Salivary gland cancer is a rare oncological disease characterized by the development of malignant tumors in the large salivary glands (submandibular, parotid, sublingual) or small (lingual, labial, palatal, buccal, molar). This disease is characterized by slow dynamics and hematogenous metastasis.
Confirmation of the diagnosis at the Yusupov Hospital occurs after a thorough examination by an oncologist using additional types of diagnostics - CT, PET-CT, MRI, and tissue biopsy. Treatment is prescribed on an individual basis based on the patient’s examination results.
Tumor of the parotid salivary gland - causes of development
The causes of salivary gland cancer have not yet been precisely established. The main factors of occurrence are considered to be adverse environmental effects, excessive insolation, infectious and inflammatory diseases of the salivary gland, certain eating habits, and smoking. The factor that has the most negative effect is radiation in any of its manifestations - radiation therapy, repeated x-ray examinations, living in an area of high radiation, etc. There is also a connection with the professional type of activity of a person, since a tumor of the salivary gland most often appears in asbestos workers mines, metallurgical enterprises, automobile and woodworking plants. This is due to the constant contact of people in these professions with dangerous carcinogens - lead, chromium compounds, silicon, asbestos, etc. A high likelihood of developing cancer also exists in patients who have had mumps in the past. The factor of smoking today is controversial, since some scientists believe that it affects the development of certain types of cancer of the salivary glands, while others deny the connection of this bad habit with tumors of the salivary glands. Eating behavior can negatively affect the development of cancer processes in the human body if there is insufficient consumption of plant fiber, yellow and red fruits and vegetables, herbs and excessive consumption of cholesterol.
Materials and methods
In the period from 2004 to 2013, out of 289 patients admitted to the laboratory of intensive therapy methods of the Federal State Budgetary Institution “Research Institute of Rheumatology named after. V.A. Nasonova" for examination with a significant increase in the SG, PNJ, palatal and small SG of the lower lip with various presumptive diagnoses, 32 (11%) were diagnosed with IgG4-C (Table 1). In 8 patients before 2009, IgG4 was not detected in the blood serum, but they are also considered in this work on the basis of classic clinical and laboratory manifestations of BM and the obligatory presence of >40% of PCs secreting IgG4 during immunomorphological examination of blocks of removed tissue of lymph nodes (LNs). ), orbits, PNJS and OSJ. Only 3 (9%) patients had isolated sclerosis of the PNJ (IgG4-3), while 29 (91%) had damage to several organs within the framework of IgG4-3. Another 29 patients with IgG4-3, without involvement of the gastric tract (orbital area in 14, retroperitoneal organs in 11, nasopharynx in 1, lymph nodes in 3) were excluded from the analysis. A mandatory condition for the inclusion of patients in this study was morphological, immunomorphological, X-ray and radiological and laboratory confirmation of the nosological diagnosis according to the international diagnostic criteria of IgG4-3 [14]. All patients underwent a complete dental and ophthalmological examination. Laboratory examination included a clinical analysis of blood and urine, a biochemical blood test with electrophoresis of serum proteins, immunological research methods with determination of rheumatoid factor (RF) levels, determination of CRP by a highly sensitive method, the study of IgG, IgA, IgM and IgG4 was performed using the nephelometric method on the BNProSPEC apparatus. An increase in IgG4 level >2.0 g/L was considered diagnostic when determined. The study of the levels of complement fractions C3/C4, antinuclear antibodies, Ro/La antibodies, antineutrophil cytoplasmic antibodies (ANCA) was performed using the ELISA method (Orgentec, Germany). Patients with suspected development of lymphomas underwent an immunochemical study of serum and urine proteins; using fresh biopsy material, determination of B-cell clonality by rearrangement of Ig heavy chain genes and T-cell clonality by rearrangement of TCR
T-cell receptor in the laboratories of humoral immunity and molecular biochemistry of the Federal State Budgetary Institution State Scientific Center M.Z. Morphological examination of biopsy specimens was carried out by 2 independent morphologists in the morphology laboratories of the Federal State Budgetary Institution "NIIR named after. V.A. Nasonova”, Federal State Budgetary Institution “Russian Scientific Research Center named after. N.N. Blokhin" or FGBNU SSC M.Z. Immunomorphological studies were carried out only in the last 2 institutions. To diagnose IgG4-SZ, a panel of antisera to CD20, CD138, κ, λ, IgG, IgG4 (clone HP 6025, Zymed) was used. Morphological/immunomorphological and molecular study of biopsy specimens previously removed in other institutions of the lacrimal glands - 5 (15.6%), PNJG - 8 (25%), OSG - 2 (6.3%) was carried out in blocks. Study on fresh material of the orbits - 18 (56.3%), PNJS - 11 (34.4%), OSJ - 5 (15.6%), small SG - 25 (77.5%), LU - 2 (6 .3%), surgical material of the nasopharynx - 3 (9.5%) and the process of the cervical vertebra - 1 (3.1%) were performed to confirm the morphological/immunomorphological diagnosis of IgG4-CD, and to exclude other diseases. Specially developed minimally invasive techniques were used to take biopsies of the orbits, PNJ and OAJ to verify the diagnosis, allowing to avoid traumatic surgical interventions, such as removal of POJS, orbitotomy and partial resection of OAJ.
Table 1. Various diseases with damage to the spinal cord/pulmonary tract, diagnosed at the Federal State Budgetary Institution "Research Institute named after. V.A. Nasonova" for the period from 2004 to 2014 (n=289)
Neoplasm of the parotid salivary gland - symptoms
A tumor of the parotid gland in the initial stages can be practically asymptomatic. The first witnesses of the disease may be causeless dry mouth or, on the contrary, excessive salivation. Further dynamics of the disease are often characterized by the following clinical manifestations:
- numbness of the face or part of it in the area of the salivary glands;
- swelling, painful lump in the neck, mouth or jaw;
- pain while swallowing;
- increased body temperature;
- dizziness;
- discomfort when opening the mouth;
- muscle pain or weakness (paresis) in a certain area of the face.
However, these symptoms may also indicate the occurrence of other benign neoplasms, for example, a salivary gland cyst. If you experience one or more of the above symptoms, you should consult a qualified physician for a diagnosis. Oncologists at the Yusupov Hospital, thanks to their professionalism and extensive experience working with patients of different ages, will competently prescribe treatment and all the necessary diagnostic measures.
results
In 32 patients (14 men, 18 women) with the onset of the disease from 13 to 77 years (median 42.4 years), IgG4-3 GS was diagnosed, while in 29 (90.6%) patients it was systemic and involved other organs. The duration of the disease at the time of diagnosis averaged 4.4 years, ranging from 2 months to 20 years. The main diagnoses that appeared in the medical documentation of patients before admission to the hospital of the Federal State Budgetary Institution “Research Institute of Rheumatology named after. V.A. Nasonova” are presented in table. 2. Only 3 (9.3%) of 32 patients with systemic disease associated with IgG-4 were correctly suspected of having BM; In 24 patients, during the development of the disease, various oncohematological diseases were diagnosed, and therefore orbitotomies (4), removal of the PNJ (8), partial resection of the AFJ (2), removal of lymph nodes (4) and laparotomy (2) were performed. Rheumatological diagnoses were assumed in 10 patients, and the diagnoses of salivary stone disease, chronic sialadenitis and endocrine ophthalmopathy appeared extremely rarely. In table Figure 3 presents the main manifestations of the debut of IgG4-S3. The acute onset of the disease with symptoms of fever, arthralgia, significant loss of body weight, girdle pain, lymphadenopathy, jaundice, hepatosplenomegaly was extremely rare and was observed in 3 patients (autoimmune pancreatitis + sclerosing cholangitis + PNSF + PTH - 3 + generalized lymphadenopathy - 1) and only in 1 case in a patient with isolated lesions of the PNJ. It should be noted that in all cases of acute onset of the disease, the presence of oncohematological pathology was assumed (pancreatic cancer - 2, lymphoma - 2). In 28 patients, the disease developed gradually from lesions of the nasal cavity and ONP, and a massive increase in the PNJ and the orbital area at the onset of the disease was observed much more often than an increase in the OA. It should be noted that the phenomena of chronic rhinitis, sinusitis and bronchitis in some cases preceded the development of lesions of the orbits and S.Z. for many years. Various types of allergic diseases (bronchial asthma, chronic rhinitis, polypous sinusitis, atopic dermatitis) and drug allergies were observed in 9 (28.1%) patients.
Table 2. Diagnoses in 32 patients with systemic diseases associated with IgG before admission to the Federal State Budgetary Institution “NIIR named after. V.A. Nasonova" RAMS
Table 3. Clinical manifestations of IgG4-SZ at the onset of the disease
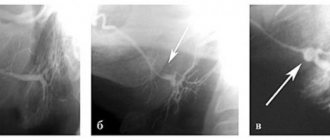
The main clinical manifestations of the disease at the time of examination and during dynamic observation, the results of a morphological and immunomorphological study of a biopsy specimen of the PNJ in one of the patients with IgG4-CD are presented in Fig. 1.
Rice. 1 (a-f). Results of examination of patient S. a, b - increase in PNJS in SS (Küttner's tumor; 2008); c—e — biopsy specimen of the PNJ in SS (Kütner’s tumor), stained with hematoxylin and eosin, UV. 100.
Patient C
.: 2003 (44 years old) - polypous rhinosinusitis due to aspirin-induced asthma; 2006 (47 years old) - polypous rhinosinusitis + damage to the orbits (septoplasty); 2007 (48 years old) - orbitotomy on the right, then on the left; 2008 (49 years old) - increase in PNJ (see Fig. 1, a, b), biopsy, diagnosis of IgG4-SZ; 2013 (53 years old) - massive increase in the pulmonary arterial systolic area, PNJS, intrathoracic lymph nodes, lung damage, interstitial nephritis. Serum IgG4 levels >50 g/L. When reviewing preparations of the removed mucous membrane of the nasopharynx, lacrimal glands and a biopsy of the mucous membrane of the nasopharynx, biopsies revealed from 50 to 90% of PCs secreting IgG4. Clinical diagnosis: IgG4-C3 with damage to the nasopharynx (polypous pansinusitis), lacrimal glands (sclerosing dacryoadenitis), gastric gland (SS PNChSZH and OSZH), mediastinal lymph nodes (lymphadenitis), lungs (interstitial pneumonitis) and kidneys (tubulointerstitial nephritis).
Almost all patients developed damage to the PNJ, and 2/3 of the patients had damage to the MUJ and orbital area (Table 4). Only 3 patients had isolated SS of PNCJ, while in 29 (90.6%) cases there was involvement of other organs and the disease was considered systemic. 17 (52.2%) patients fully met the criteria for the diagnosis of BM (enlargement of all groups of glands and lacrimal glands). An increase in intrathoracic lymph nodes was observed in 1/3, peripheral lymphadenopathy was observed less often, and an increase in intra-abdominal lymph nodes was extremely rarely detected. Interstitial lung damage was present in 22% of patients with the development of foci in the lung parenchyma in 12.5%. Autoimmune pancreatitis, sclerosing cholangitis with PTH was diagnosed in 3 (9.4%) patients and in 2 (6.3%) the development of membranous nephritis (1) and interstitial nephritis (1), confirmed by kidney biopsy, was observed. The onset of the disease with lesions of the cervical vertebra with subsequent development of SS was observed in 1 patient. She had monoclonal secretion in the immunochemical study of blood serum and urine, morphology and immunomorphology of B-cell lymphoma with massive PC synthesis (IgG4 >60%) in the biopsy specimen of the PNJ, and B-cell clonality by rearrangement of the Ig+ heavy chain in fresh PNJ tissue. The infiltrate in the removed spinous process of the second cervical vertebra was similar to the lymphoplasmacytic infiltrate and pronounced fibrosis in the tissue of the PNJ, but due to the lack of a block of surgical material, an immunohistochemical study (IHC) was not performed. Only in 8 (25%) patients, dental and ophthalmological examination revealed moderate xerostomia and the formation of dry eye syndrome without signs of epitheliopathy. The latter sign was present in patients with previous orbitotomy. Without treatment, patients with IgG4-3 experienced gradual involvement of other organs and tissues in the process (see Fig. 1). Clinical manifestations of IgG4-SZ at the onset and during dynamic observation are presented in Table. 3, 4. The main laboratory abnormalities identified in patients with this disease are presented in table. 5. Increased ESR was observed in 50% of patients and 1/3 of patients had moderate eosinophilia in the blood. Only in one case was eosinophilia up to 30%. High hyperproteinemia up to 110.0 g/l with hypergammaglobulinemia up to 50% was observed in 5 patients and was associated with a high level of IgG due to the IgG4 fraction. In some cases, the entire IgG fraction consisted of IgG4. These patients typically had high levels of IgE [8]. An increase in proteins of the acute phase of inflammation was determined in 7 patients and an increase in ESR was more often associated with disproteinemic disorders - hyperproteinemia with hypergammaglobulinemia due to high levels of IgG/IgE. Signs of autoimmune disorders: a slight increase in titers of antinuclear factor (ANF) and RF were found in 40 and 25% of patients, respectively, and were detected mainly in cases of damage to all groups of SG/lacrimal glands. Monoclonal secretion was detected in 2 patients and in one case was associated with the development of lymphoma from mucosal lymphoid tissue (MALT lymphoma) of PNSJ from IgG4-related S.S. Conducted morphological studies on blocks of previously removed SG/lacrimal glands and biopsied tissues of the orbits, OSG and PNJ demonstrated an IgG/IgG4 ratio of 40 to 95% in all cases, while pronounced manifestations of fibrosis were observed in biopsies of the orbits and PNJ (see Fig. 1 , VC). In cases of BM, fibrosis phenomena were minimal and the formation of follicle-like structures with MALT tissue was observed (Fig. 2, 3). As part of the study, patients with a significant increase in PVS and PNPS were diagnosed with various diseases (see Table 1), and they are not analyzed in this study.
Table 4. Main organ lesions in IgG4-C3 during follow-up
Table 5. Laboratory abnormalities for IgG4-C3 Note. * — number of examined patients.
Rice. 2. BM (IgG-C3). Biopsy of the thyroid gland: lymphoplasmacytic infiltration, formation of follicle-like structures (arrows).
Rice. 3. BM. IGHI: PC (a); PCs secreting IgG (b); PCs secreting IgG4 (c).
Parotid salivary gland cancer (ICD 10) - classification of tumors
All salivary gland tumors are divided into three main groups:
- malignant - sarcoma, adenocarcinoma of the salivary gland, carcinoma of the salivary gland, adenoid cystic carcinoma of the parotid gland, as well as metastatic and malignant tumors;
- benign – non-epithelial tumors (hemangiomas, chondromas, fibromas, lipomas, salivary gland lymphoma, neuromas) and epithelial (adenomas, adenolymphomas, mixed tumors);
- locally destructive - mucoepidermoid tumor of the parotid salivary gland, cylindroma, acinar cell neoplasms.
Doctors classify the stages of salivary gland cancer according to the TNM system:
- T0 – absence of neoplasm in the salivary gland;
- T1 – the tumor is present, its diameter is less than 2 cm and is not localized only within the gland;
- T2 – tumor diameter up to 4 cm, localization – within the salivary gland;
- T3 – neoplasm with a diameter within 6 cm, does not spread or spreads without affecting the facial nerve;
- T4 – the tumor reaches a diameter of more than 6-7 cm and spreads to the facial nerve and base of the skull;
- N0 – tumor without metastases to local lymph nodes;
- N1 – metastasis occurs in one adjacent lymph node;
- N2 – metastases are present in several lymph nodes, diameter – up to 6 cm;
- N3 – metastases affect several lymph nodes with a diameter of more than 6-7 cm;
- M0 – no distant metastases;
- M1 – distant metastases are present.
The stages of cancer are determined through a series of diagnostic measures that allow a comprehensive study of the tumor process and selection of the most appropriate treatment.
What kind of disease is this?
Adenocarcinoma of the salivary glands is a type of glandular cancer with the growth of a tumor-like body from the epithelial cells of the ducts of the salivary canals. The parotid and submandibular glands are affected. A distinctive feature is hematogenous metastasis with a rapid course, an increase in tumor size, and the formation of regional metastases.
Adenocarcinoma is a diffuse or nodular induration. It often contains a cavity, and doctors often misdiagnose it as a cyst. Scientists often associate the causes of occurrence with genetics, since the ducts of the salivary glands are similar to the ducts of the mammary gland. The structure of the tumor is glandular, with many cellular layers in the form of a lining. The inner layer consists of cellular elements with a clear edge, nuclei and cytoplasm. The outer layers are more disordered and do not have clear boundaries. It happens that some of the flow structures are filled with proliferating cells. Sometimes they merge, forming impressive conglomerates, entire complexes with signs of flow-type secretion. Mucus accumulates between the cells, causing the formation of follicle-like lattice-like structures. Tumor-like cells may resemble salivary duct epithelium with eosinophilic cytoplasm.
Adenoid cystic cancer of the salivary gland - diagnosis and treatment
The most accurate diagnosis can be determined after a detailed examination by an oncologist at the Yusupov Hospital, as well as based on the results of certain examinations. Diagnostic measures prescribed for suspected salivary gland cancer are:
- magnetic resonance imaging (MRI). The principle of this procedure is the use of a magnetic field and radio waves to visualize images of soft tissue, bones and internal organs. MRI is an absolutely painless and safe examination method and is widely used to check or confirm the diagnosis of salivary gland cancer;
- Ultrasound. An ultrasound examination is the first examination that an oncologist prescribes if salivary gland cancer is suspected. Ultrasound helps determine the size, diameter and exact location of the tumor. During the examination, a tumor biopsy is often performed;
- open biopsy. Such a diagnostic measure is rarely carried out, since there is a risk of damage to the facial nerve, and also due to the likelihood of damage to healthy areas of the skin through the spread of a malignant process;
- CT scan. This examination method allows you to visualize a three-dimensional image of internal organs or other parts of the body. CT is widely used to study a large number of diseases, including cancer, both for preliminary examination and to monitor the dynamics of the disease.
The technical equipment of the Yusupov Hospital allows any diagnostic procedure to be carried out with maximum accuracy. Patients of the Yusupov Hospital can be guaranteed to receive high-quality and competent interpretation of examination results, as well as further prescription of treatment - surgical or conservative.
How can I purchase Israeli-made medicines?
- 1st method: undergo examination in Israel. After making a diagnosis, the doctor at the Ikhilov Oncology Center will create an individual treatment program for you and prescribe the necessary medications. You can buy them at an Israeli pharmacy.
- 2nd method: receive medications after a remote consultation. The Ichilov Cancer Center organizes diagnosis and treatment of patients from abroad as part of a telemedicine program. After this, the patient receives a prescription for Israeli drugs, which he can order in Israel, including home delivery.
Find out if the treatment is prescribed correctly
Tumor of the parotid salivary gland: treatment without surgery at the Yusupov Hospital
The prognosis for a salivary gland tumor entirely depends on the individual clinical picture of the patient. As a rule, it is more favorable for women.
Benign neoplasms are subject to surgical removal. Surgery for tumors of the parotid glands is associated with the risk of trauma to the facial nerve, therefore, both the surgical process and the rehabilitation period require careful monitoring by an oncologist. Possible postoperative complications are paralysis or paresis of facial muscles, as well as the occurrence of postoperative fistulas.
Salivary gland cancer most often involves combined treatment - surgery together with radiation therapy. Chemotherapy for tumors of the salivary glands is used extremely rarely due to the fact that in this case it is ineffective.
The treatment of salivary gland cancer at the Yusupov Hospital is carried out by experienced oncologists, whose professionalism has been repeatedly confirmed by international certificates and diplomas. Our doctors annually undergo advanced training courses, which allows them to use only the most modern and effective techniques in medical practice. The drugs used in the hospital or prescribed during treatment are safe and most effective.
To make an appointment with an oncologist at the Yusupov Hospital, you should call or write to the coordinating doctor on our website.
How to make an appointment with a specialist in oncology
The oncology department employs highly qualified specialists. You can make an appointment with an oncologist using a special form on the website. It is also possible to get an appointment with a specialist by calling: +.
You can make an appointment for a consultation or carry out a full diagnosis if you suspect cancer. Modern equipment and the professionalism of our doctors allow us to accurately diagnose and begin the most effective, rapid treatment that will give the best results.
The clinic is located in the very center of Moscow at the address: 2nd Tverskoy-Yamskaya lane 10 (Mayakovskaya metro station).
Complications and consequences
Salivary gland adenocarcinoma
subject to surgery followed by chemotherapy. Complications are observed in almost all patients without exception:
- distortion of facial expressions due to impaired innervation of facial muscles;
- hearing loss up to complete deafness;
- psychosis, stress that impairs performance and quality of life.
The operation often causes bleeding, fistula formation, and paresis when the facial nerve is injured. Radiation therapy provokes the appearance of blisters on the skin, dryness and hyperemia in the mouth.
Prevention measures
Preventing the development of adenocarcinoma of the salivary glands means:
- protect the body from unnecessary radiation exposure;
- monitor the condition of the mouth and neck, and periodically inspect for the appearance of lumps and lumps;
- undergo professional examinations once a year by a dentist or laryngologist;
- transfer to another job from hazardous production;
- stop drinking alcohol.
Adenocarcinoma is a typical representative of the oncological process and is formed from epithelial cells with a glandular component. Cells actively secrete toxins, are prone to metastasis, rapid and continuous reproduction, losing the function of apoptosis. The neoplasm can be localized in any organ where there are glandular structures.
Types and characteristics of tumors of the submandibular glands
Types of adenocarcinoma localized under the jaw:
- 1. Clear cell
tumor with a glandular structure. Externally similar to a cylinder with localization on the cheeks, lip, palate, and mouth. The main focus of the lesion is the parotid region. Difficult to recognize at an early stage. Develops slowly (up to 15 years). It is most often formed in the form of a single node with the union of cells into a ball. Tissues around the circumference are susceptible to fibrous degeneration. - 2. Mucinous
- a rare cystic form with poorly defined boundaries and average density. The substance inside the affected gland may be glandular. The peculiarity of the form is the formation of a mucin bond, so neoplastic cells are in a floating state. The tumor may have a different shape in the center of the hyperchromic nucleus. Localized under the tongue and jaw. - 3. Carcinoma of the salivary duct
localized anywhere in the salivary glands: larynx, near the ear, under the jaw, in the mouth. The neoplasm is a collection of proliferating cells that often affects the facial nerve. It occurs in men and is characterized by a rapid increase in size at the initial stage. Then it can decrease on its own. - 4. Oncocytic
in the form of amorphous cells, a soft tissue tumor with formation under the jaw, near the auricle. Difficult to diagnose because it does not cause discomfort or pain. It occurs in people of a wide age group (30-90 years), affects the maxillofacial nerve roots, causing facial paralysis, neuropathy, and paresis.
Forecast
The disease is difficult to treat and often recurs. Forecasts in most cases are disappointing. If there are no metastases at an early stage, muscles and nerves are not affected, then the outcome is quite favorable. Surgical removal of the gland along with the tumor body will eliminate the risk of relapse and prolong the life of patients. At stages 3-4, survival, unfortunately, does not exceed 5 years. Adenocarcinoma metastasizes, affecting the lungs, liver, bone tissue, and lymph nodes. It often recurs even after radiation or chemotherapy.
Various factors influence forecasts. The most favorable is highly differentiated adenocarcinoma, treated with radical methods at an early stage. Patients may decline in as little as 2-3 months as undifferentiated adenocarcinoma progresses. A lot depends on how the operation was performed. Incorrect selection of antitumor therapy provokes relapses and the appearance of new metastases in the future. The terminal stage of the oncological process does not guarantee survival for 5 years, since the quality of life in patients is unsatisfactory.