You can contact Dr. Granov's clinic for treatment of jaw injuries. This is one of the areas of treatment that we do.
The jaw is the bony structure that holds the teeth in place. The upper jaw does not move, only the lower jaw moves. Its movements are necessary for eating food and for producing speech. Both jaws connect at a point called the temporomandibular joint (TMJ).
Jaw injuries include cracks, dislocations and fractures. With a fracture or crack, the bone breaks; with a dislocation, the bone changes location and flies out of the joint. Such injuries occur after physical activity (bruise, blow, fall). After appropriate treatment, they heal safely, but the dislocation may appear again.
Jaw injuries are dangerous because they can lead to various complications. Among them:
- breathing disorder,
- bleeding,
- blood entering the lungs
- problems with chewing food,
- problems with diction,
- infection of the jaw or facial structures,
- joint pain,
- numbness of the jaw or face,
- tooth displacement,
- edema.
Symptoms of a jaw fracture:
- pain in the cheek next to the ear, which increases with jaw movement;
- swelling of the face, blood in the mouth;
- immobility of the jaw, inability to open or close the mouth;
- when opening the mouth, only one side of the jaw moves;
- jaw pain that gets worse when chewing;
- dental injuries;
- swelling of the face or changes in the contours of the jaw;
- numbness of the face in the lower lip area.
Symptoms of a dislocated jaw:
- pain in the cheek next to the ear, which increases with jaw movement;
- feeling that the jaw is not positioned correctly in the joint;
- violation of diction;
- inability to close your mouth;
- drooling due to open mouth;
- spasm of the masticatory muscles or protrusion of the jaw forward;
- dental injuries.
First aid for jaw injuries
Jaw injuries require immediate medical attention. Call an ambulance or go to the nearest hospital. Before doctors arrive, you can put a bandage on your jaw to keep it immobilized. The bandage should be easy to remove.
Do not try to set a dislocation yourself or wait for the fracture to heal on its own. Be sure to contact a traumatologist.
Treatment of a jaw fracture
Treatment depends on the extent of the fracture. If the patient has a small crack in the bone, it will heal on its own. The doctor will only prescribe a painkiller.
Severe fractures require surgery to allow the bones to heal properly. After surgery, a bandage is applied to the jaw to allow it to heal quietly. The jaw takes 6 to 8 weeks to heal. At first, elastic bandages are additionally applied, which are then removed to allow the muscles to be developed and their mobility restored.
During treatment you can eat only liquid food. You should always have scissors with you to cut bandages in case the patient suddenly chokes on something or starts vomiting. Then go to the hospital to have a new bandage applied.
Why do my dentures keep falling out?
Answer: Yes, this can happen.
A removable denture, if not worn constantly, may fall out if you put it on and start using it over time. Over time, the jaw changes, but a false plastic jaw does not. Of course, it is possible that the prosthesis was not made entirely accurately right away. At the same time, if initially the impressions were accurately made, and nothing happened to the patient’s general condition throughout, for example, he did not lose weight, then after a while you can put on the teeth and they will stick in the same way.
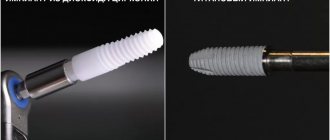
What should a suction complete removable denture look like? Gentlemen, ATTENTION, please pay attention to this photo: this is what a complete removable denture for the upper jaw looks like from the side of the palate, you need to pay attention to its volumetric border, the edge of the denture has an individual and different thickness everywhere, which is dictated primarily by the impression taken from the oral cavity .
Now compare with your dentures! You can say that everyone’s oral cavity is different and the volume of the border may not be on an already made prosthesis... yes, it can, but this is extremely rare and, most importantly, not along the entire length of the border! Now that you have looked at your individual margin, you can see if it is too thin, lacking volume, what is the reason for the constant loss of removable teeth.
How can this be eliminated?
In this case, only a dentist can help you. As for us, we always take impressions very carefully; they have an individual volumetric border, which in the future positively and necessarily prevents loss! A dentist, if a patient comes to him with a similar complaint, must take a functional impression of an existing denture. In this case, the entire internal surface of the previous prosthesis must be removed to create space for the impression material. By introducing the prosthesis with the impression mass into the oral cavity, we create a volumetric surface with massaging movements. Then the work is transferred to a dental technician, he carries out the polymerization process and here is a removable denture with a new inner part that is perfectly fixed!
The task is to create a suction removable denture! The valve zone serves as the link that allows the denture to be suctioned. If a functional, individual edge is not created, then if the patient uses fixing creams, then the glue consumption will be too high. Denture adhesive will wear out quickly.
Dentist Ivan and Alexey, when making each removable denture in the absence of all teeth on the jaw, are required to create a valve zone to prevent the loss of the false jaw.
167091cookie-checkWhy do my dentures keep falling out?no
Treatment of jaw dislocation
A dislocated jaw is treated simply: the doctor realigns the joint, placing the bone in the right place. Muscle relaxants or painkillers may be needed to relax tight muscles.
Then the jaw must be secured in a stationary state. To do this, the doctor applies a bandage. If the dislocation does not appear for the first time, then surgery will be needed to straighten it.
Recovery after a dislocation lasts 6 weeks. At this time, you should not open your mouth wide. When yawning and sneezing, the lower jaw should be supported with your hands.
Dislocations of the lower jaw
Features of the functioning of the joint in patients suffering from habitual dislocations are revealed by examination, palpation and auscultation. Habitual dislocations of the lower jaw are characterized by significant excursions of the heads when opening the mouth. They are well defined by palpation. The heads of the lower jaw, slipping past the top of the articular tubercles of the temporal bone, overstretch the capsule and the muscular-ligamentous apparatus, thereby causing severe pain in the joint and disruption of its function.
When listening, clicking sounds are revealed, the occurrence of which is associated mainly with the weakening of the connection between the disc and the head of the lower jaw and their asynchronous movement during the functioning of the lower jaw. The mechanism of their occurrence when opening and closing the mouth is as follows. When the mouth opens, the head of the lower jaw and the disc begin to travel anteriorly. At some point along this path, the synchronous movement of the head and disc is disrupted: the disc lags behind the head and is pressed against the articular tubercle; the head, moving further, jumps over the anterior pole of the disc, making a clicking sound (anterior pole clicking when opening the mouth). With the reverse movement of the lower jaw, clicking may occur again at the moment of overcoming the anterior pole (anteropolar clicking when closing the mouth).
If the disk remains in place or does not move along with the head (the movement of the head and disk will be asynchronous), then with further movement back the head will pass through the posterior pole of the disk, and a clicking sound will appear (posterior pole clicking when closing). Further, when opening the mouth (at the very beginning), a clicking sound occurs at the moment of overcoming the posterior pole and at the end of opening when overcoming the anterior pole.
Dislocations of the lower jaw should be differentiated from dislocations of the articular disc. The pathogenesis of intra-articular disc dislocation is based on either deep structural disorders that weaken the connection of the disc with the head of the mandible, or neuromuscular disorders, primarily spasms of the lateral pterygoid muscle; or a combination of these factors.
Disc dislocations, caused by the loss of its strong connection with the head of the lower jaw, can occur with any movements of the lower jaw. Disc displacements cause pain and limitation of movement in the joint due to pinching of its components. An anteriorly displaced disc can block the movement of the lower jaw.
Disc dislocations caused by spasm of the lateral pterygoid muscle are accompanied by pain. The occurrence of pain with anteromedial disc dislocations is explained by excessive stretching and rupture of the posterior condylar fusion. In addition, when closing the mouth, the head of the lower jaw precedes the forward movement of the disc backwards and enters the neurovascular zone of the “retrodiscal cushion”, causing its compression and pain of arthrogenic origin.
When the lower jaw moves, clicking sounds occur. The mechanism for the occurrence of clicking in the joint during disc dislocation is explained as follows. With spastic contraction of the lateral pterygoid muscle, the disc and head are displaced anteriorly, the disc remains in this position until the muscle relaxes. If at this moment, as a result of contraction of the muscles that lift the mandible, the head returns to its original position, then it, jumping over the posterior pole, makes a clicking sound. Sound may also occur when opening, since the head must overcome the rear pole of the disk.
The differential diagnostic sign is pain on palpation of the lateral pterygoid muscle. Additional information can be obtained from electromyography. The appearance of bioelectrical activity at rest in the masticatory or facial muscles, and the asymmetry of the activity of the muscles of the same name indicate the muscular mechanism of disc dislocation.
Disc dislocations are not visible on plain radiography and are difficult to identify using tomography of the joint; Arthrography is labor-intensive, complex and unsafe.
The most valuable for these purposes has been computed tomography of the TMJ, which makes it possible to easily differentiate different tissues of the joint and identify the condition and position of the disc. When a disc dislocates, it causes anterior displacement, sometimes rupture of its posterior attachments, and perforation of the disc. A disc that has moved anterior to the head blocks the movements of the lower jaw.
What can be considered pathology?
Normal occlusion is such a relationship of the dentition in which between
All teeth are in contact, the upper incisors overlap the lower ones by 1/3. When turning to an orthodontist, many patients ask the question: when the jaw moves forward, what kind of pathology is this? Unfortunately, this is one of the most complex dental anomalies, which was already mentioned above - mesial bite. Due to the skeletal nature of the anomaly and significant morpho-functional disorders, it is difficult to correct. But this does not mean at all that you need to resign yourself to the situation. It just takes more time and effort than, for example, eliminating interdental spaces. The prevalence of this pathology is about 4% of the total population. According to scientists, the key factor in its development is disturbances during the embryonic development of the fetus. As a result, the child experiences growth retardation in the middle third of the face. During adolescence, the growth of the lower jaw, on the contrary, accelerates excessively. As a result, the occlusion is broken. Evidence also suggests that patients experience poor posture. The psycho-emotional background also suffers. Reverse overlap cannot in any way be called a correct bite. This defect definitely requires treatment.
The lower jaw is pushed forward
Why does the lower jaw move forward? Most often, the matter is in its excessive development and structural features. It is enlarged, pushed forward, the corners are turned. In this case, it is necessary to distinguish between true and false mesial occlusion, or, as it is also called, progeny.
With false progeny, reverse bite is present only in the frontal part of the jaw. In the lateral sections, the closure remains within the normal range, or is slightly disturbed. This condition can develop due to underdevelopment of the upper jaw.
With true progeny, reverse overlap is present in both the anterior and lateral sections. When the teeth close together, a space is formed in the area of the incisors, and there is no contact. Biting and chewing food is seriously difficult due to such a serious violation of the relationship of the dentition. Orthodontic treatment in this case can radically improve the patient’s quality of life. An integrated approach will normalize occlusion and eliminate deficiencies of both an aesthetic and functional nature.
Some disorders in patients are noticed only by the dentist. With progeny the situation is different. Often parents, even in childhood, notice that their child’s bite is not forming correctly. Adult patients are also aware of their problem, but for various reasons they do not consult a doctor. Thanks to the development of technology and orthodontic devices, today it is possible to correct a bite at almost any age. Mesial occlusion sometimes requires surgical intervention. In some cases, for example with false progeny, it is not necessary. Don’t be afraid to consult a doctor - it may not take much time to solve your problem.
The upper jaw is pushed forward
Jaw disproportion can also be observed in the opposite relationship. With distal occlusion, the size of the upper jaw may not correspond to the size of the lower jaw, which turns out to be underdeveloped. The situation can be aggravated by the vestibular inclination of the teeth (they are tilted forward). The anomaly becomes noticeable during puberty, when active growth of the upper jaw occurs. In the lower jaw, the size of which is insufficient, crowding of teeth may occur. Is it possible to correct a distal bite with braces? In adults, this is the only possible method of correction. During the treatment, the relationship of the dentition is normalized. Often the teeth in the frontal region do not close together, which causes a gap to form and diction suffers. After orthodontic treatment, you can take a course of classes with a speech therapist, and normal sound pronunciation will be restored. Thus, when a patient asks the doctor a question: the upper jaw is pushed forward, how to correct it? – the doctor first conducts an examination and examination, and then draws up a treatment plan. Orthodontist Irina Butorina knows how to correct a distal bite.
Why is the jaw pushed forward and why is it dangerous?
When the lower jaw is pushed forward, why is this dangerous? First of all, the act of chewing suffers. It is almost impossible to fully bite and chew food with this type of anomaly. But for patients, sometimes the aesthetic factor is more important. This defect is one of the most pronounced, and the problem of disproportion of the oval of the face comes to the fore. The lower third looks elongated, the chin protrudes forward, and the upper lip sinks. Also, mesial occlusion has a negative impact on the condition of teeth and gums, the temporomandibular joint. The chewing load is distributed unevenly. Sometimes there are significant accumulations of plaque. The risk of developing periodontal disease is very high.
So, the lower jaw is pushed forward, how to correct the situation? Unfortunately, sometimes orthodontic treatment is not enough. Then the surgeon comes to the aid of the orthodontist. During the intervention, the body of the lower jaw is shortened, which allows it to return to its physiological size. Thus, the very root cause of the development of malocclusion is eliminated. What is the name of the operation when the lower jaw is pushed forward? This is an osteotomy. It is performed under anesthesia, the surgeon cuts the bone at a certain angle, removes excess bone tissue, then aligns and fixes the lower jaw in the desired position. The technology for performing this operation is very well developed. It is well tolerated by patients. As a rule, discharge occurs on the 3rd day. But it must be said that osteotomy is performed only after treatment with braces.
Why does jaw curvature occur in adults?
There are a number of factors that lead to malocclusion:
- Genetics. One of the common causes of dental deformities in adults. Unfortunately, it is impossible to influence genetics. However, if you analyze the dental system of parents, you can predict what dental problems their children may have.
- Anomalies in the development of the dental system. A crooked jaw in an adult can develop due to diet. The predominance of soft foods often leads to disruption of the development of the dentofacial apparatus, which subsequently causes curvature of the teeth.
- Early loss of baby teeth. Disruption of the physiological processes of changing teeth often leads to a change in their position during eruption. A similar situation can arise in adults when removing damaged or untreatable teeth.
- Abnormal position of dental germs. Deviation of the axis of eruption of units of the dentition, which persists into adulthood, often leads to curvature of the jaw.
- Wisdom teeth. Eights are characterized by late maturation, so by the time they erupt, as a rule, there is not enough space in the dentition. Having a great potential for eruption, they begin to displace neighboring units, which causes the development of dental anomalies.
- Somatic diseases. For the normal development and functioning of the upper jaw, nasal breathing is necessary. In the presence of otolaryngological pathologies, mouth breathing develops, which leads to underdevelopment of the maxillary bone and curvature of the dentition.
- Problems with the locomotor system. Poor posture, problems with the spine and other factors often lead to disruption of the functioning of the temporomandibular joint, which in turn contributes to disruption of occlusion.
Aesthetic consequences of loss of bone volume due to missing teeth
The facial changes that naturally occur with age can be exacerbated and accelerated by tooth loss. Pronounced aesthetic consequences result from loss of alveolar bone. Patients do not even suspect that all these changes in soft tissues are associated with tooth loss:
- Reduction in facial height occurs due to disturbances in the vertical dimension of the alveolar bone.
- A change in the labiomental angle and deepening of the vertical lines in this area give the face a rougher appearance.
- A malocclusion develops. As a result, the chin turns forward.
- The corners of the lips droop, the patient's face has an unhappy expression.
- Due to poor support of the lip by dentures and loss of muscle tone, the border of the red border of the lips becomes thinner.
- Age-related deepening of the nasolabial philtrum and other vertical lines on the upper lip is more pronounced with loss of bone volume.
- In edentulous patients, the decrease in the tone of the facial muscles that support the upper lip occurs faster, and the lengthening of the lip occurs at an earlier age. As a result, the smile ages.
- Bone atrophy has a negative effect on the attachment of the mental and buccal muscles to the body of the mandible. The fabric sags, creating a double chin. This effect is caused by decreased muscle tone when teeth are lost.