Currently, dental anomalies are very common. As a result of studies conducted by domestic specialists, one or another of them was identified in four out of ten children of younger and middle age. Irregularities in the arrangement of teeth in rows can be congenital or arise for various reasons. These anomalies are characterized by pathological changes in the shape and size of the lower and upper dental arches. In this case, crowding, displacement, asymmetry, changes in numbers, and disturbances in the closure and occlusion of teeth are manifested. These anomalies are easily identified during a simple dental examination and with the help of radiography, as well as by studying impressions of the dentition. Overcoming these anomalies today is possible and consists in restoring the normal shape and length of the dentition through surgery, the use of orthodontic methods, through prosthetics or wearing regulatory devices. In some cases, with defects in the dentition, it is advisable to install durable metal-ceramic crowns.
Causes of anomalies
There are three types of violations of the norms of arrangement of teeth in rows: transversal (horizontal), sagittal (antero-posterior) and vertical anomalies. The former arise as a result of certain pathologies (for example, rickets), due to difficulty breathing through the nose, as well as due to constant muscle contractions (chewing, facial and tongue), not related to eating, facial expressions and speech. Also, causes of transversal disorders can be early loss of teeth, finger sucking, and sluggish chewing of food.
Sagittal anomalies occur due to a delay in the replacement of baby teeth with permanent teeth, due to lack of space in the row, and difficulty breathing through the nose. They can also be caused by undesirable habits (constant sucking and biting of fingers, pacifiers and other objects), lack or presence of extra teeth, incorrect position of their rudiments, shortened frenulum of the tongue, difficulty swallowing, breathing and speech, congenital structural features of the facial bones. Sagittal anomalies also occur when one or more teeth are too large or small, when they erupt outside the arch, or due to improper artificial feeding of the baby.
Vertical anomalies arise due to a violation of the contact (closing) of the dentition, bad habits, uneven development of the jaws and their individual sections. Also, the causes of these disorders are damage to the hard tissues of the teeth (in particular, as a result of caries), and uneven abrasion. Vertical anomalies also occur due to improper eruption or premature loss of primary or permanent teeth, especially lateral ones (molars and others).
Fortunately, today it is not difficult to close gaps or defects that have appeared in the dentition for various reasons. In many cases, for prosthetics of your own or implanted (both anterior and lateral) teeth, a good solution would be to install a durable and aesthetic metal-ceramic crown.
ANOMALIES OF DENTAL ARCH RELATIONSHIP
Anomalies of the dental arches are mainly congenital pathologies and manifest themselves in lengthening, shortening, narrowing or expansion of the dentition or its individual sections. There are also disturbances in the relationship of the dental arches, when there is an asymmetry in the location of the upper or lower jaw in relation to each other. These pathologies are identified during examination and classified depending on the clinical picture.
For information about prices and treatment times, call:
+7
or fill out the feedback form:
Types of dental arch relationship anomalies
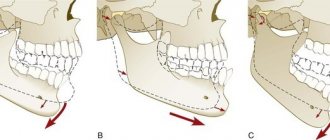
Pathologies of the dental system that affect changes in the position of the dental arches include distal (prognathic), mesial (medial), deep, open and cross bites.
- Distal bite. One of the most common pathologies diagnosed with baby teeth or their replacement with permanent ones. Manifests itself in the form of protrusion of the upper jaw in relation to the lower jaw. The causes of development may be disturbances in the size and shape of the dentition or its underdevelopment. This pathology can also be determined visually by the protrusion of the upper lip and visible front teeth. Typical facial features are a shortened lower part of the face, a half-open mouth and chin folds. Distal bite causes disruption of chewing and speech functions and therefore requires timely treatment.
- Mesial bite. The clinical picture of this pathology is the advancement of the lower dentition in relation to the upper one when the jaws are closed. Outwardly, this anomaly is especially noticeable when you look at a person in profile. It is characterized by a massive chin protruding forward and a recessed upper lip. The reasons for the development of pathology include a number of factors: birth trauma, disease, improper feeding, premature loss of upper teeth. Like the distal bite, the mesial bite causes not only discomfort, but also disturbances in speech and the process of chewing food.
- Deep bite. A fairly common violation of the relationship of the dental arches, in which the lower incisors overlap the upper incisors by at least a third. With severe pathology, this term is replaced by the concept of excessive incisal overlap. This anomaly is classified into vertical and horizontal. When vertical, the incisors and canines of the upper jaw overlap the lower ones by more than half. When horizontal, the normal distance between the vestibular surface of the lower teeth and the palatal part of the upper teeth is disrupted. Pathology develops due to genetic and postpartum factors (congenital anomalies, chronic diseases). Treatment should begin already during the eruption of baby teeth. Elimination of minor incisal overlap in adulthood is not required, but in case of severe pathology, mouth guards and braces are used.
- Open bite. This pathology is diagnosed when the upper and lower jaws are not completely closed in the frontal region. This is the most severe form of dental arch relationship abnormality, most often found in young children. It makes it difficult to chew food and pronounce certain sounds, and dries out the mucous membrane. In addition to congenital causes, external factors can also contribute to the formation of an open bite: poor nutrition, poor physical activity, and even lack of sunlight. Treatment of an open bite is a rather complex process, but today this disorder can be eliminated if not only therapeutic but also preventive measures are taken.
- Crossbite. This anomaly manifests itself in a discrepancy between the position of the upper and lower jaw in the transverse direction. In other words, the jaws are displaced relative to each other in the horizontal plane, which is noticeable during normal examination. As a rule, the pathology affects the anterior and lateral parts of the dentition. Its causes may be unfavorable heredity, early loss of baby teeth, childhood diseases, and facial injuries. Crossbite causes asymmetric development of bones and joints, impaired speech and chewing function, so its treatment should begin from a very early age.
Treatment of anomalies in the relationship of the dental arches
Treatment is prescribed after examination, diagnostic examination and diagnosis. With a professional approach and timely treatment, these pathologies of the dental system can be corrected and eliminated. For example, treatment of distal and mesial occlusion is very effective. In childhood, measures are taken to normalize the shape of the dentition with preventive measures. If the jaw has already formed, then using orthodontic devices and bite plates, the upper jaw is expanded and the front teeth are moved back. A similar principle is used to treat mesial occlusion, correcting the relationship of the anterior teeth. Other types of pathologies also have their own treatment regimens, which the orthodontist will prescribe for you when you visit our clinic.
Manifestations of anomalies
Transversal disturbances in the arrangement of teeth in rows are characterized by excessive narrowness or width of the arches, insufficient development and disruption of the shape of the jaws. With transversal anomalies, pathological bites (deep, open or cross) are observed. Also, with violations of this type, the following irregularities in the location of the teeth and arch configuration occur:
- V-shaped, in which the lateral sections are narrowed and the frontal segment protrudes forward, the incisors are rotated around their axis;
- acute-angled, in which the arch evenly narrows at the locations of the fangs;
- asymmetric, characterized by displacement of the lateral sections of the arc or one of them relative to the imaginary midline;
- saddle-shaped, in which there is a narrowing of the arch in the locations of small molars and first molars;
- trapezoidal, characterized by flattening of the anterior section of the jaw and a slight decrease in the gap between the lateral segments;
- generally narrowed, characterized by a very close arrangement of all teeth, their approach to an imaginary midline. In this case, the frontal section of the arc can be moved forward or shifted back.
Sagittal disorders are buccal or labial displacements of the teeth, their deviations from the row forward (outward) or into the oral cavity, lengthening and shortening of the arches. With anomalies of the sagittal type of dentition, a general or partial forward displacement of the upper jaw relative to the lower jaw is observed (this pathology is called “prognathia” or “distal bite”). Also, with sagittal abnormalities when closing the jaws, the teeth located in the lower row completely or partially overlap their antagonists located above. At the same time, the chin and lower lip protrude significantly forward.
With vertical anomalies, shortening and lengthening of individual sections of the dentition develops. In this case, there is a very unaesthetic symmetrical or random displacement up and down of paired and individual teeth relative to others, both in the frontal and lateral sections of the jaw arches.
Anomalies of the dentition
Correction of dentition anomalies involves the use of orthodontic, surgical and orthopedic dentistry methods, leading to the expansion or contraction of dental arches and the correct placement of teeth. A rational method of treatment is determined taking into account the combination of several factors: the closure of the lateral teeth, the causes of the anomaly (underdevelopment of the base of the jaw, etc.), the narrowing of the dental arch, the age of the patient (whether the period of active jaw growth has ended). It is also taken into account whether it is possible to eliminate the anomaly using orthodontic methods alone, or whether it is necessary and advisable to include surgical and orthopedic treatment methods, etc.
Correction result
Orthodontic treatment
Currently, there are a significant number of different systems of orthodontic appliances that can successfully eliminate many dental anomalies. In children with primary dentition and during the eruption of permanent teeth, deviations are eliminated using plate devices with screws. With a uniform narrowing of the dentition, the screw is placed in the premolar area in the middle of the dental arch, and with a deep palate, a Coffin spring is used.
If the narrowing of the dentition is accompanied by protrusion of the upper frontal teeth, a plate orthodontic apparatus with a screw, supplemented by a vestibular arch, is used. When the narrowing is located in the anterior or posterior segment of the dentition, the screw is installed according to the location of the anomaly. Limiters are used according to indications. In the case of unilateral narrowing or displacement of several teeth, an asymmetrical position of the screw and cutting of the plate are used. With a trapezoidal shape of the dentition (its flattening in the frontal area), a plate with a sectoral cut in the area of the incisors is used, and if the anterior section of the upper jaw is shortened, it is possible to use Schwartz and Bynin mouthguards.
With a permanent dentition, the impact on dentition anomalies is carried out using fixed equipment (for example, an Angle arch) and bracket systems, through which it is possible to simultaneously move the teeth forward and give a normal position relative to their own axis. When the lateral segments of the dentition are shortened, there is often not enough space for the canines and premolars due to the fact that the first molars are displaced forward. To give them a normal position, it is recommended to use a plate with a sectoral cut, a screw and a clasp on the displaced tooth. In such cases, orthodontic methods alone may not be enough, so it is necessary to resort to the removal of a premolar, which is why treatment is best carried out immediately after the eruption of permanent teeth.
Recently, non-removable arc orthodontic devices and lingual braces, which are fixed on the palatal side of the tooth crowns, have become increasingly widespread. Being very functional, they have significant aesthetic advantages, since they are not visible to others, which is important for patients, especially during puberty.
Orthopedic treatment
When the dentition expands, the patient develops gaps and spaces between the teeth. Elimination of threes and diastemas using orthodontic appliances is difficult, since the occurrence of such anomalies is usually associated with an increase in the body of the jaw or alveolar process. The problem can be eliminated with prosthetics. But if the gaps are not too significant and do not cause any complaints from the patient, orthopedic and orthodontic treatment is optional.
Surgery
In cases of macrodentia and crowded teeth, orthodontic treatment alone is ineffective. To move teeth into the correct position, it usually requires the removal of 1-2 teeth, most often premolars, in place of which abnormally located incisors and canines are moved. This combination of orthodontic and surgical dentistry is often used in older patients, but if the diagnosis of macrodentia is made during the period of changing teeth, it is possible to use the Hotz method, in which sequential removal of primary teeth allows the correct placement of erupting permanent teeth. Timely use of this method often makes it possible to avoid orthodontic care or make it minimal.
Anatomical features of the lower teeth
- The central incisor is the smallest tooth in the “adult” bite and the smallest among the incisors. The root is quite short, in 65% of cases there is one root canal, less often - two.
- The chisel-shaped lateral incisor is always larger than the central one. One or less often two root canals – both narrow. “Adult” incisors on the lower jaw are less susceptible to damage than others, so dentists rarely turn to them for the treatment of caries in children and adults.
- Fang - similar in structure to the upper one, but is smaller in size. In 96% of cases it has a single root canal of normal structure.
- The first premolar has a rounded crown in cross-section and two characteristic tubercles on the chewing side. One root is slightly flattened.
- The second premolar is very similar in crown shape to the canine, and is always larger than the adjacent premolar. The surfaces of the single root are smooth and slightly shiny. Two roots occur in only 3% of cases or less.
- The first molar with a cubic crown has five cusps on top of the crown, separated by an F-like fissure. In 88% of cases, three root canals are formed.
- The second molar is smaller than the first, but completely replicates its anatomical features. Root canals are curved and have poor patency. In 85% of cases, the tooth has three canals, in 10% - four.
The anatomical characteristics of teeth are similar in all people, but each person may have individual characteristics, for example, the absence of wisdom teeth or an increased number of root canals in a particular tooth.