canine
The lower canine, one per quadrant, erupts approximately 8-10 months before the upper one and completes its formation after 3-4 years.
The crown has a length of 11 mm, and its mesiodistal diameter is narrower than the upper one (7 mm), and decreases to 5.5 mm at the cervical level. The maximum buccolingual diameter is 7.5 mm wide and decreases to a minimum at the cervical level. The cervical lingual marginal ridge is less pronounced than that of the upper canine (Fig. 1.20).
Rice. 1.20 Lower canine: lingual view of the crown
The lower canine is about 27 mm long, and has two separate roots in 6% of cases, or two canals in one root, connected by isthmuses, with a common or two separate apexes (Fig. 1.21). In 20% of cases, the apical third has a distal slope (Fig. 1.22).
Rice. 1.21 Lower canine: graphical representation of the access cavity
Rice. 1.22. Anatomical pictures from Hess and Keller: the endodontic space of the lower canine has two separate canals connected by an isthmus in the coronal third; the canals merge into one opening in the apical third
The endodontic space is oval in shape in the bucco-lingual direction for two-thirds of the root, and then gradually becomes rounded.
The endodontic access cavity should be oval in shape in a buccolingual direction, from the cusp to the marginal ridge (Fig. 1.23a, b).
Rice. 1.23 (a, b) Lower canine: buccal and proximal view
Upper premolars
Two per quadrant, premolars erupt between 10 and 12 years of age, and root formation is completed after 3 years. They replace temporary molars.
The first and second premolars have a similar crown but different morphology.
Upper first premolar
The first upper premolar erupts when the child is about 10-11 years old. It has a length of about 21-22 mm, and its buccal-palatal dimensions are 9 mm and mesial-distal dimensions are 7 mm. It has two cusps, buccal and palatine, which are slightly shorter (about 1 mm). The pulp space is determined by the shape and size of the outer crown (Fig. 1.24). In approximately 72% of cases, two roots with two different apical foramina are present (Fig. 1.25). Premolars may also have only one root with two canals (13%) (Fig. 1.26a, b), and in some cases three roots (6%) (Fig. 1.27). In addition, in 37% of cases we found a distal root bend in the apical third.
Rice. 1.24 First upper premolar: occlusal view
Rice. 1.25 Upper premolars: graphical representation of the access cavity; note the mesial position of the second premolar access cavity (right in the figure) to facilitate passage of the distally curved canal
Rice. 1.26 (a, b) Upper single-root premolar: buccal and proximal view
Rice. 1.27 Anatomical pictures from Hess and Keller: complex pulp space of an upper single-rooted premolar; two different channels have multiple messages along the root and two separate outputs
The access cavity to the pulp chamber should have an oval shape in the buccal-palatal direction, from one tubercle to another Fig. 1.28.
Rice. 1.28 Anatomical pictures from Hess and Keller: an upper premolar with three roots, two buccal and one longer palatal
Upper second premolar
The second upper premolar erupts between the ages of 10 and 12 years. It is very similar to the upper first premolar, both in size and crown shape. But there are some main differences between the roots, presented in three versions:
One root with one canal in 75% of cases (Fig. 1.29a, b)
Rice. 1.29 (a, b) Upper first premolar: mesial and distal view
One root with two canals and one or two separate apical foramina (12%) (Fig. 1.30 and 1.31)
Rice. 1.30. Anatomical pictures from Hess and Keller: an upper single-rooted premolar having two canals merging into one exit; lateral canals are also present in the apical and middle third of the canal
Rice. 1.31 Anatomical pictures from Hess and Keller: upper single-rooted premolars have two canals with separate exits, apical and lateral
Two separate roots and canals (12%)
Three separate roots (usually two of them buccal) with three canals (1%)
On the buccal side, the roots have a distal curvature in 27% of cases, and a vestibular curvature in 12% of cases, and in 20% of cases they have two sharp curvatures.
The endodontic access cavity to the pulp chamber has an oval shape in the buccal-palatal direction. If there is significant distal apical curvature, the approach should be moved closer to the mesial marginal ridge, maintaining an oval shape (Fig. 1.28).
Stabilization
This period is characterized by a complete stop of all processes of tissue formation and development. The crown and root reach the required shape, size and level of strength that allows them to perform their basic functions.
The period of stabilization of primary teeth lasts on average 2.5-3 years. At this time, it is important to ensure optimal chewing load on the bite, which will ensure the normal development of facial and other muscles, as well as periodontal tissues and jaw bones. If a child has caries or other diseases, it is during this period that treatment of temporary teeth will be most effective in terms of preserving them, preventing the spread of infection and ensuring normal conditions for changing the bite.
Lower premolars
Two in each quadrant, they erupt between 10 and 12 years of age, with full root formation after about 3 years. They replace primary molars. In contrast, the upper premolars are distinct from each other (Fig. 1.32).
Fig 1.32 Lower premolars: occlusal view
Lower first premolar
The lower premolar erupts sometimes several months before and sometimes after the lower canine and is the smallest of all premolars. The crown has two cusps, one very large and similar to the cusp of a canine tooth. The other is shorter by about 2 mm, similar to the lingual marginal ridge of the canine (Fig. 1.33).
Figure 1.33 Lower premolars: graphical representation of the access cavity
Length is about 21-22 mm, usually has one root with one canal (73-74%). Sometimes one root with two canals is possible (19%) (Fig. 1.34a, b), two roots with two canals (6%) (Fig. 1.35a, b) or three canals (1-2%).
Rice. 1.34 (a, b) First lower premolar: occlusal and proximal view
Rice. 1.35 (a, b) Second lower premolar: (a) coronal view; (b) Proximal view showing the presence of a single root
The root is often distally curved in 35% of cases and with a sharp curve in 7% of cases. The shape of the access cavity to the pulp chamber is oval, extending from the main tubercle to the tip of the minor lingual tubercle (Fig. 1.36).
Figure 1.36 Anatomical pictures from Hess and Keller: a mandibular premolar with a complex canal system that has two main canals connected by several fins and two separate exits
Lower second premolar
The second lower premolar erupts at the age of 11-12 years and is larger than the first premolar by 1 or 2 mm. The crown has two cusps (a larger buccal and a smaller lingual), but the lingual cusp is often divided into two parts (Fig. 1.37).
Rice. 1.37 Anatomical pictures from Hess and Keller: lower premolar with two roots and two canals; several short lateral canals present in the apical third
It has only one root with one canal in 85% of cases, but we can also find two separate canals in one root (11.5%) or two canals that merge into one apical foramen (1.5%) (Fig. 1.37 ). Rarely three channels are possible (0.5-1%). In approximately 40% of cases the root is straight, while in approximately 40% the apical third is distally curved. Severe curvature (7%) and vestibular curvature (10%) are possible.
The access cavity has an oval shape, also in the buccal-lingual direction, located in the center of the occlusal surface (Fig. 1.36).
Text of the book “Fundamentals of clinical dental morphology: a textbook”
As the enamel develops further, the enameloblasts decrease in size and move away from the dentin. Some enameloblasts die by apoptosis and are phagocytosed by neighboring cells. By the time teeth erupt, anameloblasts sharply decrease and are reduced, and the enamel is covered only with a thin shell - the secondary enamel cuticle, formed by cells of the outer enamel epithelium, collapsed pulp and an intermediate layer of the enamel organ, which covers the enamel and plays a protective role.
The process of enamel mineralization, starting in the area of the cutting edge and chewing tubercles of the teeth, then moves to other surfaces. The use of a new radiography method with primary direct image magnification [Belova N.A., 1981] showed that at 18–19 weeks of intrauterine development, signs of mineralization of the incisal edge and the surfaces of the incisor crowns by one third are clearly visible, as well as the beginning of calcification of the incisal edge of the canines and the vestibular medial cusp of the first molars.
At 24–25 weeks (6 months), mineralization of the incisors continues, the cutting edge of the canine is almost completely calcified, and points of calcification of the lingual medial tubercle of the first molars appear.
At 26 weeks (7 months), calcification of the incisors and canines continues, the vestibular cusps of the first molars have almost fused, and the first signs of mineralization of the apex of the distal vestibular cusp of the second molar are visible.
At 32 weeks (8 months), calcification of the incisors and canines continues; The vestibular cusps of the first molars merge.
At 36 weeks (9 months), all surfaces of the incisors are calcified (except for the cervical region), the vestibular cusps of the first molars are completely fused, the lingual cusps of the first molars are more clearly visible, and mineralization of the lingual distal cusp of the second molar is more intense.
After the birth of a child, the cervical area of the incisors becomes calcified; cervical region, vestibular and proximal surfaces of the canines, as well as the lingual surface of the first primary molar.
The final maturation of enamel (tertiary mineralization) occurs after tooth eruption, especially intensively during the first year of a child’s life. The main source of inorganic substances entering the enamel is saliva and, to some extent, dentin.
The study of the processes of development and calcification of enamel is not only of theoretical interest.
It is necessary for a correct understanding of the mechanism of development of a number of pathological processes that are observed in the enamel of developing or already completed teeth (enamel hypoplasia, caries). 6.2.3.
Development of the tooth root and cementum The development of the tooth root occurs already in the postnatal period, shortly before eruption. By that time, the crowns of baby teeth are mostly already formed. On top of the enamel layer of the tooth crown are the remains of the enamel organ in the form of an epithelial layer consisting of several rows of cells. This reduced enamel epithelium remains on the surface of the tooth crown until its eruption and, as some authors believe [48, 72], prevents the resorption of enamel from the connective tissue of the jaws or the deposition of cement on its surface.
These regressive changes in the enamel organ do not affect its edges, where the inner enamel cells merge into the outer enamel epithelium. The cells here actively proliferate, forming the epithelial (Hertwig) root sheath (vagina radicalis epithelialis), which plays an important role in the formation of tooth roots (Fig. 134). this vagina consists of inner and outer enamel organ cells closely adjacent to each other.
Rice. 134. Formation of the root of a growing tooth.
1 – epithelial root sheath; 2 – root dentin; 3 – root cement; 4 – dental pulp; 5 – epithelial diaphragm; 6 – epithelial bodies of Malasse; 7 – dental alveolus.
The inner enamel cells remain cubic in shape and do not develop into anameloblasts. The pulp of the enamel organ and its intermediate layer are absent. the epithelial vagina forms around the dental papilla, at its base, a kind of ring - the diaphragm (see Fig. 134, A) of the root sheath (diaphragma vaginae radicis), which gradually grows into the underlying ectomesenchyme, separating that part of it that will go to the formation of the tooth root .
The mesenchymal cells of the dental papilla, adjacent from the inside to the epithelial root sheath, turn into odontoblasts, which form root dentin (see Fig. 134, B). After the appearance of root dentin, the epithelial sheath grows with the cells of the dental sac, loses its continuity and is subsequently resorbed. Some vaginal cells may remain in the periodontium of an adult tooth in the form of residual epithelial Malasse bodies (see Fig. 134, B).
As a result of the disintegration of the epithelial root sheath, the ectomesenchymal cells of the dental sac come into direct contact with the root dentin, differentiating into cementoblasts, which begin to deposit cement on the surface of the root dentin.
The differentiation of ectomesenchymal cells of the dental follicle into active cementoblasts is accompanied by the development of granular endoplasmic reticulum, the Golgi complex, and a system of microbubbles and vesicles in the cells. First, cementoblasts synthesize internal collagen fibers of the extracellular matrix. The collagen released from the cells is further modified by specific non-collagen proteins, also derivatives of cementoblasts, into a form capable of calcification.
During cement mineralization, cementoblasts are constantly separated from the hardening front by a layer of non-calcified cement - cementoid, or precement. In addition to collagen, the cementum contains processes of cementoblasts. In some cases, cementoblasts are surrounded by their own excretory products, which harden, turning cementoblasts into cementocytes. The latter are an inactive form of dental follicle cells that lose organelles for protein synthesis and subsequently die, turning into scaly formations.
It is interesting to note that, unlike bone or dentin, the initial hardening of cementum does not depend on the activity of extracellular mineralized matrix vesicles, but occurs to some extent by the spread of hydroxyapatite from the dentin of the tooth root.
The rest of the dental sac, surrounding the developing tooth root, gives rise to the dense connective tissue of the pericement (periodontal). Bundles of collagen fibers of the pericementum with some of their ends are, as it were, soldered into the ground substance of the developing cement, and with the other ends they pass into the ground substance of the alveolar bone. As a result, the root is tightly strengthened in the dental alveolus.
In general, the formation of cement occurs according to the type of periosteal osteogenesis. The resulting cement is almost coarse-fibrous bone tissue in structure, covering the outside of the root dentin.
Exposure to unfavorable factors during cementogenesis can lead to hypercementosis (cement hyperplasia). The process can affect one or all teeth. Hypercementosis is also possible in certain areas of the root of one tooth.
In some cases, loose nodular thickenings of hardened cement form in the periodontal membrane. Such thickenings are known as cementicles. They are usually observed around degenerated epithelial remnants of Hertwig's vagina. With age, cementicles may adhere to the cementum, forming centers of localized excementosis.
After the formation of the root, the epithelial root sheath stops growing in depth, gradually closes in a ring shape and forms an opening at the apex of the tooth root, through which the vessels and nerves of the dental pulp pass. The initially wide apical opening of the root canal gradually narrows due to the deposition of new masses of dentin and cement.
Root development is more difficult in multi-rooted teeth. Depending on the type of tooth, the initially single and wide root canal of such teeth is divided into two or three canals. From the edges of the diaphragm of the epithelial root sheath, two (in the rudiments of the lower molars) or three (in the rudiments of the upper molars) epithelial outgrowths grow towards each other in a horizontal direction. The apices of these outgrowths eventually grow together and the initially single cervical opening is divided into two or three openings, according to the number of future roots. Their further development proceeds similarly to that of single-rooted teeth.
The growth of the roots of baby teeth and their subsequent resorption occur in a certain order. Thus, the roots of the central incisors and first molars develop during the first six months of a child’s life. Root growth continues until the age of 2–2.5 years, after which their gradual resorption occurs. The roots of the lateral incisors begin to develop during the first half of the year and grow until 2 years. Their resorption begins at the age of 5–6 years. The roots of the fangs develop in the period from 1 year to 3.5 years, and are resorbed in the 5th year.
The development of the roots of second molars occurs within 11.5 years.
By the age of 3, the roots are fully formed. Their resorption begins at the age of 5 years. 6.2.4.
Development of the pulp of primary teeth Simultaneously with the histogenetic processes of formation of dental tissues, differentiation of the mesenchymal elements of the dental papilla occurs in its central part.
Mesenchymal cells increase in size and begin to move away from each other due to the appearance of a basic amorphous substance between them. Gradually, the mesenchyme of the papilla is transformed into loose connective tissue, rich in fibroblasts, fibrocytes and macrophages, as well as blood vessels and nerves. By the time the tooth erupts, the mesenchyme of the papilla is almost completely differentiated into the pulp of the dental organ, although the final restructuring of the tissue elements of the pulp is completed in the first years of life. 6.2.5.
Eruption of baby teeth Eruption of a tooth is the process of its movement from its origin and development within the jaw until a crown appears in the oral cavity. This tooth movement is a complex, multifunctional stage in tooth development, as it is accompanied by coordinated changes in the growth of teeth, alveolar processes and the jaws themselves. During the period of eruption, developing teeth make movements in various directions, among which the following can be distinguished:
– vertical (axial) movement in the direction of the long axis of the tooth;
– movement in the distal, mesial, lingual or vestibular direction (change in position in the jaw);
– wedging (lateral movement);
– rotation – movement around the longitudinal axis of the tooth.
All these movements make it possible to maintain constant the relationship of the tooth germs to the edge of the developing alveolar process of the jaw, which is a necessary condition for the successful completion of tooth eruption. During eruption, the tooth makes a significant journey in the jaw, during which the following are observed:
– changes in the tissues surrounding the tooth;
– tooth root development;
– restructuring of the alveolar bone;
– development and restructuring of the periodontium.
In the connective tissue of the gums, which lies in the path of movement of the erupting tooth, regressive changes occur due to the pressure of the tooth on the tissue. These changes cause ischemia (malnutrition) and subsequent tissue atrophy and resorption. The reduced enamel epithelium covering the tooth crown (formed by the outer and intermediate layers of the enamel organ, as well as enameloblasts that have completed the production of enamel) secretes enzymes that also contribute to the destruction of the connective tissue separating it from the epithelium of the oral cavity. Approaching the epithelium lining the oral cavity, the enamel epithelium proliferates and subsequently merges with it. The epithelium of the oral cavity above the crown of the tooth degenerates and through the resulting hole the crown erupts into the oral cavity, while there is no bleeding, since the crown moves through the canal lined with epithelium (Fig. 135).
Having penetrated the oral cavity, the crown continues to erupt until it takes its final position in the chewing plane, meeting the crown of its antagonist.
The reduced enamel epithelium remains attached to the enamel of the unerupted portion of the crown, where it is called the primary attachment epithelium. It is subsequently replaced by secondary attachment epithelium, which is part of the gingival epithelium.
Rice. 135. Eruption of baby teeth.
1 – epithelium of the oral cavity; 2 – tooth cuticle; 3 – erupting tooth; 4 – gingival epithelium; 5 – dental alveolus.
Regressive changes in the connective tissue surrounding the erupting tooth occur simultaneously with the intensive development of its root due to odontoblasts producing dentin and ectomesenchymal cells of the dental sac, differentiating into cementoblasts that deposit cement on top of the root dentin. At the same time, growth of periodontal fibers and restructuring of the alveolar bone are observed. Intense deposition of bone tissue in some areas is combined with its active resorption in others. The severity of these changes varies throughout the entire period of eruption and is not the same in different teeth.
Deposition of bone tissue occurs, as a rule, in those areas of the bone socket from which the tooth is displaced, and in the areas towards which the tooth migrates, resorption is observed. Resorption of bone tissue makes room for the growing tooth, reducing resistance to its movement. Bone deposition usually manifests itself as the formation of bony trabeculae separated by wide spaces.
In the incisors, areas of increased deposition of bone beams are the bottom and lingual surface of the alveoli, which indicates a displacement of these teeth towards the lips during eruption.
Bone tissue in premolars and molars is deposited on the bottom and distal walls of the dental cell, which indicates their additional medial displacement during axial movement during eruption.
In multi-rooted teeth, the deposition of bone beams occurs most intensively in the area of the future interradicular septum.
The main periods of laying, formation and eruption of milk teeth are reflected in the table. 3.
Table 3
Timing of formation, formation and eruption of baby teeth in humans
Note:
i/w – period of intrauterine life.
6.2.6.
Development and eruption of permanent teeth The development of permanent teeth occurs in the same way as the development of primary teeth, but more slowly (Table 4).
Table 4
Timing of the formation, formation and eruption of permanent teeth in humans
Note:
i/w – period of intrauterine life.
The source of their formation is the same dental plate from which the rudiments of milk teeth developed. Starting from the 57th month of prenatal development, along the free edge of the dental plate (some scientists propose to call these sections of the dental plate the replacement dental plate), behind each baby tooth germ, on the lingual side, the enamel organs of the anterior permanent teeth are formed: incisors, canines and premolars. Since there are no premolars in the child’s primary dentition, the primary molars are subsequently replaced by permanent premolars.
In the prenatal period, the rudiments of the incisors (6-7th month) and canines (7-7.5 months), and then the premolars (7.5 months), are formed first from the group of anterior permanent teeth in the prenatal period. As a result, 10 rudiments of replacement permanent teeth appear in each jaw of the embryo.
Initially, the rudiments of these teeth lie in the bone alveoli common with the rudiments of milk teeth, but then a bone septum grows between them and a gradual separation of the cells of milk and permanent teeth occurs.
At the same time, the dental plate continues to grow posteriorly in each jaw and along its edge the enamel organs of large molars are formed (it is believed that these teeth should also be embryologically classified as the generation of milk teeth, rather than permanent teeth).
The earliest appearance of the first molar rudiment is in the 56th month of intrauterine life. The formation of the remaining molars occurs after birth: the rudiment of the second molar appears in the 5-6th month of a child’s life, and the rudiment of the third molar - in the 5-6th year of life, which is probably associated with the growth and elongation of the jaws. As they grow, the dental plates lengthen and grow posteriorly, the ends of which are displaced in the lower jaw into its branch, and in the upper jaw into the maxillary tubercle. This is where the enamel organs of the second and third permanent molars are formed. Only after this the dental plate gradually resorbs and disappears.
The very development of permanent teeth and differentiation of dental tissues occur in the same way as milk teeth. Ectomesenchyme grows into the enamel organs of permanent teeth from below and a dental papilla is formed. In the circumference of the germ of permanent teeth, a dental sac is formed from the ectomesenchyme and the further development of permanent teeth proceeds in the same way as milk teeth. The difference lies only in the time of passage of individual stages and the longer development of permanent teeth (about 10 years), especially large molars. Thus, during the period when milk teeth go through the last stages of their development, the jaws already contain the laying of permanent teeth that are at earlier stages. Therefore, in a child aged 3 to 6–7 years, an X-ray examination can reveal from 48 to 52 teeth in both jaws, of which 20 (baby teeth) perform their function, and the rest are still at various stages of development.
Calcification of the rudiments of permanent teeth is not observed before birth, with the exception of the first molar. A point of calcification in one of the cusps of the crown of this tooth appears on
9th month of intrauterine life. Complete crown formation occurs by two years. Calcification of the incisors begins in a child by 3–4 months. Complete crown formation occurs in the central incisors at 2–2.5 years, and in the lateral incisors by 3 years. Fangs begin to calcify at 4–5 months of age, and crown formation ends at 4–4.5 years. The process of mineralization of small molars begins at the end of the 2nd – beginning of the 3rd year of a child’s life and ends by 6–7 years. The beginning of calcification of the second molars dates back to 45 years. The third permanent molars calcify by 1315.
The formation of the roots of the medial incisors begins at the age of 3–3.5 years, the lateral incisors at the age of 4–4.5 years, the canines at the age of 5.5–6 years, and the first molar at the age of 4–6 years. The roots of the medial incisors reach full development at the 9-10th year, the lateral ones - at
10–11 years, canines by 12–15 years; premolars - by 12-14 years, first molars - at 9-10 years, second - at the age of 14-16 years, third molar - from 18 to 25 years.
At the age of 6–8 years, permanent teeth begin to erupt. The first large molar erupts first, then the medial and lateral incisors appear, then (from 9 to 14 years) the premolars and canines, as well as the second molar and the third molar later (at the age of 18–25 years, sometimes later).
The process of eruption of permanent replacement teeth is accompanied by the loss of milk teeth. During this period, resorption occurs first of the dental alveoli, and subsequently of the roots of the teeth (Fig. 136).
Rice. 136. Development and eruption of primary and permanent teeth.
1 – primary incisor; 2 – gums; 3 – rudiment of the permanent incisor; 4 – bone alveolus.
As the permanent tooth begins its vertical movement in the jaw, it puts increasing pressure on the alveolar bone surrounding the primary tooth. In the connective tissue separating the alveolus of a baby tooth from the crown of a permanent tooth, giant multinucleated cells—osteoclasts—differentiate, which actively resorb bone tissue.
After the destruction of the alveoli in the process of ongoing vertical movement, the permanent tooth begins to exert pressure now on the root of the baby tooth. Around the latter, osteoclasts (odontoclasts) also differentiate from the connective tissue, which actively resorb the tissues of the baby tooth.
Odontoclasts are located on the surface of the tooth root in wide lacunae. They are large in size, with numerous outgrowths of the cytoplasm on the side facing the root, containing a large number of lysosomes and mitochondria.
The destruction of primary tooth root tissues (dentin and cementum) by odontoclasts includes their demineralization, phagocytosis of areas and their intracellular digestion. The localization of the initial sites of root resorption depends on the location of the anlage of the replacement teeth: in primary incisors and canines it begins in the apical region on the lingual side, in primary molars - on the interradicular surface. Cells of the pulp of the baby tooth also participate in this process, from which odontoclasts also differentiate, destroying predentin and dentin from the pulp side of the tooth.
The process of resorption of the roots of baby teeth begins long before the eruption of the corresponding permanent teeth and proceeds very slowly and in waves: periods of increased resorption are followed by periods of rest. During the latter period, cementoblasts or fibroblasts appear in the tissues, the activity of which leads to the partial development of reparative processes - the deposition of cement or bone-like tissue on the surface of destroyed dentin.
The amount of resorbed tissue is usually greater than that of newly formed tissue. Therefore, the process of destruction of the baby tooth progresses, which ultimately leads to the loss of connection between the tooth and the alveolar wall and the empty crown being pushed into the oral cavity. This crown usually falls out under the influence of a growing permanent tooth, chewing forces, or a slight mechanical impact on it.
Loss of primary teeth typically occurs symmetrically on the right and left sides of each jaw, and occurs faster in girls than in boys. With the exception of second molars, primary teeth in the lower jaw fall out earlier than the corresponding teeth in the upper jaw.
The eruption mechanism is generally similar in permanent and baby teeth. According to a number of authors, the eruption of permanent replacement teeth is facilitated by the presence of a special anatomical structure - a conductive channel, or cord. The anlage of such a permanent tooth is initially located, as noted, in the common bone alveolus with the milk tooth. Subsequently, it is completely surrounded by alveolar bone, with the exception of a small narrow canal containing the remains of the dental plate and connective tissue. Together, these structures are called the conductive cord, which contributes to the directional movement of the permanent tooth during its eruption.
The eruption of additional permanent teeth (large molars) is not accompanied by destruction of the roots of milk teeth, since they do not have predecessors, but occurs in the same way as ordinary milk teeth.
The first permanent teeth to erupt are the first molars, usually on the lower jaw first; behind them are the medial incisors, lateral incisors, first premolars, second premolars and canines, second molars and finally third molars (wisdom teeth).
Full development of the roots of these teeth is completed within 2–3 years after eruption. Thus, the process of replacing baby teeth with permanent ones lasts for 14–17 years. Therefore, at approximately 5–6 years of age (from 6 to 12 years), a mixed set of teeth is observed in the child’s jaws.
The views on the explanation of the biomechanics of teething by various authors are ambiguous. There are a number of theories of teething: the theory of tooth root growth, the theory of increasing hydrostatic pressure in the dental pulp and in the periapical region, the theory of bone tissue remodeling, the theory of periodontal traction, etc. [5].
According to the root growth theory,
the process of eruption is the result of the tooth being “pushed” out of the alveolus by the growing root. From the perspective of this theory, the eruption of a tooth with an unformed root, the complexity of the trajectory of the tooth before eruption begins, as well as the lack of resorption of the bone tissue of the dental alveolus, which opposes the root apex, are inexplicable.
The theory of increasing hydrostatic pressure in the dental pulp and in the root apex area
involves the participation in the mechanisms of tooth eruption in the process of increasing the volume of the pulp in the direction of eruption, as well as increasing blood supply and vascular permeability in the area of the root apex.
According to the theory of bone tissue remodeling
The direction of tooth movement during eruption is determined by the direction of bone tissue growth in the area of the bottom of the dental alveoli and its resorption from the opposite side. From the standpoint of this theory, it is difficult to exclude the transformation of bone tissue as a consequence of tooth eruption itself.
Periodontal traction theory
provides for the dependence of the eruption process primarily on the formation of periodontium, the development of which is accompanied by a stop in tooth eruption.
Apparently, each of the existing theories of tooth eruption reflects one of the aspects of this complex process.
Upper molars
Three molars in a quadrant without corresponding primary teeth.
Upper first molar
It erupts between 6 and 7 years behind the second primary molar. The formation of the apex is completed between the ages of 9 and 10 years.
The crown has four cusps on the occlusal surface and three roots, one palatal and two vestibular (Fig. 1.38).
Rice. 1.38 First upper molar: occlusal view
The length of the tooth is about 21-22 mm and there is one canal in the palatal and disto-buccal roots
The mesiobuccal root has two separate canals in 60-70% of cases (MB1 and MB2). The second canal in the distobuccal root (DB2) is quite rare (2-3%) (Figs. 1.39, 1.40 and 1.41).
The access cavity to the pulp chamber has a triangular shape with the base facing the buccal side and the apex facing the mesial-palatal tubercle; the cavity is always located mesial (in front) of the transverse ridge, which unites the mesiopalatine tubercle with the distal buccal tubercle. The mouths of the canals are located at the vertices of the triangle, which form the access cavity (Fig. 1.42); if we combine the orifice of the MB1 canal with the palatal orifice, we can find a second mesiobuccal root canal (MB2), which is often closed by calcification (Fig. 1.43).
Rice. 1.39 Anatomical pictures from Hess and Keller: the upper molar has a very complex canal anatomy
Rice. 1.40 Anatomical pictures from Hess and Keller: the upper molar has a very complex canal anatomy; MB1 and MB2 visible in the mesiobuccal root
Rice. 1.41 Anatomical pictures from Hess and Keller: the upper molar has a very complex canal anatomy; MB1 and MB2 visible in the mesiobuccal root
Rice. 1.42 Upper first molar: triangular access cavity with three canals
Rice. 1.43 Upper first molar: access cavity extended to the mesial ridge to locate the MB2 canal on the line connecting the mesiobuccal and palatal canal
Second upper molar
Eruption occurs at the age of 12 years with the completion of the apical third at approximately 14 years.
It is smaller and shorter than the first molar by about 1-2 mm, is about 19-20 mm high and has four occlusal cusps. There are three roots and three canals, just like the first molar, and the MB root also has a second canal (37-42%). The shape of the pulp chamber is rhomboidal rather than triangular (see Figs. 1.42 and 1.43).
Upper third molar
This tooth erupts after age 17. It has a very unique anatomical morphology; the crown has three or five tubercles (Fig. 144). The average height of the third molar is about 18 mm. There may be one root or more often than one - three or four roots, usually curved distally (Figs. 1.45, 1.46, 1.47 and 1.48).
Figure 1.44. The upper third molars have a very distinctive occlusal morphology with three or four cusps
Rice. 1.45. Upper single root third molar
Rice. 1.46. Upper third molar with four distally curved canals
Rice. 1.47. Upper third molar with atypical anatomy
Rice. 1.48. Upper third molar with strong 3D root curvature
Milk and molar teeth in children
Many people believe that there are no differences between permanent and temporary teeth, but this is not true. So, how to distinguish a baby tooth from a molar? At a minimum, their number differs (milk - 20, permanent, as a rule, 32). Temporary teeth have a light shade, while permanent teeth are naturally more yellow. Indigenous ones are also significantly larger in size than dairy ones - visually it is quite easy to distinguish them. Here are the most common questions asked by Internet users on this topic.
- Do children have molars?
Of course, there are, and at a certain point they begin to actively erupt. - How many molars do children have?
From 28 to 32 (the maximum set appears after all eights appear). - Which molars appear first in a child?
Typically, the lower central incisor erupts first. - At what age do children start to get their molars?
Usually, dentition renewal begins after 6–7 years, but there are no strict limits. - Do children lose molars?
By themselves - no, as a result of injuries and illnesses - yes. - What are the risks of removing a molar tooth in children?
As corny as it may sound, his loss. And yes, a new one will not grow. Everything is like adults. - What to do if a child has yellow molars?
Permanent teeth have a more yellowish tint than temporary teeth. Plaque on a child’s molars is normal, but hygiene should never be neglected. - What to do if a child has black molars?
When teething, baby teeth may have a black color (the so-called Priestley plaque, or pigment bacteria). However, this does not happen with molars. If they are black, go to the dentist immediately. - What to do if a child does not have molar buds?
This happens, but very rarely. Fortunately, with modern implantation and prosthetics technologies, the problem can be solved. - Is it normal for a child to have crooked molars?
Contact an orthodontist immediately: correcting a bite in childhood is much easier and faster than in adults. - Which teeth do children replace with molars?
All twenty, plus new molars appearing.
Lower molars
Three molars in a quadrant without corresponding primary teeth.
First lower molar
This is the first permanent tooth that erupts at the age of 6 years and completes its formation at approximately 9-10 years. The crown has five cusps, two lingual and three buccal (Fig. 1.49). 22-23 mm long. There are usually two roots, one mesial and one distal (97%), and we rarely find a third distolingual root (3%). In the mesial root we find two canals in 65% of cases: they may have only one apical foramen (40%) or two separate ones (60%). The distal root has one canal (70%) or two canals (30%); there may also be two separate apical foramina (38%) or only one (62%) (Figs. 1.50, 1.51 and 1.52) (Figs. 1.53 and 1.54).
Rice. 1.49. Lower first molar: occlusal view
Rice. 1.50 Anatomical pictures from Hess and Keller: lower molar with very complex canal anatomy
Rice. 1.51 Anatomical pictures from Hess and Keller: lower molar with very complex canal anatomy
Rice. 1.52 Anatomical pictures from Hess and Keller: lower molar with very complex canal anatomy
Rice. 1.53. Micro-computed tomography scan of the roots of lower molars: note the complex morphology of the pulp space
Rice. 1.54. Micro-computed tomography scan of the roots of lower molars: modern digital techniques reproduce the subtle and complex morphology of the pulp space previously illustrated by Hess histological images
All roots on the buccal side have a moderate distal slope. The pulp chamber is triangular or square, depending on the number of canals (3 or 4), located in the center of the crown in the mesial-lingual area. Because of this feature, during the formation of the pulp chamber access cavity, it is important to be careful not to remove precious tooth structure in the distal area.
The shape of the access cavity should be triangular or trapezoidal with the larger base facing the mesial ridge and the smaller (or triangular apex if there is only one distal canal) slightly distal to the central occlusal fossa (Figs. 1.55 and 1.56).
Rice. 1.55 Lower molar: access cavity to three canals
Rice. 1.56 Lower molar: trapezoidal access cavity to four canals
If there is a third root, its mouth can be found along the bottom of the pulp chamber in the corners of the base of the trapezium.
Second lower molar
The tooth erupts at the age of 11 years and is very similar to the lower first molar with some differences.
It is smaller than the first molar by 1-2 mm in each direction. It has four cusps on the occlusal surface and usually two roots, one mesial and one distal. The mesial root has only one canal in 13% of cases; most often there are two channels that end in only one opening (49%), or there are two channels with two independent openings (38%). The distal root has only one canal in 92% of cases. Rarely there are two canals with one apical foramen (5%) or two separate foramina (3%).
The access cavity to the pulp chamber is located in the middle of the mesial-lingual region and has a trapezoidal shape. Due to the size of the pulp chamber and its proximity to the mesial-lingual wall, we advise careful design of the access cavity to avoid unnecessary excision of tooth structure (see Figures 1.55 and 1.56).
Third lower molar
Erupts after 17 years, usually at the age of 25. Also called "wisdom teeth", they have an atypical and varied morphology. It can have from three to five tubercles (Fig. 1.57). Often there is a fusion of roots from two or three roots. And, as a consequence, the anatomy of the canals cannot be schematized, as with the upper molar. Experience in root canal treatment will help the clinician perform the endodontic procedure correctly (Figs. 1.58, 1.59, and 1.60).
Rice. 1.57. The varied occlusal morphology of mandibular third molars may have four to five cusps
Rice. 1.58 (a) Lower third molar with a curved mesial root fused to the distal one. (b) Lower third molar: distal root
Rice. 1.59 (a) Lower third molar with four roots, two mesial and two distal: the mesiobuccal root is a very curved canal in the middle third. (b) Lower third molar: distal view showing graceful curvature of the distolingual root
Rice. 1.60 (a) Lower third molar: on the buccal side, two separate mesial roots are visible with extremely severe curvature, according to Schneider. The distal root has a moderate 3D curvature in the mesial and lingual direction. (b) Lower third molar: from the distal side, a 3D curvature of the distal root is visible in the lingual as well as mesial direction
Igor Lukinykh
Characteristics of temporary, replacement and permanent dentition. Part 1
Over the course of a person's life, temporary and then permanent teeth emerge successively in the oral cavity. Knowledge of the anatomical structure, timing of teething, characteristics of growth and development of the jaws at different stages of the formation of the maxillofacial system, physiological occlusions is important for doctors of all specialties. This general morphological direction is basic and determines the patterns of development of the dentofacial system and reveals individual characteristics.
Timing and basic patterns of eruption of primary teeth
A newborn child's jaws contain the rudiments of 20 temporary and 16 permanent teeth of various stages of development. The lower jaw is located behind the upper jaw, and between the alveolar processes in the anterior section there is a sagittal gap of up to 10 - 14 mm. During the thoracic period, the intramaxillary formation and mineralization of temporary teeth continues, and from the 6th month the process of teething begins and a temporary bite is formed. At the same time, mineralization of permanent teeth begins. The average age of teething is the age at which the tooth erupts in 50% of children. It has been established that in a zone with a high fluoride content in drinking water, the eruption of lateral incisors, canines, and second molars begins 2-3 months later compared to a zone with a low fluoride content in drinking water. The sequence of eruption of temporary teeth on each jaw occurs in the following order: I – II – IV – III – V, and in general in the occlusion as follows: Iн – Iв – Iв – Iн – Ivн – Ivв – IIIв – IIIн – Vн – Vв. The presented order of eruption is the most typical, however, options are also possible when the child’s lateral incisors erupt first, and soon after them the central ones. Teeth usually erupt sequentially, in pairs, symmetrically. Violation of paired eruption is observed with malformations of teeth and jaws. It is considered normal when, by the end of the 1st year of a child’s life, 8 incisors have erupted, then the first molars, canines and second molars (Table 1). Table 1. Timing of mineralization, eruption and formation of teeth
However, recently, due to acceleration processes, many children begin to erupt at an earlier time - 4 or 5 months of life, so some authors propose average periods of eruption, which were determined by them as a result of their own clinical studies (Table 2).
Table 2. Anatomy of primary teeth.
Temporary teeth differ from permanent teeth in size, shape, and color (Table 3).
Table 3. Comparative characteristics of temporary and permanent teeth
Among the temporary teeth there are: incisors – 8; fangs – 4; molars – 8. The teeth are not homogeneous in their structure. This depends on the group affiliation of the tooth, on the described surface of the tooth. For convenience of description, surfaces are distinguished: vestibular, lingual, medial, distal, occlusal. The group of temporary incisors are single-rooted teeth. There are 4 incisors on each jaw: 2 medial (central) and 2 lateral (lateral), left and right, respectively. What is common in the structure of the incisors is the shape of the crown, flattened in the vestibular-lingual direction near the cutting edge. The root has a cone shape.
Rice. 1
Anatomical shape of primary teeth of the right upper jaw
Rice. 2
Anatomical shape of primary teeth of the right lower jaw.
The group of temporary canines are single-rooted teeth. There are 2 fangs on each jaw: right and left. What is common in the anatomy of these teeth is the presence of a crown that is pointed on all surfaces and the longest cone-shaped root. Group of temporary molars. These are teeth with a multi-tubercular chewing surface and several roots. Primary molars are the largest teeth in the primary dentition. The child has 8 molars: 4 molars of the upper jaw - first and second (right and left); and 4 molars of the lower jaw - first and second (right and left).
There are several systems for recording the dental formula of primary teeth.
There are three main periods in the temporary dentition: 1st period (from birth to 2.5 - 3 years) - formation of the temporary dentition; 2nd period (from 3 to 4 years) – formed temporary bite; 3rd period (from 4.5 to 5 – 6 years) – reduction (abrasion, wear) of the temporary occlusion. The period of formation of temporary occlusion. With normal development of teeth and jaws, the process of eruption of temporary teeth begins at 6–8 months (Fig. 3), lasting up to 2.5–3 years. As teeth erupt and chewing function develops, involution of those organs that previously provided the act of sucking is observed. With the eruption of the second primary molars, the first rise in the height of the bite occurs. During this period, the alveolar process actively develops, the basal part of the lower jaw thickens, its branches grow, the outlines of the mandibular canal change, the size of the mandibular angle decreases, and the relief and architecture of the lower jaw become more complex. By 2.5 - 3 years, the temporary bite is considered formed. This period lasts up to 4 years and is a stable state of the dental system. Violations in the primary occlusion can lead to various complications, both local and general. They affect the growth and development of the jaws, the eruption of permanent teeth, reduce chewing ability, and lead to changes in the shape of the hard palate. Rice. 3
The period of formed temporary occlusion has the following dental characteristics: 1. There are 20 temporary teeth, they have a pronounced anatomical shape, 2. The teeth within the dentition have close contact. The contact point is point-like, but with an increase in physiological mobility, by the end of the period of formed temporary occlusion, the contact point becomes planar. 3. the upper and lower rows of teeth have the shape of a semicircle and their midpoints coincide with each other; 4. The teeth of the upper jaw in the frontal region overlap the teeth of the lower jaw. This is explained by the greater width of the upper dental arch compared to the lower one; 5. each tooth of the upper jaw articulates with two lower ones, with the exception of the second molar, which articulates only with its antagonist - the second lower molar; 6. The distal approximal surfaces of the second temporary molars are in the same vertical plane. By the end of the eruption of primary teeth, the first stage of physiological rise in the height of the bite takes place, which begins with the establishment of contact between the first temporary molars and ends with complete eruption and correct articulatory relationships of the second temporary molars. The next period of formation of the dental system is the period of reduction of the temporary occlusion, lasting from 4.5 to 6 years. A fully formed temporary bite during this period is unstable and undergoes a number of changes. It is also called the period preceding the change in the temporary bite, or the period of “wear and tear” of the temporary bite.
Fig.4 Fig. 5
Rice. 4. Reduction of temporary occlusion (models of the jaws): a) front view, b) rear view.
Rice. 5 Correct ratio
As a result of the growth of the jaw bones in preparation for the replacement of temporary teeth with permanent (larger ones), this period is characterized by the formation of physiological gaps between the teeth (diastemas - between the central incisors and three - between the remaining teeth). The abrasion of the cusps of the chewing teeth and the cutting edges of the frontal teeth gradually increases. The physiological mobility of individual teeth to be replaced increases. The dentition lengthens. Due to the abrasion of the chewing surfaces of the lateral teeth, a medial (towards the midline) shift of the lower jaw occurs and a “direct sliding bite” is formed. In this case, the incisors contact their cutting edges, and a medial step appears in the lateral area, formed by the distal surfaces of the second temporary molars (Tsilinsky’s symptom). This relationship of teeth ensures the subsequent correct position and relationship of the first permanent molars. The spaces of primates (diastema and trema) are a reserve site for the medial displacement of the lower dentition and the subsequent unimpeded placement of permanent teeth. Wearing of teeth leads to a decrease in the height of the crowns, and a straight “sliding” bite is formed. The differentiation of the elements of the temporomandibular joints is completed, the formation of third molars, the development and mineralization of premolars and second molars continues. Towards the end of the period of “wear and tear” of the temporary dentition, the eruption of the first permanent molars begins.
Timing and basic patterns of eruption of permanent teeth
The development of permanent teeth generally resembles the development of primary teeth. Permanent molars do not have temporary predecessors, which is why they are called additional molars. All other permanent teeth are replacement teeth. During the eruption of permanent replacement teeth, destruction and loss of temporary teeth occurs, which also includes progressive resorption of the roots of temporary teeth and their alveoli (Fig. 6).
Rice. 6
Due to the pressure of the permanent tooth on the alveolus of the temporary tooth, differentiation of osteoclasts begins, which are actively involved in the processes of bone tissue resorption. The localization of the zones of physiological resorption of the roots of temporary teeth varies depending on the group affiliation of the tooth: in single-rooted teeth it is located in the area of the apex of the tooth on the lingual side, and in multi-rooted teeth - in the zone of root bifructation. The timing of the eruption of permanent teeth with the correct development of the child coincides with the time of loss of temporary teeth (Table 4). The process of temporary tooth loss occurs synchronously with the process of permanent tooth eruption. Clinically, after the loss of a temporary tooth, cusps or part of the cutting edge of the erupting permanent teeth are detected.
Table 4. Timing of eruption of permanent teeth.
The eruption of permanent teeth begins with the first permanent molar at 6 years of age. Then, sequentially at the age of 6–8 years, the central and lateral incisors erupt. At 9–10 years of age, the first premolars erupt, followed most often by the canines (10–11 years) and the second premolars (11–12 years). At 12–13 years of age, the second permanent molars erupt. Thus, by the age of 12–13 years, all temporary teeth are replaced by permanent ones. The final formation of roots is completed by 15 years. Replacement teeth have a special anatomical structure that facilitates their eruption - a conductive canal, which contains a conductive cord. The anlage of such a permanent tooth is initially located in a common bone alveolus with its temporary predecessor. It is subsequently completely surrounded by alveolar bone, with the exception of a small canal containing the remains of the dental plate and connective tissue. Together, these structures help guide the movement of the permanent tooth as it erupts.
Periods of mixed dentition
So, with the eruption of the first permanent molar, the mixed dentition begins. The mixed dentition represents a higher degree of development and differentiation of the masticatory apparatus. It is characterized by the presence of temporary and permanent teeth, which lasts from 6 to 12-14 years. The mixed bite is of particular interest to orthodontists, because at this time the most intensive growth of the jaw bones occurs, metabolic processes in bone tissue are at a high level. Therefore, timely identification of etiological factors is especially effective during the day, as is the treatment of dental anomalies themselves. However, information about the development of mixed dentition is ambiguous. So, for example, A.D. Osadchiy (1967) distinguishes two periods in the mixed dentition: 6 – 8 years – early mixed dentition and 9 – 12 years – late mixed dentition. I.L. Zlotnik (1952) also distinguishes these two periods, but with an age difference of 6 - 9 and 10 - 12 years, respectively.
Rice. 7
This allocation of periods is associated with the presence in the dentition during the period of early mixed dentition of the first permanent molar, four permanent incisors on the upper and lower jaw. And premolars and canines are in the period of late mixed dentition. At 9 years of age, the growth of the jaw bones slows down, but there is a noticeable growth of the alveolar process, associated with the eruption of permanent canines and premolars and the formation of the roots of the incisors and first molar (F.Ya. Khoroshilkina, 1999). This division takes into account the growth rate of the jaw bones and alveolar process and the level of intensity of metabolic processes in them. The eruption of the first permanent teeth (first molars) provides a second physiological rise in the height of the bite, and sagittal and transversal occlusal curves are formed. The third period of increasing the height of the bite begins at 12 years of age with the eruption of the second molar. It is accompanied by active growth of the dentoalveolar arches, which lasts from 13.5 to 15 years. During the development of the chewing apparatus in children, the mixed dentition is the most labile. The simultaneous presence in the oral cavity of temporary teeth that have lost stability due to root resorption, and permanent teeth that are at various stages of eruption and root formation, leads to a significant decrease in chewing function, leading to uneven training of the masticatory muscles, abnormal growth of the jaw bones and often the formation of anomalies dental system. During this period, both self-regulation of existing anomalies and the formation of new ones are noted. Due to the unstable condition of individual parts of the dental system and the entire masticatory apparatus as a whole, as well as the increased growth of the jaws during this period, it is necessary to use it to perform corrective orthodontic interventions. Article continues here
Authors: V.I. Kutsevlyak, A.V. Samsonov, S.V. Altunina, Yu.V. Tkachenko