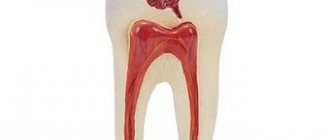
Among existing dental pathologies, the most common problem is caries - a disease that has no age restrictions. The development of carious processes entails the destruction of dental tissue, disrupts the aesthetics and functionality of the jaw, causes pain and provokes the occurrence of more complex diseases of the oral cavity. The classification developed by the American dentist G.V. allows us to assess the degree of progression of the pathology, as well as select the optimal method of treatment. Black.
System principle
The differentiation method, proposed by a dentist back in the century before last, is based on the use of criteria for assessing the coverage and localization of the lesion. Based on them, a systematic approach is used that allows dividing the types of caries into five classes. It is worth noting that due to the age of development, the classification does not include types of caries discovered in a later period (for example, secondary and root forms). Nevertheless, the technique remains relevant in modern practice.
Classification of caries lesions according to the process
In this direction, there are 3 types of dynamics of the course of this disease: fast, slow and stabilized.
Also, this pathogenic process can be considered by the extent of its localization: caries manifests itself on one tooth, on several elements, or is systemic in nature and affects most of the different teeth in the upper and lower rows.
Classification
The five classes of caries development, defined initially, were subsequently supplemented with an auxiliary degree, which makes it possible to more accurately determine the specifics of the pathology and select the correct treatment plan. Based on the Black scale, the doctor selects the appropriate material for making a filling, a method for preparing dental tissue, as well as a method of therapy that can give the maximum positive effect in the short term.
Black's classification of carious diseases represents the following forms of pathology:
- The first class is damage to the deepened areas of the natural relief of the crown, usually diagnosed on incisors and canines, as well as premolars. The disease occurs on a surface exposed to constant stress when eating food, so treatment of the lower and upper teeth involves the formation of a filling made of a composite material. A distinctive feature is the use of a structure with a reduced enamel bevel, which allows you to restore occlusion and correctly distribute mechanical pressure on the jaw row. The photopolymer composition is applied at an angle to the base, which ensures the density of the structure and reduces the likelihood of chipping.
- The second class is caries, which manifests itself on molars and premolars in the area of contact areas. It spreads both distally and medially, and in some cases affects the unit on both sides. The treatment method involves opening the crown through the contact area, excision of pulp tissues that have undergone necrosis, and fixing the filling using an adhesive composition.
- The third class is a pathology that covers the canines and incisors in the area of closure, without affecting the angular and cutting edges. Due to the complexity of the location, it provides for increased requirements for aesthetic restoration. To restore functionality and appearance, it is recommended to use composites whose polymerized structure is identical to natural tooth enamel.
- The fourth class is caries that forms in the corners and cutting edges of the fangs and incisors. Traditionally associated with mechanical injuries resulting from the application of a contact directed force to the crown. In such situations, the dentist is required not only to eliminate the cause of the development of the pathology, but also to restore the aesthetic properties of the dentition, since the affected area is located in the smile zone. Depending on the degree of damage to the base, composite materials, ceramic plates (veneers, lumineers, etc.), as well as artificial crowns made of porcelain, metal-ceramics or zirconium dioxide are used.
- The fifth class is caries, which affects the front and back parts of the dentition, manifesting itself in the area of the junction with the gum tissue, as well as in the root part of the teeth. In this case, the cause of destruction is not only the carious process, but also internal pathologies, which are characterized by erosive manifestations. To eliminate the consequences of the disease, plastic surgery of gum tissue and installation of a composite filling are recommended.
An additional, sixth class, the use of which in the system was proposed by the World Health Organization, includes forms of pathology that manifest themselves on the cutting edges of the frontal and chewing units. Orthopedic restoration involves the installation of artificial crowns or decorative plates, while the price for caries treatment is determined by the choice of material, as well as the complexity of the dental procedure.
Classification of caries according to the sequence of occurrence
As in the previous gradation, experts distinguish 3 types of carious lesions.
The first category includes caries that appeared on a tooth for the first time.
The second is a re-injury to a previously filled tooth. In the vast majority of cases, this disease spreads around or under the filling.
The third category includes the so-called recurrent caries lesion. It occurs due to insufficient treatment of the area or a poorly installed filling.
Secondary caries is all new carious lesions that develop near a filling in a previously treated tooth. Secondary caries has all the histological characteristics of a carious lesion.
The reason for its occurrence is a violation of the marginal seal between the filling and the hard tissues of the tooth; microorganisms from the oral cavity penetrate into the resulting gap and optimal conditions are created for the formation of a carious defect along the edge of the filling in the enamel or dentin.
Recurrent caries is the resumption or progression of the pathological process if the carious lesion was not completely removed during previous treatment. Recurrence of caries is often detected under the filling during an X-ray examination or along the edge of the filling.
There are a large number of caries classification systems, almost all of them are repeated. Therefore, for an accurate diagnosis, it is very important for a specialist to correctly determine the depth of the cavity, the nature of the course and the main reason why the carious pathology formed.
The effectiveness of treatment and the absence of relapse processes in the future will depend on the reliability of the diagnosis.
Filling class II cavities with composites in difficult situations
Despite advances in composites in almost every aspect, restoration of Class II cavities is still considered a challenging and time-consuming task for the dentist. To successfully fill a class II cavity, the specialist must ensure that there is no open interproximal contact, inaccurate anatomical contour, inadequate marginal sealing, and prevent postoperative sensitivity, edge staining, recurrent caries, and filling loss.
With more than 70 restorative materials and 50 flowable composites (not including dual-cure composites) on the market, dentists are faced with a difficult situation when choosing the right brand. Since the introduction of the first light-curing composite in 1970, dentists have tried different materials and techniques to achieve successful restorations in a variety of clinical situations. Since setting up the composite is a very delicate process, there are some challenges associated with insulation, adhesion, material selection and polishing. Combining these factors with the high cost and imperfection of the insurance system, doctors have to work not only efficiently, but also efficiently. Dr. Ron Jackson summed up the challenges dentists face every day: “Given the current industry landscape, dentists must have the materials and techniques that allow them to perform posterior restorations faster, easier and more cost-effectively.”
Because of this, many physicians have combined certain materials and equipment to create "their own" Class II cavity repair system based on their own experience and clinical observations. However, this approach is not entirely compatible with the modern approach to dentistry, which includes three dominant features: the latest scientific achievements, the skills and objectivity of the doctor, and the individuality of each patient. With such a huge number of sources of information, such as articles and notes in magazines, web presentations, advice from consultants and representatives, the Internet, and the opinions of colleagues, it becomes increasingly difficult to understand which method or technique is actually worthy of attention.
The application of current dental literature in real practice is especially important when performing direct restorations. One example that illustrates this point is the promotion of Bulk-fill materials in publications to focus on polymerization stress rather than volumetric shrinkage. If we follow the opinions of the literature, then the use of Bulk-fill materials allows us to omit some stages when carrying out restorations, thereby restoring faster.
In addition, more recently, manufacturers have introduced systems and products designed to be used in a specific sequence to achieve consistently optimal results. An example of this is the 3M ESPE Trifecta Method for indirect restorations and DENTSPLY Caulk Class II for direct restorations.
The purpose of this article is to analyze the existing literature regarding flowable bulk-fill composites as materials that can reduce the stages of restoration, and also to highlight important factors that allow achieving high results when filling class II cavities.
Bulk-fill work with liquid materials
Shrinkage of a flowable material can compromise the success of the entire restoration and lead to poor marginal seal, microleakage, microfracture, and recurrent caries. If a fluid material is placed in a narrow space and then polymerized, polymerization stress very often develops. According to Hooke's law, stress is determined by the elasticity of the material under stress. In this case, shrinkage stress is transferred to the surrounding tooth tissue, since the elastic modulus (elasticity) of the tooth is much higher than the filling material. As a result of the transfer of shrinkage stress to the tooth, damage to its own tissues may occur. This can lead to postoperative sensitivity, microfractures, disruption of the adhesive layer, microleakage and recurrent caries, as well as loss of marginal seal. Several factors have been identified as influencing the shrinkage stress of a restoration: the size and geometry of the restoration (C-factor, depth and diameter), the materials used and the curing protocol.
The layer-by-layer filling technique has been proposed to reduce the shrinkage stress of composite materials. More recently, there have been major disagreements among scientists on this issue. Versluis and Abbas showed that minimizing deformation and deflection can be achieved using a bulk-fill technique. Lee and Park argue that layered application is a successful solution for controlling polymerization stress. Despite the varying conclusions, layering is generally the recommended technique preferred by many dentists, taking into account additional factors such as depth of cure, adaptation and adequate formation of the bond layer.
The new category of bulk-fill flowable composites claims to work effectively with a 4 mm layer, as well as reduced polymerization shrinkage. The first liquid-flow material Bilk-fill (Superfil SDR flow DENTSPLY Caulk) was introduced in 2009 (Photo 1). There are currently 4 bulk-fill flowable composites on the market: Superfil SDR flow, Filtek Bulk Flow (3M ESPE), Venus Bulk Flow (Heraeus Kulzer) and x-tra Base (VOCO America).
Photo 1: Liquid Superfil SDR (Dentsply Caulk)
Ilie and Hickel studied Superfil SDR in comparison with other materials and found that Superfil shrinkage was 1.1 mPa, while Esther-X (Dentsply Caulk) and Filtek Supreme Plus Flow (3M ESPE) were 5.3 mPa and 6.5 mPa respectively. The authors hypothesized that part of the reduced shrinkage of Superfil SDR is due to slow polymerization and greater fluidity. Compared to other composites, Superfil SDR shows the lowest hardness, which can be explained by its lower volumetric fill (44%). For this reason, the Superfil SDR flow instructions recommend covering the occlusal portion with 2 mm of universal restorative material.
The C-factor is determined by the stresses created by the cavity configuration in relation to bonded and uncoated surfaces. According to Feilzer: the higher the C-factor (the more bonded surfaces), the higher the stress generated (eg classes I and II). Conversely, cavities with more unbonded surfaces result in less shrinkage stress (Class III and IV cavities). Two recent studies have also suggested that cavity depth and cavity diameter may influence shrinkage, thereby affecting microleakage. By studying the effect of bulk-fill filling of cavities with a high C-factor with liquid materials with low shrinkage (Superfil SDR flow), Van Ende, la Macorra and Gomez-Fernandez proved that a 4mm layer does not reduce adhesive strength due to shrinkage stress. The authors concluded that the bulk-fill technique is desirable for high C-factor restorations, and dentists in such situations should use low-shrinkage materials to avoid debonding and microleakage. These findings were in agreement with those of Roggendorf, who indicated that it was possible to use low-shrinkage bulk-fill materials in the open sandwich technique without negatively affecting the edge seal.
Stages of Class II restoration
Insulation
The gold standard for isolating prepared teeth before placing composite material is a rubber dam. However, in the case of Class II cavities, isolation using matrices becomes difficult. The matrix system should not only help achieve marginal sealing, but also follow the anatomical contour of the tooth and recreate interproximal contact. Historically, circular matrices (Tofflemire Type, AutoMatrix) have been used in such situations, but they are not an ideal option. While they are quite effective at isolating the prepared tooth, Tofflemire matrices are of little use in creating proper contact, which then results in food retention in the dental space.
In 1986, BiTine sectional matrices (Darway Dentsply Caulk) were introduced, which made it possible to create more accurate contacts in class II. Nowadays, sectional matrix systems such as Palodent Plus (Dentsply Caulk), V3 (Triodent) and Composi-Tight 3D (Garrison Dental Solutuions) are designed to overcome all the disadvantages of circular matrices and the disadvantages of BiTine systems (for example, tooth separation, ring placement and stabilization, prevent the ring from slipping) (Photos 2 and 3). In addition, the sectional ring matrix systems mentioned all include anatomical wedges for improved creation of precise interproximal contact. Figure 4 shows a radiograph of a Class II composite restoration performed with a circular matrix and wood wedge, and a sectional matrix system and anatomical wedge.
Figure 2: BiTine (Darway/Dentsply Caulk) sectional matrix system placed in the mouth to restore tooth #4. Please note that the ring helps adapt the matrix to the tooth wall, but does not contact the adjacent one and does not improve separation to create the correct contact point.
Photo 3: Palodent Plus Sectional matrix system (Dentsply Caulk)
Figure 4: Radiograph showing the upper premolar restored using a circular matrix and a triangular wood wedge. The lower premolar was restored using the Palodent Plus Sectional matrix system and anatomical wedges. Note the more regular gingival contour and contact point of the lower tooth.
Adhesion
Since 1955, Buonocore's acid etching technique has made adhesion to enamel quite successful. However, achieving optimal bonding to dentin remains a highly challenging procedure due to microleakage, material infiltration and penetration, hydration, and postoperative sensitivity. To eliminate these factors, the evolution of dentin bonding has switched from a full-etch technique, meaning the application of 30% or 40% phosphoric acid to the enamel and dentin, to a sapro-etch technique, where phosphoric acid esters are contained in the bonding agent, and there is no separate application of the etching gel to the tooth.
Recently, a third technique has emerged that promotes hybridization of the remaining smear layer of dentin and acid-etches the enamel to maximize bonding force and prevent marginal leakage. The selective etching technique is designed to enhance the positive aspects of both techniques and produce an optimal final result. In two recent studies, a meta-analysis conducted by Heintze and Rousson concluded that the best results are obtained with a rubber dam filling and enamel etching technique. At the time of writing, there are 3 universal adhesives on the market that can be used in all three techniques: Prime&Bond Elect (Dentsply Caulk), Scotchbond Universal Adhesive (3M ESPE) and All-Bond Universal (Bisco Dental Products).
Composite
The placement of composite material involves a precise and strategic process. Challenges for the clinician include: appropriate adaptation of the material to the prepared tooth, choice of bulk-fill versus layer-by-layer technique, polymerization shrinkage and stress of the material, depth of cure, and handling of the material itself.
Historically, doctors have used flowable composites as linings in class II cavities because of their good penetration ability and adaptation to cavity walls. However, the use of flowable material for marginal sealing in class II cavities remains a controversial issue. Some studies report a reduction in microleakage with the use of flowable composites along the gingival margin, while others criticize this practice. There is an opinion that the localization of cavities at the gingival margin above or below the cemento-enamel junction is the best test for filling material. In these studies, GIC appears as a material with good adhesive properties and low shrinkage compared to fluid materials.
Since the currently available flowable Bulk-fill composites are not desirable for use on occlusal surfaces, a final layer of conventional restorative material is required. To simplify the selection of a material that can provide good results in all clinical situations, Dentsply Caulk introduced TPH Spectra Universal Composite (Photo 5). This new composite is based on TPH3 technology and contains nano-hybrid and micro-filled components. The result is a composite that has proven itself well in both restorations in the anterior and posterior segments. It has a transparency similar to natural teeth, high-quality polishing ability, color stability and wear resistance. TPH Spectra is also available in two versions: a creamy low-viscosity formula and a high-viscosity formula. For two viscosity options, the physical properties are absolutely the same. Since consistency is a very individual and subjective indicator, dentists have the opportunity to make a choice for each specific clinical situation.
Photo 5: TPH Spectra (Dentsply Caulk)
Polishing
The final step to achieve excellent clinical results when filling class II cavities is contouring with the tip at high speed, followed by finishing and polishing of the restoration. The polishability of a material is based on filler type, shape and composition. Recent studies have shown that hybrid and microfilled composites improve esthetics and extend the life of the restoration by reducing stainability, preventing microbial accumulation, inflammation of the gingival margin and wear of the filling. The Berger study looked at 3 composites and polishing systems (Dentsply Caulk, 3M ESPE and Cosmedent) supplied by the same manufacturer. According to the authors, for the best possible polishing of composites, polishing systems from the same manufacturers as the materials should be used.
In 2009, the names of polishing systems rated as good or excellent were published:
Super-Snap Rainbow Technique Kit (Shofu Dental), Enhance (Dentsply Caulk), FlexiDisc (Cosmedent) and OptiDisc (Kerr).
Clinical cases
Clinical case 1
A 32-year-old woman came to the clinic. Upon examination, an open interproximal cavity was revealed, in which food retention occurred, in the tooth on the lower jaw on the left. The cavity was formed due to a fracture of the composite on the disto-occlusal side of tooth No. 20. The patient desired restoration and closure of the cavity (Figure 6).
Photo 6: Tooth No. 20 before preparation, inadequate condition of the filling on the disto-occlusal side
After local anesthesia with a carpule of 4% articident with epinephrine 1:100,000 (Dentsply), the existing filling was removed with tips at high and low speeds, and a Snoop Caries Detector (Pulpdent) was used to detect caries (Photo 7).
Figure 7: Completed disto-occlusal preparation, checking Snoop Caries Detector (Pulpdent)
After placing the rubber dam, the entire prepared surface was etched with 34% phosphoric acid gel for 20 seconds, then thoroughly rinsed with water. Isolation of the prepared tooth was performed by Palodent Plus (Photo 8). Prime&Bond Elect was rubbed into the cavity for 20 seconds, then air-dried for 5 seconds to remove the solvent. The bonding agent was light cured for 20 seconds (Photo 9).
Photo 8: Isolation of tooth #20 using the Palodent Plus Sectional matrix system
Photo 9: Application of Prime&Bond Elect (Dentsply Caulk) - universal adhesive
The first layer of Superfil SDR was applied to the cavity and then cured for 20 seconds (Photo 10). TPH Spectra low viscosity shade A2 is applied in a 2 mm layer and also cured (Photo 11).
Photo 10: Adding No. 20 Superfil SDR into the tooth cavity using a special tip
Photo 11: Low viscosity TPH Spectra Universal Composite was applied as the final occlusal layer.
The resulting restoration was finished and polished with Enhance and PoGo (DEntsply Caulk) (Photos 12 -14).
Photo 12: Tooth No. 20 after filling
Photo 13: Palodent Plus Pin Tweezers (Dentsply Caulk) are used for easy matrix removal.
Photo 14: After finishing and polishing, final appearance of tooth No. 20
Clinical case 2
A girl came to the clinic complaining of a missing filling. Intraoral examination revealed that the disto-occlusal amalgam filling on tooth #12 had fallen out (Figure 15). The patient did not report pain, but reported sensitivity when drinking cold drinks. After clarifying the medical history and evaluating the radiographs, it was decided to perform a direct restoration with composite material.
Photo 15: Preparation of tooth No. 12
Anesthesia was performed with a carpule of 2% xylocaine with epinephrine 1:100,000 infiltration from the buccal side. Preparation was carried out with a carbide bur at high speed and a round bur at low speed. Complete removal of carious decay verified by Snoop Caries Detector.
Due to the depth and size of the cavity obtained after preparation, it was decided to use the selective etching technique with Prime&Bond Elect. The technique was chosen for maximum adhesion to enamel and minimal etching of dentin. The enamel was etched with 34% phosphoric acid and then washed with water (Photo 16). Prime&Bond Elect was rubbed into the surface for 20 seconds, air dried for 5 seconds and light cured for 20 seconds (Photo 17). Isolation was carried out by Palodent Plus (Photo 18). The shade of the teeth is approximately defined as A2 according to the VITA Classic (Vident) scale. TPH Spectra high viscosity shade A2 is placed in a 2 mm layer (Photos 19 and 20). Each layer of composite is cured for 20 seconds.
Photo 16: Selective etching of tooth enamel No. 12
Photo 17: Tooth #12 is isolated with the PalodentPlusSectional matrix system. Due to problems with mouth opening, a rubber dam was not applied to this patient.
Photo 18: Prime&BondElect was rubbed onto the prepared surface of tooth No. 12
Photo 19: High-viscosity TPHSpectra introduced into the cavity
Photo 20: Tooth No. 12 after curing of the material before removing the matrix
The final restoration is finished and polished to achieve precise shape and contour. After checking the occlusion, the composite was polished with Enhance and PoGo (Photo 21).
Photo 21: Final view of the restoration of tooth No. 12
Final comment
Modern restorative materials can provide superior results when applied in a careful and precise manner. Creating systems that provide step-by-step instructions can greatly assist dental practitioners. This approach already exists in implantology, orthopedics, and now it has been created in the therapeutic section, making it possible to achieve the highest possible results when filling class II cavities.
Posted by Jason H. Goodchild, DMD
Differences between chronic caries and acute
Let's take a closer look at the features of the chronic and acute forms of this disease.
The acute form of caries is characterized by the rapid development of destructive changes in the hard tissues of the tooth, the rapid transition of uncomplicated caries to deep caries.
The affected tissues are soft, slightly pigmented (light yellow, grayish-white), moist, and can be easily removed with an excavator.
Chronic caries is characterized as a slow process (several years).
The spread of the carious process (cavity) is mainly in the planar direction. The altered tissues are hard, pigmented, brown or dark brown in color.
Clinical principles for preparing carious areas
To carry out all the necessary therapeutic manipulations, many specialists rely in their work on Black’s classification of caries.
For any of the above types of tooth damage from caries, it is necessary to carry out full preparation and filling.
The durability of your tooth (or several) depends on the quality of these manipulations.
Experienced dentists, when removing soft carious dentin, can leave its deep pigmented elements to avoid damage to the tooth pulp. After carrying out this work, there should be no affected tissue left on the walls of the cavity.
At all stages of preparation and filling, the dentist sets the main goal - to destroy the carious areas of the affected tooth, disinfect the remaining parts and apply a hermetically sealed structural material that can restore the structure of the tooth and help it fully perform its functions in the future.
Type of caries according to degree of activity
There are 3 types of caries in this category: compensation, subcompensation and decompensation.
Compensatory caries is characterized by a slow or non-progressive process.
Damage to the surface of the teeth is insignificant and does not cause any discomfort in the patient.
With regular and systematic hygiene procedures, as well as special preventive measures, it is possible to stop the development of the disease at its initial stages.
Subcompensatory caries is characterized by an average rate of progression, at which it can go unnoticed and not cause concern to the patient at all.
Decompensation caries is expressed by intensive development and dynamics of progression, accompanied by such acute pain that it affects both the patient’s ability to work and everyday life.
Because of this, the disease is often called acute caries. It requires immediate treatment procedures, since otherwise the process may spread to third-party teeth with the subsequent addition of pulpitis and periodontitis.