What are they?
Let's consider classifications depending on the anatomical location and histological structure.
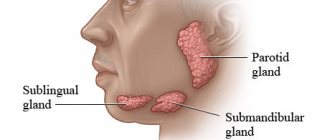
Depending on their location, these may be tumors:
- parotid salivary gland - the most common option, accounting for up to 85%;
- submandibular salivary gland;
- sublingual salivary gland;
- small salivary glands located on the oral mucosa.
There are quite a lot of histological variants, we will name only the most common:
- Benign: pleomorphic adenoma - up to 50% of all;
- basal cell adenoma;
- tubular adenoma;
- adenolymphoma;
- myoepithelioma.
- Malignant: mucoepidermoid carcinoma;
- adenoid cystic cancer;
- acinar cell carcinoma and others.
Benign tumors are characterized by slow growth and a favorable clinical prognosis. In many cases, they do not require any treatment at all, but only require regular monitoring. At the same time, malignant neoplasms grow quickly and aggressively, are capable of growing into surrounding tissues, blood vessels and nerves, as well as spreading to the lymph nodes and metastasizing to distant organs.
Pleomorphic adenoma (mixed tumor). This benign tumor is the most common, occurring in 72% of all epithelial tumors of the salivary glands. In terms of frequency of lesions, the parotid salivary gland is in first place, the mucosalivary glands of the palate are in second place, then, respectively, the submandibular, sublingual and minor salivary glands, glands of the lip, cheek, and tongue.Pleomorphic adenoma grows painlessly, slowly, over several years and can reach large sizes. When the adenoma is localized in the parotid salivary gland, paresis of the facial muscles is not observed. Upon examination, a tumor is detected in the area of the salivary gland, mobile, often with a bumpy surface. Its consistency is densely elastic, sometimes with areas of softening due to the mucus-like component. The skin above it does not change, it folds freely. The salivary function of the affected gland is usually not affected. Pleomorphic adenoma has a capsule, but may not be completely encapsulated, in which case the tumor cells penetrate into the adjacent glandular tissue. This explains tumor recurrences after extracapsular removal. Sometimes tumor growth accelerates significantly (within 1 month), and pain may appear. Such symptoms are characteristic of tumor malignancy; in such cases it is interpreted as carcinoma in pleomorphic adenoma.
The diagnosis of a tumor is clarified by cytological examination of the punctate, which is obtained in the needle in the form of a crumbly whitish mass.
Macroscopically, pleomorphic adenoma is a tumor in a thin translucent capsule, on a section in the form of a pasty mass of white-gray color with areas of mucus and compaction.
Microscopically, the tumor, in addition to pronounced epithelial tissue, contains mesenchyme-like areas consisting of myxoid or cartilage-like structures, the presence of which is explained by the accumulation of mucoid or hyaline substance between the myoepithelial cells.
Treatment is surgical. If the tumor is localized in the submandibular and sublingual salivary glands, the tumor is removed along with the gland. Tumors located on the palate, cheek, lips, tongue are excised within unaffected tissues. The peculiarity of the operation on the parotid salivary gland is associated with the branching of the facial nerve in the thickness of the gland. The nature and extent of surgical intervention depend on the size and location of the tumor. In all cases, it is necessary to excise the tumor with adjacent glandular tissue. Some authors suggest extracapsular tumor removal. When the tumor is localized in the lower pole of the gland, resection of this section is used. If the tumor occupies the anterior section and lies in the gland above the branches of the facial nerve, subtotal resection of the gland is performed in the plane of the branches of the facial nerve. Parotidectomy with preservation of the branches of the facial nerve is performed when most of the gland is affected and the tumor recurs, as well as when there is a tumor of the pharyngeal part of the gland. Access to the gland is carried out by two well-known methods - Kovtunovich and Redon. In the first case, the operation begins with exposure of the peripheral part of the facial nerve (middle branch), in the second - the central trunk.
The operation is parotidectomy with preservation of the branches of the facial nerve. A skin incision is made in front of the auricle 2-3 mm, starting from the scalp of the temple, bordering the earlobe and continuing in the retromaxillary and submandibular areas. the skin-fat flap is prepared and retracted anteriorly. The parotid-masseteric fascia and the anterior edge of the gland are exposed. When approaching the peripheral branches of the facial nerve, the location of the middle branch is determined: it is located next to the duct of the parotid gland along the line connecting the tragus with the angle of the mouth. The middle branch is dissected to the point of division of the trunk, then the upper and lower branches are isolated from the gland, holding them with threads to reduce trauma. The surface layer of the gland is removed, bandaged and the salivary duct is crossed. By lifting the branches of the nerve, the deep and pharyngeal parts of the gland are dissected and removed along with the tumor, and the external carotid artery is ligated along the way.
In an operation using the Redon method, after removing the skin-fat flap, the posterior edge of the gland is released and the external carotid artery is ligated. Then the trunk of the facial nerve is found deep in the wound between the mastoid process and the posterior edge of the mandibular ramus. The location of the nerve branch is determined and all three main branches are prepared. The further course of the operation is identical to that described.
An operation that involves removing only the superficial layer of the gland along with the tumor located above the branches of the facial nerve is called subtotal resection of the glands in the plane of the nerve branches.
In case of resection of the lower pole of the parotid salivary gland, a skin incision is made bordering the angle and body of the jaw, moving downwards by 1.5-2 cm, so as not to damage the marginal branch of the facial nerve. This must also be remembered during excision of the gland due to its location in this area. Subcutaneous tissue is dissected, m. platysma and fascia. The lower part of the gland, where the tumor is located, is exposed and removed. The wound is sutured in layers.
A mucous retention cyst most often forms in the minor mucosalivary gland of the lower lip, less commonly in the cheek, the anterior floor of the mouth, the lower surface of the apex of the tongue and palate. The predominant localization on the lower lip is associated with biting it.
The cyst is located under the mucous membrane, has the appearance of a hemispherical elevation with clear boundaries, ranging in size from 0.5 to 2 cm, with a bluish tint. Sometimes the mucous membrane over it is whitish in color, which is due to the presence of scar changes due to injury. Palpation of the cyst is of elastic consistency with ripple, painless. Biting the mucous membrane over the cyst can lead to its emptying, releasing a clear, viscous fluid. When the contents become infected, inflammation occurs.
Pathohistologically, the cyst wall is a connective tissue with granulations, turning into fibrous tissue, sometimes the inner side of the wall is partially lined with stratified squamous epithelium.
A mucous retention cyst must be differentiated from tumors of the minor salivary glands, which are less common, have an elastic consistency, sometimes with a bumpy surface, without fluctuation. In some cases, it is necessary to differentiate it from cavernous hemangioma, which is characterized by a purplish-bluish coloration and a symptom of filling.
Treatment consists of removing the cyst. Two converging semi-oval incisions are made in the mucous membrane above the cyst. Using a hemostatic mosquito clamp, the membrane is separated semi-bluntly from the surrounding tissues, the connective tissue bridges are cut with scissors and the cyst is isolated. Injured small glands protruding from under the edges of the wound and interfering with suturing are removed with tweezers or a “mosquito”, each separately and entirely. Using a scalpel for these purposes can lead to their dissection, incomplete removal and recurrence of the cyst. The operation is completed by applying catgut sutures to the mucous membrane.
Cyst of the sublingual salivary gland (ranula). This cyst is located, as a rule, in the anterolateral part of the floor of the mouth near the frenulum of the tongue. Clinically defined as an oval bulge, covered with unchanged mucous membrane or translucent with a bluish tint. The cyst is always intimately associated with one of the areas or the entire sublingual salivary gland. Its former name ranula (“frog tumor”) is determined by the type of cyst and its resemblance to the laryngeal bladder of a frog. It grows slowly, over months, and does not cause pain. When it reaches a significant size, speech is impaired and eating becomes difficult. Sometimes the cyst can extend beyond the midline of the floor of the mouth, displacing the tongue posteriorly or into the submandibular region. In the latter case, it is difficult to differentiate from a cyst of the submandibular salivary gland. On palpation, the cyst often appears as a formation with fluctuation, sometimes it is more elastic. When the membrane breaks through, a viscous transparent fluid is released abundantly from the cyst, and it is not contoured. After time, the cyst fills with fluid again and becomes visible.
Microscopically, the cystic fluid contains protein substances (clumps) and sometimes so-called cystic cells, apparently of epithelial origin.
Macroscopically, the cyst shell is thin, bluish-white. In terms of its microstructure, it is fibrous and granulation tissue associated with the interlobar connective tissue layers of the gland. The inner lining of the membrane rarely has cubic or columnar epithelium.
Diagnosis of a sublingual salivary gland cyst is usually not difficult. It should be differentiated from a cyst of the submandibular salivary gland, a dermoid cyst and vascular tumors (lymphangiomas and hemangiomas) localized at the bottom of the oral cavity.
Treatment: given the close connection of the cyst with the parenchyma of the gland, they are completely removed. The previously recommended cystotomy has limited use due to the frequent development of relapses. A cyst of the sublingual salivary gland, which spreads in the lower part of the floor of the oral cavity in the form of an hourglass, is operated on in two approaches: through an incision in the submandibular triangle, the lower part is bandaged and removed; from the side of the oral cavity, the sublingual gland with the remaining part of the cyst is excised.
A cyst of the submandibular salivary gland is much less common than a ranula. It is located in the submandibular triangle and is a painless formation of soft consistency. It grows slowly and is detected by chance when a swelling is detected in the submandibular region. A large cyst pierces the mylohyoid muscle (m. mylohyoideus) or bends around it from behind and spreads to the upper part of the floor of the mouth. In these cases, its bulging into the sublingual area is also determined. The salivary function of the gland is not affected.
Diagnosis of a cyst of the submandibular salivary gland is sometimes difficult. To clarify the diagnosis, a puncture is used: obtaining a yellowish mucous fluid suggests the presence of a cyst.
A cyst of the submandibular salivary gland is differentiated from lymphangioma, lipoma, lateral neck cyst, dermoid cyst.
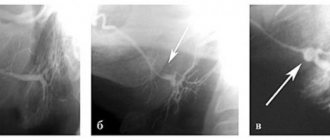
To determine the topography of the cyst, a double contrast method is used: cystography and sialography. Different X-ray projections allow you to determine the relationship between the cyst and the gland
Treatment. The cyst of the submandibular salivary gland is removed along with the gland.
Parotid salivary gland cyst. This is a rare disease, localized in the superficial and deep layers of the gland, mainly in the lower pole. The cyst grows slowly. It is often discovered by accident.
The cyst is a limited, painless swelling in the parotid region of soft elastic consistency. The skin over the cyst is of normal color and gathers loosely into a fold. Unchanged saliva is released from the gland duct. The contents of the cyst are yellowish liquid, sometimes cloudy, mixed with mucus. Histologically, the walls of parotid salivary gland cysts do not differ from the walls of cysts of other salivary glands.
A parotid salivary gland cyst is differentiated from organ-specific tumors, lipomas, vascular tumors of the gland, as well as from a branchial cyst caused by pathology of the first branchial cleft.
Treatment consists of removing the cyst. Due to the close connection of the cyst shell with the parenchyma of the parotid gland, the adjacent section of the latter is excised. The complexity of the operation is related to the location of the branches of the facial nerve. Surgical access to the gland is the same as when removing benign tumors of the parotid salivary gland.
"Surgical Dentistry" edited by Robustova T.G.
Fourth edition. Moscow "Medicine" 2010
Clinical cases:
Pleomorphic adenoma of the left parotid salivary gland.
How do they manifest themselves?
Symptoms of the disease completely depend on the location of the tumor and the involvement of surrounding tissues and organs in the pathological process, so they can be very diverse.
Initial manifestations:
- dense formation in the salivary gland or under the oral mucosa;
- long-term non-healing ulcer of the mucous membrane;
- moderate periodic pain is possible;
- discomfort when chewing or swallowing.
If the tumors are malignant, then at later stages the following may be observed:
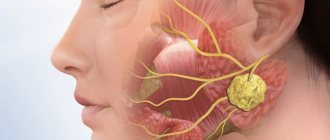
- facial asymmetry due to damage to the facial nerve due to parotid cancer;
- the appearance of dense, painless lymph nodes in the neck;
- redness and swelling of the skin over the tumor or lymph nodes;
- feeling of a foreign body in the throat;
- difficulty swallowing.
With metastasis to distant organs (lungs, liver, bones and others):
- weight loss for no reason;
- loss of appetite;
- nausea;
- constant weakness, fatigue;
- symptoms of damage to individual organs - shortness of breath, cough, hemoptysis, bone pain, jaundice, etc.
Causes of pain under the tongue
Modern medicine knows dozens of different reasons that can cause unpleasant and painful sensations under the tongue in an adult, teenager and child: from a banal mechanical injury to the frenulum, leading to tissue damage, to allergic reactions causing swelling. At the same time, there is a list of the most common causes observed in most patients.
The main causes of pain under the tongue:
- Mechanical injuries to the frenulum and muscle tissue are the most common cause of sublingual pain. As a rule, it is observed in people with a short frenulum. It is injured due to stretching, as well as in the event of mechanical trauma to tissues, for example, during eating, hygienic brushing of teeth, etc.;
- Dental pathologies of the oral cavity – stomatitis, dental problems (caries, periodontitis, periodontitis), gumboil, etc.;
- Infectious inflammation of the oral cavity - pain often manifests itself with sore throat. During this period, it is painful for a person to eat, swallow water and saliva, stick out his tongue or simply chew;
- Cellulitis or abscess of the floor of the mouth is a significant accumulation of pus in a small area of the floor of the mouth. Causes “bursting” of internal tissues, putting pressure on peripheral nerves - this provokes pain and tactile discomfort;
- An allergic reaction can be the body’s response to various irritants. Causes swelling of the soft tissues of the oral cavity, accompanied by discomfort or pain in the sublingual area;
- Asymmetry of the hyoid bone - an anatomical disorder in the growth of the hyoid bone, can provoke excessive or nonspecific pressure on the peripheral nerves, causing pain;
- Neuralgia is a general disease of the nervous system that manifests itself in its various parts. It is often a consequence of nervous shock and is accompanied by a feeling of painful numbness in the oral cavity;
- Diseases of internal organs and body systems - some areas of the tongue may reflect (irradiate) pathologies of internal organs, which is accompanied by painful sensations in the sublingual area;
Note! Most of the above problems that provoke the development of pain in the sublingual area can be caused by bacterial infections (streptococci), fungi (candidiasis), and herpes.
Why do they arise?
Most tumors arise from random mutations in our cells without any clearly identifiable cause. The only risk factors that increase the likelihood of developing the disease can be identified:
- Smoking and drinking alcohol lead to permanent damage to the mucous membranes and salivary glands, including contributing to the development of many other cancers: cancer of the lung, tongue, lip, larynx, esophagus, and so on.
- some viral infections (human immunodeficiency virus, human papillomavirus, Epstein-Barr virus);
- radiation exposure (including previous radiation therapy to the head and neck area for other neoplasms);
- the effect of chemicals used in the production of rubber, nickel, and hair dyes.
Diseases of the salivary glands
The salivary glands are a relatively small group of glands surrounded by the soft tissue of the cheeks, lips, and floor of the mouth.
Go to:
- Maxillofacial Surgery
The salivary glands produce secretions that keep your mouth moist, protect your teeth and mucous membranes, and help you digest food.
The major salivary glands include the paired parotid, submandibular (submandibular) and sublingual glands. The largest of them are the lunar glands.
Salivary gland problems
Many factors can interfere with the proper functioning of the salivary glands, preventing the production of sufficient secretions and preventing the flow of saliva into the oral cavity.
- Salivary stones (Sialolithiasis)
One of the most common causes of an enlarged gland is the presence of a stone in the gland or in its duct.
There are never too many promotions
Travel, training, food delivery and other partner offers Read more >>>
Sometimes salivary stones block the ducts, making it difficult for saliva to enter the mouth. Saliva accumulates in the gland, causing pain and swelling.
- Inflammation of the salivary gland (Sialadenitis)
A bacterial infection affects the gland, causing it to become inflamed, swollen, and its ducts blocked.
Sialadenitis is manifested by a painful enlargement of the gland and the appearance of purulent discharge from the ducts of the gland, opening into the oral cavity.
- Viral infections of the salivary glands
Viral infections such as mumps, influenza, Epstein-Barr virus, cytomegalovirus, coxsackievirus, and human immunodeficiency virus (HIV) can also lead to reactive swelling of the salivary glands. Swelling occurs in the parotid glands on both sides. Subsequently, after 48 hours, symptoms typical of a viral infection appear - headache and fever.
- Salivary gland cysts
A cyst can form in the salivary gland as a result of injury, infection, or the presence of a salivary stone. There are also congenital cysts of the parotid glands. The cyst is a slightly protruding round formation, soft in consistency, painless on palpation.
- Tumors of the salivary glands
There are malignant and benign tumors of the salivary glands.
The two main common tumors are pleomorphic adenoma and Warthin's tumor.
Pleomorphic adenoma usually occurs in the parotid glands. The tumor grows slowly and does not cause pain. Pleomorphic adenoma is a benign tumor.
Warthin's tumor is also benign and occurs in the parotid glands. It is usually observed on both sides more often in men.
-10% on all MRI and CT scans in the department on Narodnaya
- Sjögren's syndrome, Mikulicz's disease
Systemic autoimmune diseases, in which the process mainly involves the salivary and lacrimal glands, which leads to dry mouth (xerostomia) and a feeling of sand in the eyes (xerophthalmia). Women get sick more often.
Treatment of diseases of the salivary glands
Treatment of diseases of the salivary glands depends on the cause and nature of the disease. When stones form in the duct, treatment usually begins with removing the stones, prescribing a salivary diet and physiotherapeutic procedures. If these measures do not produce the expected results, surgery may be required to remove the stone or affected gland.
Surgery is usually indicated for malignant and benign neoplasms of the salivary glands.
Other salivary gland problems can be treated with medication.
Bacterial infections can be eliminated with a course of antibiotics. If necessary, bougienage of the gland duct is carried out and massage is prescribed. You can make an appointment with a maxillofacial surgeon by phone or through an online appointment.
How are they diagnosed?
The doctor will ask you about your problem and carefully examine the mass and surrounding lymph nodes. Be sure to tell your doctor when you noticed the lump, how it changed over time, and what risk factors you have.
Your doctor may order the following tests for you:
- Ultrasound of the soft tissues of the neck and CT/MRI of the neck and base of the skull with contrast - in order to assess the size of the tumor, the likelihood of its malignancy, the condition of the surrounding tissues and the presence of lymph node involvement;
- CT of the chest and PET/CT of the whole body if metastases are suspected to detect them;
- biopsy of the formation and suspicious lymph nodes with further histological examination, which is necessary in most cases when a malignant neoplasm is suspected.
How is the sublingual area treated?
Considering the above reasons, if you have the slightest pain in the sublingual space, you should immediately consult a doctor. The doctor will find out the source of the pain and determine a treatment regimen. In some cases, allergists and therapists provide treatment. But more often, pain in the floor of the mouth is treated by dentists.
In case of injury to the frenulum or the tissues of the area under the tongue, rinsing will be prescribed: with a solution of soda, romazulan, stomatophyte, hexoral, chlorophyllipt or iodinol. You should rinse your mouth according to the following schedule:
- morning and evening before bedtime;
- after meal.
The doctor also treats the area of injury with an antiseptic and anti-inflammatory drugs.
Inflammations caused by dental problems require immediate treatment - the specialists at Family Dentistry will get rid of caries, pulpitis or periodontitis and prescribe a course of anti-inflammatory drugs to cope with sublingual inflammation.
But one of the most dangerous diseases in the floor of the mouth is inflammation of the salivary glands. It is important to begin treatment before an abscess appears and complications develop. In this case, the doctor prescribes:
- antibacterial therapy - the doctor injects medicine into the gland and also prescribes a broader-spectrum antibiotic;
- drugs to activate saliva secretion - either a solution of potassium iodide or pilocarpine is used, sometimes regular lemon is used;
- hot dry compresses;
- physiotherapy course.
If the inflammation is advanced and pus appears or a stone has formed, the patient is sent to a surgeon, who cleans the gland cavity of pus and removes the stone.
How is the stage determined?
The stage is established according to the international TNM classification, in which each letter has a numerical value:
T (from the English tumor - tumor) - the size of the formation itself and the characteristics of its growth
N (from the English nodus - node) - the nature of the damage to the lymph nodes
M (from the English metastasis - metastasis) - the presence or absence of tumor spread to distant organs
Based on the combination of all three indicators, the stage of the disease is determined, which determines the prognosis and treatment:
How are they treated?
Treatment depends on the stage of the disease and may include surgery, radiation and drug therapy.
The main method is surgical treatment, which involves removing the tumor itself and the affected lymph nodes. At an early stage, this allows you to achieve the best results.
Radiation therapy and chemotherapy may be given before surgery (to shrink the tumor and subsequently remove it), after surgery (to get rid of tiny cells that the surgeon can't see and reduce the chance of recurrence), or instead for palliative purposes to provide relief when surgery is not possible due to a common process or severe concomitant pathology.
Symptomatic features of pain under the tongue
Pain in the sublingual area can have various symptomatic manifestations. First of all, they are accompanied by different types of pain (sharp, aching, throbbing), as well as constancy or frequency.
If you consult a doctor, it is very important to correctly characterize the pain - this will allow the specialist to narrow down the range of symptoms for differential diagnosis. For example, you may have pain in the frenulum under your tongue or pain under your tongue on the right/left.
One of the characteristic manifestations of stomatitis or candidiasis is a white pimple under the tongue. Its presence may indicate the development of a fungal or bacterial process. If such a symptom is detected, treatment will include antifungal and antibacterial therapy with the prescription of antibiotics or special antiseptic rinses. The presence of pimples of a different color may indicate the presence of a wide range of problems, the identification of which requires a thorough diagnosis of the oral cavity or the entire body.
What is the prognosis for the disease?
To determine prognosis, the 5-year survival rate statistic is used, which reflects the percentage of patients still alive 5 years after diagnosis.
As with other cancers, the prognosis depends primarily on the extent of the process. At stages I-II, when the process is localized in the salivary gland and does not go beyond its limits, this figure can reach 94%, at stage III and damage to the lymph nodes - 65%, and in the case of stage IV and distant metastases - 35%.
Ultrasound of the salivary glands: what are the capabilities of this diagnostic method?
Saliva, one of the most important components of the digestion process, is produced by special glands. What diseases are typical for the salivary glands? How can ultrasound help in their diagnosis? How is this procedure carried out?
These and other questions are answered by Yulia Vasilievna Safronova, ultrasound diagnostics doctor at Clinic Expert, Smolensk.
— Among the exocrine glands, a special place is occupied by the glands that produce saliva, one of the important biological fluids of the body. Yulia Vasilievna, tell us how many salivary glands are in the human body and where are they located?
— There are three pairs of large salivary glands in our body: parotid, submandibular and sublingual. The parotid muscles are located behind the lower jaw, at the level of the earlobe. The submandibular salivary glands lie among the muscles of the floor of the mouth, and the sublingual glands lie in the thickness of the muscle tissue under the tongue. In addition, in the tissues of the lips, cheeks, and palate there are many small salivary glands. All of them secrete saliva, which a person needs for the normal digestion process.
— What diseases can affect the salivary glands?
- For example, inflammatory ones are acute and chronic sialadenitis, abscesses, phlegmons. The salivary glands can be affected by tumors (benign and malignant) and autoimmune processes. Since these glands have excretory ducts, sialolithiasis (stones in the salivary glands) can develop. In addition, children sometimes have congenital anomalies in the development of glands, their ducts, or the complete absence of a gland (or glands).
— What diagnostic methods can be used to examine the salivary glands?
- Parotid and submandibular salivary glands are assessed using ultrasound, magnetic resonance imaging and computed tomography. The sublingual glands are not visible on ultrasound, so they are examined using CT, MRI, or contrast-enhanced X-ray. There are also methods for radioisotope diagnostics of the salivary glands, but they are not widely used due to their toxicity.
Focal lesions of the small salivary glands are more often detected during a dental examination.
— Let's talk in more detail about ultrasound examination. What does an ultrasound of the salivary glands show?
— During an ultrasound examination, we evaluate the structure of the salivary glands and their size. We also see the blood supply to the gland, the condition of its ducts. Ultrasound helps detect inflammation, stones, and neoplasms in the salivary glands.
— To whom and in what cases is this study prescribed?
— Ultrasound diagnostics is, as a rule, the first stage of the study of the salivary glands. Dentists, therapists or ENT doctors refer patients for an ultrasound of the salivary glands if patients complain of pain in the submandibular or parotid region, difficulty swallowing, increased or decreased salivation, or the presence of compactions in the areas of projection of the salivary glands. Sometimes patients come forward on their own.
I would like to emphasize that ultrasound is a kind of screening method for studying the salivary glands. For a more accurate diagnosis, it is sometimes necessary to refer patients for computed tomography or magnetic resonance imaging.
— Yulia Vasilievna, please tell us how an ultrasound of the salivary glands is done
— In the classic version, the patient lies with his back on the couch, and a cushion is placed under the neck. The patient raises his chin high. The doctor applies a special gel to the area under study and, using a linear sensor, examines the submandibular, parotid area, where the salivary glands and adjacent lymph nodes are located. The procedure is carried out on both sides. During the study, the size of the glands, the state of their structure, and the patency of the ducts are recorded. All this data is recorded in the conclusion that the patient receives at the end of the study. The entire procedure takes on average up to 15 minutes.
— Are there age restrictions for this research method?
— No, because ultrasound is a safe method. Therefore, ultrasound of the salivary glands can be performed on both infants and elderly people.
— Are there any contraindications to performing an ultrasound of the salivary glands?
— There are no absolute contraindications. We do not perform the procedure if there are pustular skin lesions or open wounds in the study area.
Interviewed by Sevilya Ibraimova
You can sign up for an ultrasound of the salivary glands here. ATTENTION: the service is not available in all cities
The editors recommend:
MRI of the salivary glands: when is it necessary?
For reference:
Safronova Yulia Vasilievna
In 2006 she graduated from the Smolensk State Medical Academy 2006-2007. – clinical internship in therapy In 2009, she received a certificate in ultrasound diagnostics and minimally invasive technologies under ultrasound guidance. In 2013, she defended her PhD thesis in therapy. Currently, she is an ultrasound diagnostic doctor at Clinic Expert, Smolensk