- Causes of salivary gland cancer and risk groups
- Symptoms of the disease
- Diagnostic methods
- Classification: types of salivary gland cancer
- Stages of the disease
- Treatment
- Complications and relapses
- Life prognosis at different stages of cancer and prevention
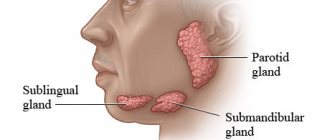
The salivary glands produce saliva, a liquid found in the oral cavity that performs some important functions: wetting the mucous membrane, food, facilitating articulation, swallowing, protecting against pathogenic bacteria, etc. There are two groups of salivary glands:
- Large: sublingual, parotid, submandibular.
- Small ones have a microscopic structure, scattered throughout the oral cavity - there are several hundred of them in total.
Cancer can develop in all of these glands. Most often (in 7 out of 10 cases), benign and malignant tumors arise in the parotid salivary glands. Approximately 1–2 tumors out of ten occur in the submandibular salivary glands; in 50% of cases they are malignant. In rare cases, cancer develops in the sublingual or minor salivary glands.
Causes of salivary gland cancer and risk groups
A normal salivary gland cell becomes cancerous when a certain set of mutations occurs in it. The development of malignant tumors is caused by mutations in oncogenes (genes that activate cell reproduction) or tumor suppressor genes (suppress cell reproduction, “repair” damaged DNA, trigger programmed cell death - apoptosis). In each specific case, it is very difficult to judge the reasons for the mutations that occurred in cells. It is impossible to say why exactly they happened.
There are some risk factors that increase the likelihood of developing a malignant tumor:
- The older a person is, the more changes in his genes accumulate, the higher the likelihood of developing various types of cancer.
- Salivary gland cancer is more common in men than in women.
- Irradiation of the head. For example, this may be a previous course of radiation therapy, exposure to ionizing radiation in the workplace.
- There is evidence that the risk of salivary gland cancer is increased in people who have certain occupational hazards: contact with asbestos, nickel alloy dust, work in enterprises that produce rubber and woodworking.
The role of heredity is currently considered insignificant. Most patients do not have a family history (close relatives who have been diagnosed with the same type of cancer). The role of alcohol and tobacco has not been proven. These unhealthy habits are known to increase the risk of head and neck cancer in general, but no association has been found with salivary gland cancers.
Is a mobile phone dangerous? In one study, researchers found that heavy cell phone users were more likely to have parotid tumors (usually benign).
But other studies have not found such a relationship.
PATHOLOGICAL RESULTS
Box 4 contains a short list of variants of salivary gland pathology.
| Box 4 Variants of pathology of the salivary glands
|
Acute sialadenitis
Since we have to deal with paired organs, it is important to compare both glands in one picture. Characteristic findings are explained by inflammatory edema and an increase in fluid content in the parenchyma, which is transformed during inflammation. Typically we see the following:
- Diffuse expansion of the entire affected gland.
- The organ can be clearly demarcated from adjacent structures.
- The structure of the parenchyma appears loose, heterogeneous, coarsely textured and more hypoechoic.
- Limited hypoechoic formations can be detected as a concomitant inflammatory reaction of the intraglandular lymph nodes.
- Zones of liquefaction (as signs of abscess formation) are visualized as hypoechoic with a hyperechoic surrounding wall and pronounced distal signal enhancement.
- Coarsely structured hyperechoic echoes at the center of such liquefaction lesions may correspond to areas of necrotic tissue.
Chronic sialadenitis
Sonographic imaging is highly dependent on the duration and degree of inflammation of the glandular parenchyma. As in the case of acute sialadenitis, a conclusive differential diagnosis between the various pathogenic forms of chronic sialadenitis cannot be made using sonography alone. Typically we see the following:
- A clear increase in the unevenness of the echo texture.
- The internal structure has a heterogeneous pattern, most likely due to fibrotic changes in the parenchyma.
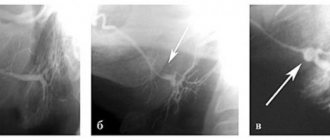
- Small cystic echo lesions are formed, which correspond to limited ductal ectasia (Fig. 4).
- Sometimes stones within the gland are identified as echogenic structures with a distal acoustic shadow.
Rice. 4. (A) Chronic sialadenitis of the parotid gland. (B) Sialocele of the parotid gland. (C) Dilatation of Stenson's duct (arrows).
Differential diagnosis is important in the following situations:
- Patients suffering from Gougerot-Sjögren syndrome have sonographic signs of enlarged, heterogeneously structured, hypoechoic salivary glands. Numerous limited hypoechoic formations are found inside the parenchyma, which may be associated with cystic dilatation of the ducts, on the one hand, or with enlargement of intraglandular lymph nodes, on the other hand. Sonographically, the structure of the salivary glands looks like a “cloud”.
- Sialadenitis of epithelioid cells (Heerford syndrome) is sonographically characterized by a rich echo pattern interrupted by numerous enlarged lymph nodes that appear as hypoechoic masses.
- Kütner's tumor of the submandibular gland is visualized as a formation with an indistinct echo signal in a certain part of the submandibular gland, which is easily mistaken for an adenoma.
- Ultrasound helps detect changes after radiation therapy. The echohomogeneous pattern disappears after irradiation, with a more hypoechoic and sometimes irregular pattern being a sign of loss of function.
- Other secondary pathological changes (edema, infections and soft tissue tumors) around the salivary glands are easily distinguished from primary salivary gland pathology.
Parotid abscess
The evolution of the inflammatory process is characterized by a hypo-, anechoic lesion with irregular edges. Typically we see the following:
- Hypo-, anechoic lesion with irregular edges.
- Peripheral hypervascularization, which is determined by color Doppler scanning.
- In the case of partial necrotic changes, lymph nodes with anechoic areas of necrosis are identified.
- In the case of fistula formation, a fistula is defined that reaches the skin surrounded by edematous tissue.
An important initial sign of an abscess is the appearance of vessels with a linear and fairly regular direction, which subsequently changes to a more irregular one, and is characterized by numerous anastomoses, which can be determined by an increase in the intensity of the color Doppler signal. In abscesses, the color Doppler signal has a peripheral structure because in this case the vessels are intertwined along the periphery of the abscess.
Enlarged lymph nodes
Lymph nodes may be found inside the parotid gland. However, only around the submandibular gland, due to the characteristics of embryological development. In the parotid gland, a group of small lymph nodes (3-5 mm) is located along the retromandibular vein. These lymph nodes carry out lymph drainage from the Eustachian tube, external auditory canal and deep areas of the face. Intraglandular and extraglandular lymph nodes normally do not exceed 9 mm in diameter.
Ultrasound imaging of otherwise unremarkable glandular parenchyma may reveal predominantly multiple hypoechoic lesions that often lack any distal signal enhancement. Sonographically, as a rule, it is impossible to obtain reliable signs that would allow a definitive differential diagnosis between benign and malignant enlarged lymph nodes.
Reliable differential diagnosis between reactive lymphadenitis (Fig. 5), non-Hodgkin's lymphoma (Fig. 6), MALT lymphoma, or intraglandular metastatic spread is not possible on the basis of sonographic findings alone.
Rice. 5. Pathological lymph node.
Rice. 6. Primary lymphoma of the parotid gland.
Clinical signs, number, location, and sometimes texture of nodes can lead to diagnosis, but do not replace histological analysis. As with enlarged lymph nodes of the neck, some authors mention the so-called “hilus” (gate) as a sign of reactive lymphadenitis.
Cystic tumors
Congenital or acquired salivary gland cysts are usually filled with clear fluid. We usually see an echo-negative tumor with clear borders and distal signal enhancement (Fig. 7).
Rice. 7. Salivary gland cyst (arrows indicate parotid gland, arrowheads indicate cyst).
It is important to note that if cystic tumors are detected sonographically in both parotid glands, and if there is a relevant medical history, then lymphoepithelial cysts caused by HIV infection should be suspected.
Sialolithiasis
Although the sign of a distal acoustic shadow is usually detected, the signal reflection can sometimes be unclear or insufficient. This phenomenon is the result of a reflected ultrasonic component that does not reach the transducer but is scattered out of the image plane. Typically, we see an echo-opaque object with a clear sign of a distal acoustic shadow (Fig. 8) and dilatation of the excretory ducts.
Fig.8. Intraglandular sialolithiasis of the submandibular gland.
Parotid duct stones contain organic components and are visualized with great effort. Sometimes only a distinct echo-opaque object without a distal acoustic shadow may be detected. However, in many of these cases, dilatation of the efferent ducts of the salivary glands can be considered as another indirect sign of the development of sialolithiasis, if the stone cannot be clearly identified. However, dilation of the duct can also be caused by scar changes in the connective tissue (for example, the situation after an inadequately performed incision of the duct or after acute inflammation). Stones with a diameter of 1.5 to 2 mm or more, located in the area of the large salivary glands, can be reliably detected during sonography.
It is important to note that the precise determination of the position of sialoliths (intraglandular, extraglandular and intraductal) is of great importance. Differential diagnosis is important both in the presence of air inside the ducts and in the case of pneumoparotitis, foreign bodies, angiolithiasis and calcified lymph nodes or arteriovenous malformations (Fig. 9).
Rice. 9. Arteriovenous malformation of the salivary glands.
Remember, because of its limited sensitivity and limited negative predictive value, sonography does not reliably exclude small salivary gland calculi. Further diagnostic studies are needed to identify stones in patients with normal sonographic findings and suspected lithiasis.
Sialadenosis (sialosis)
All large salivary glands can be simultaneously affected by sialoadenosis. Sialadenosis is a non-inflammatory condition characterized by bilateral enlargement of the salivary glands, most commonly the parotid glands. Usually we see that the glands look indistinctly enlarged, are difficult to differentiate from surrounding structures, their echo structure looks homogeneously hyperechoic, and with sialoadenosis tumor-like lesions are not detected. In some cases, the parotid gland is so enlarged that ultrasound requires a low-frequency transducer to evaluate the deep part.
Benign epithelial tumors of the salivary glands
A well-defined boundary between the surrounding salivary gland tissue and the tumor itself is a characteristic feature of a benign salivary gland tumor. Because ultrasound is unable to visualize nerves, the relationship of parotid tumors to the facial nerve cannot be reliably determined.
Pleomorphic adenomas have a homogeneous/hypoechoic texture. However, sometimes heterogeneous structures with hard and cystic inclusions may be noticeable. In these cases, a characteristic feature is distal signal enhancement (Fig. 10).
Rice. 10. Pleomorphic adenoma of the parotid gland.
Monomorphic adenomas (adenolymphomas) may also appear sonographically homogeneous and hypoechoic, as is the case with pleomorphic adenomas. If the proportion of cystic structures is high, adenolymphoma may also present completely without echo with extensive distal enhancement. Occasionally, septae may be identified within the tumor.
The remaining less common types of benign salivary gland tumors (eg, basal cell adenomas, oncocytomas, lymphoepithelial lesions) also have similar nonspecific sonomorphological features.
Definitive sonographic identification and differential diagnosis between different types of benign salivary gland tumors is currently impossible, although significant cystic portions in the mass tend to indicate adenolymphoma, and the absence of cystic areas indicates pleomorphic adenoma. To a certain extent, parotid tumors can be classified as either the "superficial" or "deep" part of the gland.
Benign nonepithelial tumors of the salivary glands
Lymphangiomas and hemangiomas (Fig. 11 and 12) have similar sonomorphological characteristics, which makes differential diagnosis between them impossible.
Rice. 11. Intraglandular lymphangioma.
Rice. 12. Submandibular hemangioma.
During the study, loosely connected alveolar structural components, consisting partly of hypoechoic and hypergeogenic areas, can be detected. Sonographic examination allows us to assess the depth of penetration and spread of this tumor into the corresponding salivary gland and into the area of surrounding soft tissue.
Intraglandular and extraglandular lipomas (Fig. 13) appear as sharply demarcated, ovoid formations, with a hypoechoic and homogeneous signal reflection pattern.
Rice. 13. Well-defined lipoma.
Lipoma has a more characteristic hypoechoic reflection pattern than the rest of the salivary gland parenchyma, but its echo texture is more hyperechoic than other types of intraglandular tumors, and it also has a linear hyperechoic feathery texture.
Malignant tumors of the salivary glands
We typically see a fuzzy edge and a patchy echo texture. It is possible to describe the relationship between invasive tumor growth and surrounding tissue. It is impossible to detect involvement of the facial nerve in the malignant process. The most common malignant tumors of the salivary glands are mucoepidermoid carcinoma, adenoid cystic carcinoma, carcinoma arising in pleomorphic adenoma, and distant metastases (Fig. 14).
Rice. 14. Metastatic melanoma in the parotid gland (arrows indicate parotid glands, arrowheads indicate metastases).
Indications for sonographic examination are sometimes absent, since at the preoperative stage it is impossible to identify with complete certainty the benign or malignant nature of tumor development. If a malignant process is suspected, ultrasound-guided fine-needle aspiration biopsy can be a useful tool to more accurately classify the tumor at a preoperative stage.
It is important to note that if tumor margins cannot be accurately imaged by sonographic examination, especially when the tumor extends to osseous or deep structures, the patient's diagnostic imaging should be extended in any case to computed tomography and/or magnetic resonance imaging.
Gougerot-Sjögren syndrome
Gougerot-Sjögren syndrome occurs when lymphocytes invade and destroy the exocrine gland. It is the second most common autoimmune syndrome after rheumatoid arthritis, affecting the salivary glands in 40-80% of cases. This results in a higher incidence of parotid lymphomas and salivary stone disease. Typically we see the following:
- At an early stage, sonography is normal.
- Later, the glands become enlarged and large-scale structural damage occurs.
- The gland is heterogeneous.
- At a later stage, sonographic examination reveals sialoectasia and marked hypervascularization on color Doppler ultrasonography of the salivary glands.
The intraoperative role of sonography has become important since the introduction of minimally invasive surgical techniques in salivary gland surgery. During surgery, if endoscopic observation of the surgical field is not possible, sonographic guidance can be used to:
|
Rice. 15. Minimally invasive procedures under ultrasound guidance.
Rice. 16. Therapeutic intraglandular injection of Botox.
Color Doppler ultrasonography of the salivary glands
The standard B-scan is a well-established tool for diagnosing salivary gland diseases. For tumors located in the salivary glands, there is increasing interest in non-invasive collection of clinical information such as growth and invasiveness, as well as making an accurate diagnosis before surgery. Before the benefits of sophisticated ultrasonography became available, standard testing was performed by correlating simple sonomorphological criteria, such as anechoic areas, with specific histological features. This can be easily achieved even if you buy a portable ultrasound machine .
Over the past few years, color Doppler sonography has become well established as an integral part of head and neck, ENT and maxillofacial surgery, especially as part of the preoperative evaluation of tumors and cervical lymph nodes.
Color duplex sonography
Color duplex sonography (Box 5) is a combination of B-mode sonography, pulsed Doppler sonography, and color coding of perfusion areas. The basic principle of color duplex sonography is the frequency shift of the transmitted signal, which is caused by reflection from moving red blood cells. The speed and direction in which red blood cells approach and move away from the transducer provide the information needed to perform duplex sonography.
| Box 5 Color duplex sonography
|
The ability to use Doppler signal amplifiers to achieve improved visualization of tumor vascularization has provided new opportunities for tumor characterization. Analysis of microvascularization and time-dependent changes after Doppler amplifier insertion, as well as elastography, are promising new tools for identifying features that help determine whether specific changes are typical for certain types of salivary gland tumors (Fig. 17).
Rice. 17. Study of the salivary glands using power Dopplerography.
The diagnostician should know the following:
|
Symptoms of the disease
Benign and malignant tumors of the salivary glands present with similar symptoms. One of the main differences is that cancer grows much faster and more often leads to a number of symptoms associated with growth into surrounding tissues and compression of nerves.
You need to visit a doctor if you are bothered by the following symptoms:
- A lump or swelling has appeared in the mouth, cheek, jaw, or neck.
- You have noticed that your face has become asymmetrical.
- I am worried about pain in the mouth, neck, ear, cheek, jaw. It doesn't last long.
- Numbness of part of the face.
- Weakness in the facial muscles, because of this, half of the face may be “lowered,” which becomes especially noticeable when baring teeth or frowning.
- I can't open my mouth wide.
- Difficulty swallowing.
Diagnostic methods
During the initial appointment, the oncologist talks with the patient, questions him, trying to find out risk factors, and conducts an examination. The doctor feels the tumor on the face and cervical lymph nodes, evaluates the sensitivity of the face and the work of facial muscles. After this, the patient can be referred for additional consultation to an ENT doctor.
Computed tomography and magnetic resonance imaging help assess the size, shape and location of the tumor, and detect lesions in the lymph nodes and other organs. The current gold standard for searching for distant metastases is PET scanning. If the tumor is located near the jaw, an x-ray is taken. A chest x-ray helps detect metastases in the lungs and evaluate the condition of the lungs and heart before surgical treatment.
The most accurate method for diagnosing salivary gland cancer is a biopsy. During this procedure, the doctor receives a fragment of pathologically altered tissue and sends it to the laboratory for cytological and histological examination.
The most common procedure is fine-needle aspiration biopsy. Tumor tissue is obtained using a hollow needle similar to the one used for injections. If the required amount of tissue cannot be obtained, the doctor performs an incisional biopsy: makes an incision and removes part of the tumor.
If tumor cells are found in the sample, the diagnosis of cancer is virtually certain.
How do they manifest themselves?
Symptoms of the disease completely depend on the location of the tumor and the involvement of surrounding tissues and organs in the pathological process, so they can be very diverse.
Initial manifestations:
- dense formation in the salivary gland or under the oral mucosa;
- long-term non-healing ulcer of the mucous membrane;
- moderate periodic pain is possible;
- discomfort when chewing or swallowing.
If the tumors are malignant, then at later stages the following may be observed:
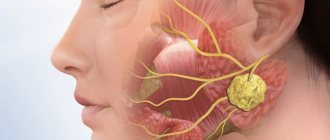
- facial asymmetry due to damage to the facial nerve due to parotid cancer;
- the appearance of dense, painless lymph nodes in the neck;
- redness and swelling of the skin over the tumor or lymph nodes;
- feeling of a foreign body in the throat;
- difficulty swallowing.
With metastasis to distant organs (lungs, liver, bones and others):
- weight loss for no reason;
- loss of appetite;
- nausea;
- constant weakness, fatigue;
- symptoms of damage to individual organs - shortness of breath, cough, hemoptysis, bone pain, jaundice, etc.
Classification: types of salivary gland cancer
The salivary glands are made up of different types of cells, any of which can give rise to a malignant tumor. Therefore, there are different types of cancer:
- Mucoepidermoid carcinoma of the salivary gland is the most common type. Most often it is found in the parotid salivary glands, less often in the submandibular and small ones. These tumors are rarely aggressive.
- Adenoid cystic carcinoma is characterized by very slow growth and rare metastasis. However, this malignant tumor can be very difficult to get rid of: it can recur a long time after treatment.
- Adenocarcinoma is a malignant tumor that develops from glandular cells. Different types of adenocarcinomas can occur in the salivary glands: acinic cell carcinoma, low-grade polymorphic adenocarcinoma, basal cell adenocarcinoma, clear cell carcinoma, cystadenocarcinoma, etc.
- Rare types of malignant cancers of the salivary glands include: squamous cell carcinoma, epithelial-myoepithelial carcinoma, anaplastic small cell carcinoma, undifferentiated carcinomas.
Stages of the disease
Salivary gland cancer, like other malignant tumors, is classified into stages according to the generally accepted TNM system. The letter T in the abbreviation denotes the characteristics of the primary tumor: the size and degree of its growth into surrounding tissues, N - spread to the lymph nodes, M - the presence of distant metastases. Depending on these indicators, the following stages are distinguished during salivary gland cancer:
- Stage 0 is “cancer in situ” (carcinoma in situ). The tumor is located within the layer of cells that form the salivary gland and does not grow into neighboring tissues.
- Stage I is a tumor that is located within the salivary gland and measures no more than 2 cm.
- Stage II - the tumor reaches a size of more than 2 cm, but not more than 4 cm.
- Stage III - a tumor that reaches a size of more than 4 cm and/or spreads into surrounding tissues, or a tumor of any size that has grown into surrounding tissues, has spread to one cervical lymph node on the same side, and the focus in the lymph node is no more than 3 cm and does not extend beyond its borders.
- Stage IV includes substages IVA, IVB or IVC. The first two are characterized by varying degrees of spread of the malignant tumor to the anatomical structures of the head, neck, and lymph nodes. If stage IVC is diagnosed, it means that there are distant metastases.
In addition to stages, there are three degrees of malignancy of salivary gland cancer:
- Grade I - low degree of malignancy. Such tumors are called highly differentiated. Tumor tissue is as similar as possible to normal salivary gland tissue. It grows slowly, and the prognosis for such patients is most favorable.
- Grade II are moderately differentiated tumors. Tumor tissue differs more significantly from normal tissue. This cancer is more aggressive and has a poorer prognosis.
- III degree - poorly differentiated tumors. Cancer cells almost completely lose the features of normal ones. Such tumors behave the most aggressively.
Determining the degree of malignancy helps the doctor predict how the cancer will behave and plan treatment correctly.
NORMAL ULTRASONIC ANATOMY
Parotid glands
The parotid glands, which are the largest of the salivary glands, are enclosed in a separate fascia, which penetrates the glands, forming various lobules. In cross-section, the parotid gland is a sharply defined, homogeneous organ with intermediate echogenicity (Fig. 1).
Rice. 1. Normal parotid gland.
The gland can be clearly distinguished from subcutaneous adipose tissue. The anterior part of the gland sits on the masticatory muscle and can be differentiated from the buccal adipose tissue, which has lower echogenicity, by contraction and relaxation of the masticatory muscles. The posterior part of the gland is located in the retromandibular fossa and is clearly delimited anteriorly by the ascending ramus of the mandible, and posteriorly by the sternocleidomastoid muscle and the mastoid process. Mediocaudal to the inferior pole of the parotid gland, the posterior belly of the digastric muscle and the internal carotid artery can be distinguished. It is important to remember that a small portion of the parotid gland may be hidden by the acoustic shadow of the mandible.
In and around the gland, the internal jugular vein and the retromandibular vein can be found, which are located in the glandular parenchyma and can be visualized, especially in the longitudinal projection. In transverse views, distal to the retromandibular vein, the styloid process is projected onto the glandular parenchyma, which should not be confused with sialolithiasis. The facial nerve is usually not visible. However, with the use of modern high-resolution transducers, it is sometimes possible to obtain a sonographic image of the main outflow canal.
Submandibular gland
The submandibular gland extends cranial to the mandible and the geniohyoid muscle and has a close connection with the anterior belly of the digastric muscle. The submandibular gland forms an arch around the posterior border of the geniohyoid muscle and often reaches ventromedial to the submandibular gland. Echogenic structures with an element of acoustic shadowing are often projected in the area of the gate of the submandibular gland. In this area, it is necessary to carry out differential diagnosis between the elements of the hyoid bone and the sialoliths of the submandibular gland, which may have comparable characteristics on imaging [2,7]. Sonographic imaging characteristics of the submandibular gland include an intermediate echogenic structure with a regular echo pattern corresponding to the echo pattern of the parotid gland parenchyma (Fig. 2).
Rice. 2. Normal submandibular gland.
In and around the gland, the facial artery and facial vein, which pass through the gland, are easily distinguished sonographically. The path of the efferent duct can sometimes be visualized using high-resolution ultrasound probes, even in the absence of duct obstruction. If we are talking about differentiation of the elements of the hyoid bone, then during swallowing movements its displacements are observed.
Sublingual gland
Visualization of the sublingual gland can sometimes be problematic. The sublingual gland is located under the mucous membrane in the oral cavity, lower in the projection of the tip of the tongue, next to the frenulum of the tongue. The dorsal part of the glands often touches the surface of the submandibular gland.
The gland is bounded ventrally and medially by the geniohyoid and genioglossus muscles, and caudally by the mandible. Short excretory ducts usually cannot be visualized. Accumulation of saliva may be found in and around the sublingual gland, which forms the ranula (Figure 3).
Rice. 3. Sublingual ranula.
Treatment
The patient is treated by a team of doctors, which may include: a clinical oncologist, an ENT doctor, an oncologist-surgeon, an oral and maxillofacial surgeon, a chemotherapist, a radiotherapist, etc. The treatment program is determined by the stage of cancer, the histological type of the tumor, its location (which gland is affected) , age, general condition and concomitant diseases of the patient.
Surgery
If the tumor has not grown much into the surrounding tissue, then it is resectable, that is, it can be removed surgically. The surgeon’s task is to excise the tumor while capturing the surrounding tissue so that there are no cancer cells left on the cut line, that is, to ensure a negative resection margin. If tumor cells have spread to the lymph nodes, or a biopsy reveals aggressive cancer, the lymph nodes are also removed.
For parotid salivary gland cancer, surgery presents certain difficulties, because the facial nerve passes through the gland, which controls the work of facial muscles. If the tumor affects only the superficial lobe of the gland, you can remove it separately - perform a superficial parotidectomy. There is no risk of damaging the facial nerve. In some cases, it is necessary to remove the entire gland, and if the tumor has grown into the facial nerve, then it too.
For cancer of the sublingual and submandibular gland, the surgeon removes the gland itself and some of the tissue located around it, including, possibly, bone tissue. In some cases, it is necessary to excise the nerves that control sensitivity, movements in the lower part of the face, in the tongue, and the sense of taste.
For cancer of small glands, the affected gland and part of the surrounding tissue are removed. The extent of the operation depends on the size and location of the tumor.
Radiation therapy
Indications for the use of radiation therapy for malignant tumors of the salivary glands:
- To combat malignant tumors that cannot be removed surgically due to their location or size. Sometimes radiation is supplemented with courses of chemotherapy.
- After surgical treatment. This type of radiation therapy is called adjuvant and is sometimes combined with chemotherapy. Radiation after surgery helps destroy remaining cancer cells and prevent recurrence.
- For advanced cancer. In this case, radiation therapy is aimed at combating pain, difficulty swallowing, bleeding and other symptoms.
Radiation is typically given five days a week for 6–7 weeks. If radiation therapy is used for palliative purposes, the course will be shorter.
Chemotherapy
Chemotherapy is used quite rarely for malignant neoplasms of the salivary glands. Anticancer drugs can reduce the size of the tumor, but are not able to completely destroy it. They are most often prescribed for advanced cancer as palliative treatment or in addition to radiation therapy.
Depending on the type and other characteristics of the cancer, the doctor may prescribe combinations of different chemotherapy drugs: carboplatin, cisplatin, 4-fluorouracil, doxorubicin, paclitaxel, cyclophosphamide, vinorelbine, docetaxel, methotrexate. Chemotherapy for cancer is always given in cycles. The patient is administered the drug, then takes a “break” for several days. The course of treatment may consist of several cycles.
Rehabilitation
After treatment, some problems associated with nerve damage may persist: dysfunction of the facial muscles, speech disorders, swallowing, and cosmetic defects. Some side effects of chemotherapy and radiation therapy go away after treatment is completed, while others persist for a long time. In such cases, rehabilitation courses are indicated. The doctor draws up a rehabilitation treatment program individually, depending on the severity and nature of the disorders.
Histology
The parotid gland has a lobular structure. Connective tissue septa extending from the fascia of the stomach divide its parenchyma into lobules, which in turn form 5-7 larger lobes.
Rice. 5. Schematic representation of the histological structure of the parotid gland. A - at a magnification of 200 times: 1 - intercalary duct; 2 - striated duct; 3 - terminal secretory department; 4—fat cell; 5 - interlobular duct; 6 - interlobular septum; 7 - blood vessel; hematoxylin-eosin staining; B - with a magnification of 600 times: 1 - fat cell; 2 - serocytes of the terminal secretory section; 3 - striated duct; 4 — myoepitheliocytes; 5 - intercalary duct; hematoxylin-eosin staining.
O.J. is a complex alveolar gland (see Glands). Its lobules are formed from terminal secretory sections tightly adjacent to each other - acini and excretory intralobular ducts: intercalated and striated (Fig. 5).
The terminal secretory sections are formed by glandular epithelial cells - serocytes, located on the basement membrane, consisting of a dense network of reticular fibers. The serocyte has a pyramidal shape, its cytoplasm contains a basally located rounded nucleus, a well-developed endoplasmic reticulum with numerous cisterns, a lamellar complex and secretory granules of various types.
In the terminal secretory sections of the lake. secretory tubules are distinguished, which are located between serocytes and have the appearance of thin tubes without their own walls.
Intercellular secretory tubules are characteristic of glands with protein secretion. The apical pole of serocytes, as well as their surface facing the intercellular secretory tubules, are covered with microvilli.
The terminal secretory sections pass further into narrow intercalary ducts lined with cuboidal epithelium, and then into striated ducts, or salivary tubes, lined with single-layer columnar epithelium. The characteristic basal striation of the epithelium of striated ducts depends on the accumulation of mitochondria lying between the folds of the plasmalemma of the basal part of the cell. It is believed that the striated ducts play a role in changing the concentration of primary saliva.
Between the cells and the basement membrane of the terminal secretory sections, intercalary and striated ducts there are myoepithelial cells, or basket cells, which are contractile elements that contribute to the secretion of secretions and maintaining the tone of the gland ducts.
Intralobular ducts pass into interlobular ducts, which run in layers of connective tissue between the lobules of the gland, merge with each other, forming interlobular ducts and, finally, the parotid duct. Interlobular ducts of the lake. lined with double-row prismatic epithelium, which, as the excretory ducts thicken, becomes multilayered. Along the parotid duct the epithelium is multilayered cubic, and at the mouth of the duct it is multilayered squamous.
Complications and relapses
Even if the treatment is successful and the examination results show no signs of the presence of cancer cells in the patient’s body, a relapse may occur in the future. Therefore, you need to regularly see an oncologist, come for examinations, undergo various studies and take tests.
Typically, the doctor prescribes examinations once every few months for several years, then less frequently.
- If cancer recurs, treatment options may vary:
- If the tumor can be removed, surgery is performed followed by a course of radiation therapy.
- If the tumor cannot be removed surgically, the doctor prescribes radiation therapy in combination with chemotherapy.
- If there are distant metastases, chemotherapy becomes the main treatment method. Radiation therapy and surgery can be used to control some symptoms.
With advanced cancer with metastases, achieving remission becomes extremely unlikely. In this case, treatment will be aimed at slowing the progression of cancer, combating symptoms, and prolonging the patient’s life.
Euroonco doctors undertake cancer treatment at any stage. For us there are no hopeless patients. You can always help, and we know how to do it correctly, we have all the necessary technologies, the latest generation drugs.