Hyoid frenulum: trim or stretch?
The sublingual frenulum is a membrane that is located under the tongue and connects the tongue to the sublingual space.
How to determine whether the hyoid frenulum is long enough?
The hyoid ligament (frenulum) can be of different lengths in different people. Ask your child to lift his tongue up toward the hard palate. With a normal length of the hyoid frenulum, the child freely raises the tongue to the hard palate. With a short hyoid frenulum, the child cannot stretch the tongue forward and lift the tongue up to the hard palate. When the child pulls his tongue up, you will see how the hyoid ligament, limiting the rise of the tongue, stretches, becomes more pronounced, protrudes more prominently under the tongue, and becomes thinner.
Another reason that a child cannot lift his tongue up is that the child’s tongue muscles are not strong enough and are inactive. Then you will see how he cannot cope with his muscles, then the tongue trembles, deviates to the side, twitches, and falls down.
Normal: at 5 years of age, the frenulum in a stretched state should be at least 8 mm. The average length of the frenulum is 1.5 cm.
What does this mean?
Short hyoid frenulum:
- may cause difficulty in moving the tongue, as it does not allow it to rise high. In this case, the so-called “upper sounds” suffer, i.e. the pronunciation of sounds such as Ш, Ж, Ш, Ш, Р, Рь is disrupted;
- can lead to a displacement of the center of the tongue, its asymmetrical development and low mobility, which prevents the formation of the correct articulatory posture of some sounds;
- may also cause problems with sound pronunciation;
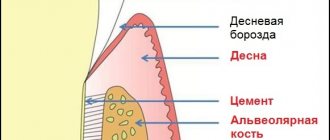
- in some cases, it can provoke problems with the formation of the lower jaw, i.e. The teeth may deviate and the necks of the teeth may become exposed. There is a risk of developing periodontitis and gingivitis. Therefore, a consultation with an orthodontist is necessary.
What to do?
1. Surgery
2. Stretching the hyoid frenulum
Even if the frenulum is somewhat shortened (equal to 8 mm), it is better to stretch it than to operate, since this procedure is somewhat painful and unpleasant for the baby!
Strong indications for trimming the hyoid frenulum:
1. It is better to trim the short frenulum of the tongue at an early age, up to one year.
Indications for surgery if the child while feeding:
• the child sucks poorly at the breast due to the fact that the shortened frenulum prevents the mother from tightly clasping the nipple;
• throws back his head;
• smacks and cries when sucking.
2. At an older age, the indication is when, due to a shortened frenulum, the child’s dentition shifts and an abnormal bite is formed.
3. Difficulties in pronouncing sounds; only in some cases does it require surgical intervention.
In 90% of cases, when 1-4 sounds are violated, the short frenulum of the tongue is easily stretched with the help of special articulatory gymnastics exercises.
Methods and techniques to stretch the hypoglossal ligament (frenulum)
MECHANISM OF EXERCISES for stretching the frenulum: since this is a fold (like a muscular one), a mucous fold, that is, it is possible to carefully and slightly correct the initial state of the frenulum, the exercises give the tongue the opportunity to rise up, thereby gradually stretching the muscle (it is quite elastic), these exercises It cannot be performed jerkily, it must be performed very smoothly and slowly.
Sounds that require a noticeable upward movement of the tip of the tongue ([р], [ш], [ж]) are placed after the child’s hyoid ligament is fully stretched.
Sounds ([l], [h], [sch], [t'], [d']) can be started when the frenulum has not yet fully stretched, but there is already some upward movement of the tip of the tongue.
A short frenulum does not interfere with the normal pronunciation of other sounds of the Russian language.
It is recommended to start stretching the frenulum at an early age. All children are recommended to do tongue exercises - this will help avoid a lot of problems at 5-7 years old (talking about pronunciation).
Causes of tongue abnormalities
Language defects are of a polyetiological nature. Anomalies are a consequence of intrauterine development disorders, which may be due to hereditary, endogenous and exogenous causes. All these factors affect the child in the early stages of embryogenesis.
The prerequisites for the occurrence of congenital pathologies of the tongue are:
- Genetic diseases
. They can be inherited or develop as a result of new mutations. Thus, macroglossia is characteristic of Beckwith-Wiedemann, Down, Sotos syndromes, and hereditary mucopolysaccharidoses; hypo- and aglossia - for Hangarth syndrome; folded tongue is a sign of Cowden's syndrome and hereditary keratoses, etc.
- Exogenous factors
. This group of reasons includes exposure of the fetus to ionizing radiation, carcinogens, chemicals, radioactive radiation, and pesticides in food products consumed by a pregnant woman. The development of maxillofacial anomalies is facilitated by the bad habits of parents (drinking alcohol, drugs, smoking), and the expectant mother taking medications with teratogenic effects.
- Endogenous factors
. Include infectious and metabolic diseases of the pregnant woman: trichomoniasis, toxoplasmosis, viral infections, hypovitaminosis and hypervitaminosis A, hypothyroidism, etc. The number of congenital craniofacial dysmorphias increases in proportion to the mother’s age at the time of conception.
Pathogenesis
The universal mechanisms of language developmental defects have not been determined. It is believed that the anomalies occur when the development of the first and second gill arches and the growth of the ligular primordia are disrupted. There is an opinion that at the end of the second month of intrauterine development of the fetus, the blood supply to the branchial arch changes. Until the 2nd month, blood comes from the internal carotid artery, and after that - from the external carotid artery. The period of changes in blood supply can be a trigger point in the formation of defects of the maxillofacial area in the presence of endogenous and exogenous aggravating factors.
Classification
There is no generally accepted classification of tongue defects in dentistry. Based on the main criteria (size, structure, method of attachment), anomalies can be divided into the following groups:
- Size anomalies
– macroglossia (hypertrophied tongue), microglossia (reduced tongue).
- Anomalies of structure/shape
- aplasia and aglossia (absence of tongue), cleft tongue (double tongue), goiter of the tongue root. Splitting of the tongue can be complete or incomplete. A goiter of the tongue is the location of the thyroid gland in the thickness of the root of the organ.
- Attachment abnormalities
- ankyloglossia. This anomaly limits the mobility of the tongue in the oral cavity, and, consequently, its functions.
- Combined anomalies
– folded (furrowed, scrotal) tongue. It is characterized by the presence of folds and grooves on the surface of the organ, due to which its size increases.
Diagnostics
Diagnosis of linguistic anomalies does not present any difficulties. The presence of serious malformations is determined by a neonatologist in the maternity hospital; less pronounced anomalies are diagnosed by a dentist or surgeon during a routine examination. Additional research methods are rarely used. Differential diagnosis of defects is carried out with glossitis, neoplasms, and inflammatory processes. The main diagnostic methods are:
- Visual inspection
. Intraoral examination is carried out using two mirrors. The size, shape, color, structure, anatomical and topographic location of the organ are assessed. Examine the mucous membrane of the tongue, the severity of the papillae, the presence of primary and secondary lesions. The degree of organ dysfunction is assessed.
- Teleradiogram
(TRG). A study in a lateral projection allows us to judge the size, area of the tongue, its relationship with the teeth and jaws. Studying the TRG parameters makes it possible to determine the presence of tongue anomalies and occlusion. For complex combined defects, a CT scan of the jaws and facial bones is performed.
Differentiation is required by congenital and acquired folded tongue: in the latter case, it may be a manifestation of Melkerson-Rosenthal syndrome. With this syndrome, other symptoms are also present - facial paralysis, swelling of the lips or face. In some clinical cases, the anomaly resembles sclerosing glossitis in the tertiary period of syphilis, which also needs to be differentiated.
Preparing for surgery
Preparation for surgery on the frenulum of the tongue includes consultations with a pediatrician or therapist and a standard list of examinations. A pediatrician or dentist refers you for surgical correction. No later than 2 weeks before surgery, it is necessary to undergo general and biochemical blood tests, a general urine test, and undergo testing for blood clotting, viral hepatitis, and HIV. In adult patients, a fluorography result will be required, possibly an ECG. It is important to rule out allergies to pain medications.
Before plastic surgery of the frenulum of the child’s tongue, it is better to feed him, because after the operation he is unlikely to be comfortable eating. Before manipulations begin, the oral cavity is hygienically cleaned and treated with antiseptic solutions.
The frenuloplasty lasts no more than half an hour. In the case of small children, parents will have to ensure that the child remains calm for at least 15 minutes. Hospitalization is not required for frenuloplasty.
Features of operations to shorten the hyoid frenulum
Depending on the technical features, there are several methods of surgery on the frenulum of the tongue:
- Transverse intersection of the mucous fold is the simplest method, which is indicated for small thickness and width of the mucous fold (frenotomy);
- Removal of a fragment of the frenulum - indicated in the case of a thick fold of large width (frenectomy);
- Frenuloplasty is needed if the frenulum fuses with the tissues of the floor of the oral cavity or the lower lip and it consists of moving fragments of soft tissue and mucous membrane.
The first two methods of frenulum correction are simple to perform and can be implemented either with a regular scalpel or with a laser. Plastic surgery is somewhat more complicated and requires a certain skill. Laser surgery is used in cases of frenulum defects in both adults and young patients due to important advantages:
- Speed of manipulation;
- No seams;
- No bleeding due to “sealing” of vessels with a powerful light beam;
- Short-term and comfortable rehabilitation;
- Does not require pain relief;
- No scarring.
Laser dissection of the frenulum is especially recommended for children, as it does not involve the use of surgical instruments, which by their mere appearance can cause fear. With laser plastic surgery of the lingual frenulum, the surgeon, after administering an anesthetic, directs a light beam at the frenulum, cutting it. During the procedure, the vessels are sealed, and the edges of the wound are disinfected. Healing occurs quickly and painlessly.
Complications
With insufficient hygienic care of the folded tongue, food debris and microorganisms accumulate in the grooves of the mucous membrane, and inflammation occurs - glossitis. With a decrease in immunity, fungal flora begins to multiply in the grooves, which is accompanied by the appearance of a white cheesy coating and unpleasant itchy sensations - candidiasis develops. With macroglossia, the mucous membrane of the tongue dries out, is easily injured, becomes crusty, and bleeds. Saliva drips from the corners of the mouth, causing maceration of the skin. The lingual tonsil can become inflamed when the body's reactivity decreases. Edema, swelling, hyperemia and pain when swallowing occur. The rudiments of the thyroid gland at the root of the tongue can increase significantly, causing dysphagia, difficulty breathing, and hoarseness.
Prognosis and prevention
The complete absence of tongue in combination with other multiple developmental defects has an unfavorable prognosis and can be fatal. Macroglossia, ankyloglossia, and cleft tongue can be surgically corrected. A folded tongue, lingual tonsils, and lingual goiter do not pose a threat to life, but should be observed by specialists (dentist, endocrinologist, otolaryngologist). There is no specific prevention of developmental anomalies. General preventive measures include giving up bad habits, treating chronic diseases, taking multivitamins for pregnant women, proper nutrition and lifestyle. Source: https://www.krasotaimedicina.ru/diseases/zabolevanija_stomatology/tongue-anomaly
Plastic frenulum of the tongue
Posted at 16:25h in Services by doctor
Plastic surgery of the frenulum of the tongue is a fairly simple surgical procedure that is most often performed on children: infants who have difficulty feeding, as well as preschool children who cannot pronounce individual sounds. If experts see the cause of problems in insufficient length or abnormal development of the frenulum of the tongue, they will certainly advise cutting, correction of its length or structure.
The frenulum of the tongue helps form the bite, correct pronunciation of sounds, ensures mouth opening, tongue mobility, swallowing and proper smiling, without which physical and psychological discomfort occurs. The frenulum is a thin arched mucous fold that runs from the middle and bottom of the tongue to the floor of the mouth, to the base of the gums. The normal length of the frenulum is about 27-30 mm.
The most common feature of the anatomy of the lingual frenulum is its insufficient length. This deficiency can be corrected radically by resorting to the help of a surgeon, or conservatively by regularly performing special exercises to stretch the frenulum. In severe cases, such training does not bring any results at all, and the choice inevitably falls on a radical measure in the form of plastic surgery.
Disputes between parents and even among specialists do not subside: many believe that it is better to postpone the operation or even abandon it in the absence of compelling reasons, while others, on the contrary, advocate cutting the frenulum almost immediately after birth, reinforcing this opinion that newborn babies probably won’t remember the operation and won’t experience the same stress as 4-5 year olds.
It is important that adults who are worried about the healthy future of their child do not exaggerate the scale of the problem. If outwardly the frenulum seems short, but it does not cause any difficulties when eating or forming speech, then there is no reason to have an operation “just in case”, “because in many families this is the case...”. A specialist should refer you for treatment after examining the oral cavity and confirming the fact of an abnormally short frenulum, which actually creates problems with pronunciation of sounds, nutrition, and provokes dental and periodontal diseases.