The dental organs are an integral part of the masticatory apparatus.
The chewing apparatus of an adult contains 32 dental organs (16 each in the upper and lower jaws).
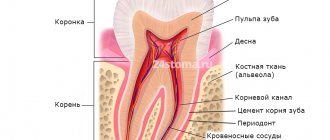
The dental organ consists of a tooth; the socket and the adjacent jaw, covered with the mucous membrane of the gums; ligamentous apparatus that holds the tooth in the socket; vessels and nerves.
In the tooth there are:
- crown (thickened part protruding into the tooth cavity);
- neck of the tooth (narrowed part adjacent to the crown, surrounded by gum);
- root (part of the tooth located inside the jaw socket).
TOOTH PULP
There is a cavity inside the tooth that resembles the shape of a crown, and at the root of the tooth it continues in the form of a canal. The root canal ends at the apex of the tooth root with an opening. The tooth cavity is filled with loose connective tissue, rich in blood vessels and nerves - pulp. The dental pulp is divided into crown and root parts. The pulp of the tooth crown is represented by loose connective tissue with a delicate network of collagen and precollagen fibers with a large number of cellular elements. In the tooth root pulp, collagen structures are denser, thicker and oriented longitudinally along the neurovascular bundle.
Based on the cellular composition of the pulp, they are divided into: peripheral, subodontoblastic and central layers.
The peripheral layer consists of specialized cells - odontoblasts, which take part in the metabolic processes of enamel and dentin. They are located in several rows.
The odontolast has an elongated pear-shaped shape. It has a peripheral protoplasmic process (or dentine), which runs in the dentinal tubule to the dentinoenamel junction, and short lateral processes that anastomose with neighboring cells in the early stages of differentiation.
The subodontoblastic and central layers consist of small, poorly differentiated stellate cells connected to each other by short processes. The pulp contains many fibroblasts that participate in the formation of a fibrous capsule that limits the focus of inflammation.
In the central layers there are cytoplasmic cells - histiocytes. During inflammation, they acquire the ability to move and phagocytose and are called macrophages.
The blood supply to the pulp is provided by blood vessels that penetrate into it through the opening of the apex of the tooth root and through additional canals from the periodontium. The lymphatic system in the pulp is presented in the form of slits, capillaries, and vessels. The outflow of lymph from the pulp occurs in the submandibular and mental lymph nodes. Arterial trunks accompany veins. The pulp vessels have numerous anastomoses. Through the apical foramen, sensitive pulpy and non-pulse fibers of the trigeminal nerve pass, which innervate the pulp, forming plexuses.
The dental pulp has a trophic, protective and plastic function. The trophic function is carried out due to the developed network of blood and lymphatic vessels; protective - due to histiocytes, plasma cells; plastic is the participation of the pulp in the formation of dentin.
The bulk of the tooth is dentin, which surrounds the tooth cavity. In the area of the tooth crown, dentin is covered with bright white enamel. The dentin of the root is covered with cement.
Dentin diseases
Very often, the bone substance of the tooth is susceptible to a disease such as caries. When damage affects only enamel and dentin, the disease is classified as moderate. The process begins with damage to the surface layers of tissue, then a carious cavity is formed in which food debris accumulates, which provokes the onset of decay processes and further destruction of the tooth. A diseased tooth causes significant discomfort, reacting with acute pain to various irritants, but after their elimination, the pain stops. These signs should be a signal to visit the dental clinic as soon as possible and fix the problem. Otherwise, caries can reach the root of the tooth in a fairly short period of time. When the root is damaged, a deep form of caries occurs, in which there is a high risk of losing the tooth. In order to keep your teeth healthy for as long as possible, you must observe the following: 1. Perform regular high-quality oral hygiene. 2. Have healthy foods in your diet, enriched with vitamins and minerals. 3. Regularly undergo preventive examinations by a dentist to identify diseases at an early stage in order to prevent further destruction of dental tissues
PERIODONTIUM
The root of the tooth is held in the socket by connective tissue fibers that make up the root membrane or periodontium.
The periodontium is located in a narrow, slit-like space between the tooth root and the jaw bone. The thickness of the periodontium is 0.15-0.25 mm. With age, as well as from mechanical load, the thickness of the periodontium changes and amounts to 1.2-1.2 mm.
The basis of periodontal connective tissue are bundles of interdental and cemento-alveolar fibers, which are woven, on the one hand, into the compact plate of the alveoli, and on the other hand, into the cementum of the tooth root. In the area of the tooth neck, fibrous fibers have an almost horizontal direction and include numerous collagen fibers, circularly covering the cervical area (circular ligament). The apical periodontium contains more loose connective tissue and cellular elements. Fibrous fibers in the area of the tooth apex are represented by looser, more delicate bundles and are arranged radially; with the help of the fibers, the tooth is suspended and fixed in the bone bed.
The blood supply to the periodontium is abundant and it has a fairly developed lymphatic network. Periodontal vessels form several plexuses (external, middle, capillary) in the root area. Cellular elements are represented by fibroblasts, mast cells, plasma cells, histiocytes, cementoblasts, osteoblasts, and epithelial remnants of the neoplastic epithelium. The main function of the periodontium is support and retention. In addition, the periodontium distributes and regulates pressure on the tooth (shock absorbing), has a plastic function due to cellular elements and a barrier function (due to the unique anatomical structure and resistance to adverse environmental influences). The reflexogenic function of periodontium is also highlighted.
New aspects of assessing dental morphology
To achieve excellent aesthetic results from dental treatment, it is necessary to understand in detail the morphological features of each tooth, which influence both the stage of restoration and the stage of tooth preparation. Minimally invasive ceramic restorations have a high success rate, but their effectiveness is much higher when bonded to enamel rather than dentin. Research data demonstrate that veneers bonded to dentin have a 10% lower success rate than veneers bonded to enamel. Therefore, before carrying out preparation, the doctor must clearly understand the thickness of the enamel in different areas, so as not to compromise the future result of treatment. This aspect of treatment has become even more relevant, given the general trend towards the prevalence of minimally invasive interventions. Minimally invasive approaches make it possible to preserve the original volume of tooth tissue to the greatest extent. On the other hand, the implementation of minimally invasive treatment approaches is simply impossible without a holistic understanding of the characteristics of tooth morphology.
Minimally invasive preparation
Several studies have demonstrated that preserving the enamel, especially its edges, significantly increases the strength and fracture resistance of ceramic restorations, and also significantly reduces the risk of their failure. To control the depth of preparation, you can use special burs to mark the preparation grooves. The amount of tissue reduction required also depends on the type of material used and the shade of the tooth for which the restoration is being made. Changing the shade of a tooth by one order of magnitude requires tissue preparation with a thickness of 0.2 mm to 0.3 mm. For example, to change the shade of a tooth through restoration from A2 to A1, it is necessary to ensure a reduction of 0.3 mm of the tissue layer, and when moving from A4 to A1 - 0.9 mm of the enamel thickness (photo 1). However, as shown in polarized photographs of incisor sections (Figure 2), the thickness of the enamel is variable in different areas. The average enamel thickness on the outer surface of the incisor varies from the apical third (approximately 1.0 mm) to the middle third (approximately 0.9 mm) to the cervical third (approximately 0.3 mm) (Figure 3).
Photo 1. Illustration of the required amount of preparation when correcting tooth shade.
Photo 2. Polarization photograph of a section of the central incisor.
Photo 3. Average enamel thickness in different areas of the incisor.
Without understanding this specificity, even with the use of marking burs, it is impossible to ensure proper preservation of enamel tissue. It is also necessary to understand that in most cases, when we prepare a tooth for a veneer, its contour will accordingly be slightly changed, based on aesthetic needs. This means that in some areas we will have to carry out minimal reduction, and in others – more pronounced. The ideal concept for planning an intervention is to be outcome-oriented - the clinician should always remember what he wants to achieve in the end. For this purpose, it is advisable to produce a composite reproduction of the final restorations and use it as a guide during the preparation of the teeth. In this way, better control over the preparation depth can be achieved.
Basics of dental morphology
It is clear that clinicians must understand tooth morphology during preparation, but how important is this morphology for future restorations? The goal of cosmetic dentistry is to improve the visual profile of teeth, correcting their color, shape, position, size and relationship with other units of the dentition. Despite the fact that today there is a huge amount of materials available for performing aesthetic restorations, the role of tooth morphology in the selection of such restorations has not yet been canceled. According to Kataoka and Nishimura, to recreate an esthetically acceptable tooth contour, dentists must consider three basic elements of morphology. The first element combines three variants of the geometric shape of the tooth: square, ovoid (conical) and triangular. The second element involves taking into account secondary anatomical features, that is, individual lobes. These are formed as a result of the normal development of the tooth, and can be represented by variants of depressions and undulations, which form the unique contour of the crown. The third element involves tooth texture. Changing the reflective surface can greatly affect the appearance of the crown. Essentially, tooth texture is an element of secondary anatomy that is determined by the physical characteristics of the enamel, including the presence of vertical lobes, horizontal and cervical ridges, or perikymata. Perikymata and other more variable forms of the enamel surface usually occur in young patients. The loss of such unique features in older age develops due to the phenomenon of physiological abrasion, due to which the shape of the teeth is leveled over time. Also, the shape of the tooth surface also affects how light interacts with it: if the shape of the tooth is convex, then it seems more glossy, but if, on the contrary, it is concave, then it appears matte (photo 4).
Photo 4. The tooth has a glossy appearance in areas of convex surfaces, and a more matte appearance in areas of concave surfaces.
The ability to recreate adequate tooth texture is an important factor in mimicking natural tooth morphology, which should be considered when using different restorative materials. Elgendy et al demonstrated that no composite resin technique adequately reproduces tooth morphology when considering the criteria of long-term color stability and optical performance of the restoration.
Creating cosmetic illusions
The main tool for recreating the most natural restorations is the ability to control the optical characteristics of the restoration and the predictability of interaction with light. We perceive objects depending on how light is reflected or reflected from them. The same principle can be used when correcting the shape and size of a tooth crown. Even though the shape of the anterior teeth itself is extremely important, elements of morphology such as the lines and angles that form at the contact sites remain equally significant. The more distal or mesial the lines of the angles of transition from the vestibular surface to the contact surface are located, the flatter the contact zones appear, and the visually wider the tooth appears. For example, a patient came in after pretreatment with composite veneers with the complaint that his teeth looked overly wide (Figure 5). He was worried that ceramic veneers would not look the same. The green and red lines in the photo demonstrate the relationship between the lines of the angles of transitions into contact zones, due to which the visual perception of the tooth shape may change.
Photo 5. Comparison of lines of transition angles into contact surfaces in the case of composite and ceramic veneers.
Understanding all the possibilities for recreating cosmetic illusions plays an important role in the process of closing diastemas. In the absence of orthodontic treatment, closing diastemas with ceramics or composites often causes teeth to appear too wide. In the case depicted in Figure 6, the patient sought dental attention regarding a space between his central incisors. After refusing orthodontic treatment, the decision was made to perform two composite restorations to close the diastema. The choice of composite instead of ceramics allowed us to minimize the amount of hard tissue reduction. By forming adequate transition zones, the doctor was able to achieve an aesthetically acceptable effect of closing the diastema while implementing a minimally invasive approach to the intervention (photo 6). Thus, using the capabilities of cosmetic illusions allows you to achieve effective results even in situations that previously seemed extremely difficult from the point of view of their clinical solution.
Photo 6. View before and after treatment of diastema without the use of orthodontic intervention methods.
Probably the most important aspect of aesthetic restoration remains its form. Of course, the shade can also affect the perception of the size and appearance of the crown: the brighter the tooth, the larger it appears in size. You can see this effect in photo 7, where the same tooth was photographed at different brightnesses. This is one of the most powerful tools for creating the illusion of shape. It is also necessary to remember that the height of the tooth also affects the perception of its width. If you take two teeth of the same width, the taller one will appear less wide. This is why taller people appear thinner. This phenomenon is demonstrated in photo 8 - adding a small amount of length creates a narrower appearance of the tooth.
Photo 7. Change in the visual size of teeth when changing the brightness level.
Photo 8. Photo before and after a slight correction of the length of the incisal edge: in the photo after, the teeth look narrower.
conclusions
The success of aesthetic dental treatment is determined by three main factors: tooth color, shape and texture. Understanding the principles of optical illusion can significantly influence the final success of iatrogenic interventions. The application of biological principles during dental treatment allows us to minimize the amount of targeted tissue reduction and, thus, contributes to achieving the most natural appearance of ceramic restorations. In addition, minimizing the depth of preparation also has a positive effect on the long-term functioning of various types of orthopedic structures. Using the principles of optical illusion, dentists can recreate different tooth shapes by adjusting only optical or minor geometric characteristics. This allows you to recreate the contour of teeth longer or shorter, narrower or wider, while adjusting only minor details of texture. Most patients are unhappy with the appearance of their smile, but they refuse orthodontic treatment. Dental materials available today will allow you to choose the most biologically and functionally enhanced approach to restoring the shape of individual teeth and the profile of the smile as a whole, including through direct composite restorations or ceramic veneers with minimal or no need for preparation.
Author: Adamo E. Notarantonio, DDS
DENTINE
Dentin in its structure resembles coarse-fibrous bone tissue, consisting of a basic substance penetrated by a large number of dentinal tubules. The main substance of dentin consists of collagen fibers, between which there is an amorphous adhesive substance. The outer layer of dentin (with a radial arrangement of fibers) is called mantle; the inner layer with a tangential arrangement of fibers is peripulpar. Dentinal tubules (tubules) have the shape of round, oval tubes. They begin in the tooth cavity, bending in a wave-like manner, pass through the thickness of the dentin and end in flask-shaped swellings in the area of the dentino-enamel junction.
In the lumen of these tubules there are dentinal processes of odontoblasts. Dentin contains 70-72% inorganic substances (mainly phosphate and calcium carbonate), and 28-30% is water and organic matter (proteins, fats and carbohydrates).
Tooth enamel Tooth enamel is the hardest tissue of the human body. In the area of the cusps of the tooth crown there is the thickest layer of enamel; towards the cervical area the thickness of the enamel decreases. Enamel prisms are the main structural formation of enamel. The enamel prism is a faceted cylindrical fiber that begins at the dentinoenamel junction.
It bends in an S-shape, runs radially and ends on the surface of the tooth crown. Enamel prisms are connected into bundles (10-20 each), directed radially from the dentinoenamel junction to the outer surface. The thickness of the prisms is from 3 to 6 microns. Each prism contains thin cytoplasmic fibers that form an organic mesh, in the loops of which crystals of mineral salts are located.
Enamel prisms and interprismatic spaces (in electron microscopic examination) consist of strictly oriented hydroxyapatite crystals arranged in a certain order, the length of which ranges from 50 to 100 nm.
Most of the tooth enamel consists of inorganic matter (95%), organic (1.2%) and water (3.8%). Tooth enamel contains 96.5% mineral salts, of which about 54% are phosphorus and calcium (17% and 37%, respectively), which are represented by hydroxyapatite crystals.
Tooth structure
A tooth is an organ located in the alveoli of the jaws. A tooth consists of a crown part, a root and a neck connecting the crown to the root. According to the morphological composition, the tooth is divided into hard and soft tissues. Enamel covers the coronal, that is, visible, part of the tooth. It is the hardest element in the human body. Under the enamel is the bone tissue of the tooth, or, as it is also called, dentin, which has a soft and porous structure. The root under the gum is covered with a shell of cement, and in the cavity of the tooth there is pulp, soft tissue consisting of blood vessels and nerve fibers. They penetrate the porous structure of dentin, reaching the beginning of the enamel. This explains the high sensitivity during sudden temperature changes in the oral cavity, as well as when interacting with other unfavorable factors.
TOOTH CEMENT
The cementum of the tooth covers the root and is divided into primary and secondary. Primary (cell-free) cement is adjacent directly to dentin, covering the lateral surfaces of the tooth root. Secondary (cellular) contains cementocides, covers a layer of primary cement, is localized only in the area of the root apex and on the interroot surfaces of premolars and molars.
The main substance of cement is represented by collagen fibers running in different directions, most of which run in the radial direction. In some pathological conditions, hypercementosis is observed (excessive deposition of layers of cement on the surface of the tooth root). Cement consists of 68% inorganic and 32% organic substances.