GBOU "NIKIO im. L.I. Sverzhevsky" of the Moscow Department of Health
Hypertrophy of the lingual tonsil
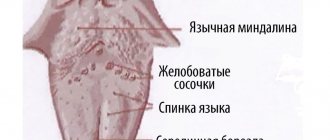
The lymphadenoid tissue of the root of the tongue is presented in the form of two clusters of large follicles located in rows or in random groups. These clusters are separated by a central groove extending from the middle of the lingual epiglottis fold to the largest, final, circumvallate papilla on the root of the tongue. Therefore, it is more correct to talk about not one, but two lingual tonsils. The number of large follicles in a 1-year-old child is 10-12, and in a 5-year-old child it is 20-30. At the age of 35 to 40 years, the maximum number of follicles (35-40) is observed with a simultaneous increase in their size. After 45 years, the number of follicles decreases and the size of each of them decreases (A.I. Tseshinsky, 1951).
One must think that the main cause of hypertrophy of the lingual tonsil in adulthood is inflammatory processes in the oropharynx. In some cases, hypertrophy of the lingual tonsil develops as a compensatory process in individuals who have had their palatine tonsils removed (B. S. Preobrazhensky).
Symptomatology and diagnosis of hypertrophy of the lingual tonsil.
Severe enlargement of the lingual tonsil can cause mechanical difficulty in breathing and voice production. Such cases, however, are very rare. Typically, patients with hypertrophy of the lingual tonsils complain of a feeling of pressure projected into the area of the hyoid bone, a sensation of a foreign body in the throat, cough, and sometimes laryngospasm . These complaints are not pathognomonic for hypertrophy of the lingual tonsil. Therefore, their assessment requires caution. Sometimes patients with hypertrophy of the lingual tonsils complain of coughing paroxysms. In such cases, mechanical irritation of the lingual tonsil using a probe can provide some assistance in diagnosis. If cough occurs only when the lingual tonsil is irritated, then it seems likely that it is the receptive field of the cough reflex.
When making a differential diagnosis, you need to keep in mind the following diseases.
- Inflammatory processes in the area of the root of the tongue. They can be caused by a banal infection (abscesses and phlegmon of the root of the tongue), tuberculosis, syphilis and various fungi (actinomycosis, coccidioidomycosis, blastomycosis, moniliasis). These diseases differ from hypertrophy of the lingual tonsil by the asymmetry of the lesions, their greater density and more saturated color. Histological (biopsy), serological and bacteriological examination helps.
- Tongue root cysts. In this area, there are retention cysts of the mucous glands and very rarely - cysts formed from elements of the thyroglossal duct. They are distinguished by a smooth-stressed surface.
- Benign tumors - adenomas and mixed tumors of the salivary glands are more common. They are also distinguished by their smooth surface and significant density.
- Malignant tumors - cancer and lymphoepithelial tumors are usually observed. Diagnosis is simple for ulcerated tumors.
- The goiter of the tongue root is distinguished by a pink, smooth surface covered with a network of highly developed venous vessels. It has a significantly higher density than hypertrophied lymphadenoid tissue. In some cases, the thyroid gland is absent in its usual place, which can be confirmed by palpation of the neck in thin individuals. Research with radioactive iodine helps, which, after ingestion, is concentrated in the thyroid tissue, as a result of which strong gamma radiation is detected in the area of the root of the tongue.
Treatment of hypertrophy of the lingual tonsil.
With moderate hypertrophy, patients are prohibited from smoking and eating spicy foods. Sometimes alkaline rinses and lubrication with iodine-glycerin are beneficial. Some authors recommend cauterization with lapis and galvanocauter. The use of radiation therapy has been proposed. With severe hypertrophy of the lingual tonsil, its surgical removal is indicated. It can be removed piece by piece by “biting” under the control of a laryngoscopic mirror. Some authors prefer to perform complete enucleation of the lingual tonsils along with the capsule. Such intervention is especially advisable in cases where there are significant inflammatory changes in the hypertrophied lingual tonsils or if these tonsils are the cause of repeated phlegmonous inflammation in the area of the root of the tongue, damage to the kidneys, joints and other organs. Before the operation, a detailed clinical examination of the patient is necessary, studying the blood picture, its coagulability, counting the number of platelets, etc.
We perform removal of the hypertrophied lingual tonsil using a holmium laser (Ho:YAG) with a radiation power of 4.8 W (energy - 0.6 J, frequency - 8.0 Hz).
Hypertrophy of the palatine tonsils
Classification
There are three degrees of enlargement of the palatine tonsils:
- First degree - a third of the distance from the edge of the palatine arch to the uvula is blocked.
- Second degree - lymphoid tissue fills two-thirds of the space.
- Third degree - the tonsils “meet” at the uvula and touch each other.
According to the forms of the disease, they are distinguished:
- Hypertrophic form (physiological and age-related anomalies).
- Inflammatory form (bacterial infections).
- Hypertrophic-allergic form (accompanied by allergic symptoms).
Symptoms
The earliest manifestations of the disease are discomfort when swallowing and a feeling of a “lump in the throat.” Then there is difficulty in nasal breathing, sleep disturbance, snoring, whistling noise when breathing, coughing and mouth breathing.
With hypertrophy of the second and third degrees, the mobility of the soft palate decreases, articulation is impaired, nasal sound, slurred speech, and distortion of words appear. The patient constantly breathes through the mouth, since the choanae are blocked by the tonsils and swollen mucosa. Attacks of night apnea (stopping breathing during sleep) appear. Hearing progressively worsens.
Complications
All complications are associated with impaired patency of the Eustachian tubes and choanae. Violation of the outflow of secretions from the nose provokes the addition of a bacterial infection in the air cavities and middle ear.
Due to discomfort during swallowing, dysphagia appears, manifested by weight loss, vitamin deficiencies and gastrointestinal disorders. Due to chronic lack of oxygen, the nervous system suffers.
Diagnostics
The diagnosis is made by an otolaryngologist based on the following information:
- Complaints and anamnesis.
- Pharyngoscopy (size, color, nature of the surface and consistency of the tonsils).
- Clinical blood test (increased leukocytes, eosinophils, accelerated ESR).
- X-ray of the nasopharynx (degree of lumen overlap).
Differentiation is carried out with tonsillitis, lymphosarcoma, tonsillitis, intratonsilal abscess.
Treatment
Therapy depends on the degree of enlargement of the tonsils and is divided into several stages:
- Drug treatment: Treatment of mucous membranes with antiseptics
- Lymphotropic drugs.
- Ozone therapy
The prognosis for life and health is favorable. After the operation, recovery is rapid, breathing and speech return to normal. In children, first-degree hyperplasia may disappear on its own as the child grows. Specific prevention has not been developed.
Article:
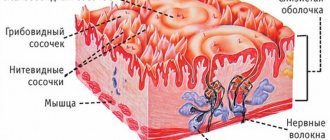
The tongue is a small muscular organ of the human body.
The tongue is located at the bottom (lower wall) of the oral cavity and, with the teeth closed, almost completely fills it, while in contact with the hard palate, gums, and teeth. Anomalies of the tongue can be either congenital or acquired; they are often the result of certain pathological processes occurring in the body. Currently, malformations of the main speaking organ are quite rare. Many of them are serious problems that often require surgery.
- Genetic diseases . May be inherited or develop as a result of new mutations, diseases such as: Beckwith-Wiedemann syndrome, Down syndrome, Sotos syndrome, hereditary mucopolysaccharidosis
- Exogenous factors . This group of reasons includes exposure of the fetus to ionizing radiation, carcinogens, chemicals, radioactive radiation, and pesticides in food products consumed by a pregnant woman. The development of maxillofacial anomalies is facilitated by bad habits of parents (drinking alcohol, drugs, smoking), and the expectant mother taking medications with teratogenic effects (this is a drug composition that is prohibited during pregnancy).
- Endogenous factors . Include infectious and metabolic diseases of the pregnant woman: trichomoniasis, toxoplasmosis, viral infections, hypovitaminosis and hypervitaminosis A, hypothyroidism, etc. The number of congenital craniofacial dysmorphias increases in proportion to the mother’s age at the time of conception.
A generally accepted classification of tongue defects has not been developed.
Based on the main criteria (size, structure, method of attachment), anomalies can be divided into the following groups:
- Anomalies of size - macroglossia (hypertrophied tongue), microglossia (reduced tongue).
- Anomalies of structure/shape - aplasia and aglossia (absence of tongue), cleft tongue (double. Cleft tongue can be complete or incomplete.
- Anomalies of attachment - ankyloglossia. This anomaly limits the mobility of the tongue in the oral cavity, and, consequently, its functions.
- Combined anomalies – folded (furrowed, scrotal) tongue. Characterized by the presence of folds and grooves on the surface of the organ
Macroglossia - massive tongue. Such a tongue does not fit in the oral cavity and literally falls out of the mouth. The child develops an incorrect bite due to constant pressure on the dentition. Teeth imprints are visible on the lateral surfaces of the tongue. Due to the constantly open mouth, the mucous membrane dries out, which causes discomfort. This is also a big disadvantage for correct sound pronunciation and food intake. A dental surgeon comes to the rescue again; he performs an operation to reduce the muscle mass of the tongue, that is, plastic surgery.
Microglossia is characterized by underdevelopment and reduction in the size of the tongue. Depending on the severity of the defect, a disturbance in sucking occurs, and subsequently in speech. There are cases when the anomaly is asymptomatic. The small tongue is not able to take the desired articulatory position: the amplitude of its movements is too small. In the case of microglosia, a pediatric dental surgeon performs tongue plastic surgery. At what age? Only the doctor can decide this. After the operation there is a rehabilitation period and sessions with a speech therapist.
Aglossia is a rare anomaly in which the tongue is completely absent. With aglossia - the complete absence of an organ - the baby cannot suck, so this rare anomaly requires tube feeding
Ankyloglossia is a congenital anomaly that is discovered shortly after birth. It is characterized by partial or complete shortening of the lingual frenulum. The average length of the frenulum is 1.5 cm. Deviations from the norm (shortened or very short): 1. The frenulum is thin, almost transparent, but prevents the rise of the tongue. 2. The bridle is thin . Its anterior edge is attached close to the tip of the tongue. Because of this, when the tongue is raised upward, the tip bifurcates into a “heart”. 3. The bridle is a dense short cord. It is attached close to the tip of the tongue. The upward movement of the tongue is limited. When you try to stick your tongue out of your mouth, its tip curls up and the back of the tongue “bulges out.” 4. A dense short cord of the frenulum is tightly fused with the muscles of the tongue: attached almost to the tip of the tongue. All movements of the tongue are sharply limited. 5 . It is difficult to understand where the frenulum is and where the tongue is, they are a single whole . It seems that the tongue has fused with the bottom of the oral cavity. With such a language, it’s not only impossible to speak, it’s impossible to eat!
All these deviations from the norm in the structure of the hyoid frenulum will at first complicate the process of feeding the child, and subsequently will prevent the timely appearance of not only the sounds [P] - [P'], but also the whistling sounds [S], [Z], [C]; hissing [Sh], [F], [H], [Sh]; sonors [Y], [L], [L'], back-lingual [K], [G], [X].
Parents for the most part do not like to listen to arguments in favor of surgery on the hyoid frenulum. They rely on exercises that supposedly stretch the frenulum. A similar misconception is noted among speech therapists. We would like to disappoint you: the frenulum does not stretch during speech therapy work, although with the help of special articulation exercises you can significantly increase the mobility of the tongue, due to which the impression is created that something has “stretched” somewhere. In fact, the time for producing sounds is extended, wasting the energy of both the child and the speech therapist.
What else can a child’s tongue “tell” about?
Recently, children with “geographical language” have become increasingly common. The surface of such a tongue is covered with streaks of white, brown and pink colors, with outlines reminiscent of a map of the continents, hence the name. At the same time, the mucous membrane of the tongue is shiny, as if polished, and taste buds are faintly visible on it. This is the state of the tongue to talk about the need to visit an allergist and gastroenterologist . A visit to a speech therapist is also required. As a rule, the sensitivity of such a tongue and mobility are significantly limited, so it is necessary to carry out articulatory gymnastics and the production of certain sounds.
Sometimes the surface of the tongue is dotted with deep grooves “Folded tongue”, like wrinkles. A sort of old tongue. He is painfully dry and inactive, which negatively affects sound pronunciation. A similar feature occurs when there is a disruption in the endocrine system, so do not put off a visit to the endocrinologist.
Attention should also be drawn to the child’s too pale, loose and flaccid tongue. In such a language, muscle tone is reduced (hypotonicity), its movements are slow and unclear, and it is sometimes impossible for him to take the necessary articulatory posture to pronounce a particular sound. Hence the errors in sound pronunciation: “porridge in the mouth.”
If the tongue is too tense, which is why its back is upturned, like a “hump,” and in the protruded position the tongue turns blue, the tip of the tongue deviates to the side, there is hypertonicity. In both the first and second cases, the child should be shown to a pediatric neurologist; perhaps such phenomena are a consequence of birth trauma, encephalopathy or some other diseases.
Conclusion.
Language is a map of internal problems.
The noted anomalies in the structure of the articulatory organs have different effects on sound pronunciation.