Removal of the parotid, submandibular gland, removal of cervical lymph nodes
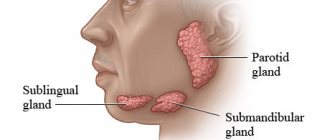
The salivary glands are divided into minor and major salivary glands. There are 3 pairs of large salivary glands: the parotid salivary glands, located below and in front of the auricle directly under the skin, the submandibular salivary glands and the sublingual glands, located under the mucous membrane of the floor of the mouth. The minor salivary glands are located in the mucous membrane of the mouth, palate, cheeks and lips. Various tumors, stones, and recurrent infections are the most common reasons for operations on the salivary glands.
Causes
- The presence of inflammatory processes in the oral cavity
- Mechanical factors, for example, trauma to the ducts from sharp edges of teeth or crowns
- Stagnation of saliva secretion
Currently, there are four methods aimed at eliminating stones from the salivary glands.
1. Interventional sialendoscopy.
The doctor uses a special instrument with a camera at the end - an endoscope - to remove stones from the salivary ducts. This procedure is performed under local anesthesia.
2. Extracorporeal lithotripsy.
Under the influence of ultrasonic influence on stones, they are crushed.
Thanks to this method, it is possible to extract and wash the ducts with a special solution, which will prevent the development of the inflammatory process.
3. Dissection of the duct is done if the stone is large and cannot be removed using a simple method.
4. Extirpation of the salivary gland.
This operation is used only when irreversible changes are observed in the parenchyma of the gland. The doctor performs the procedure in a hospital setting under general anesthesia.
Symptoms
A stone located in the duct of the salivary gland clogs the duct and prevents the flow of saliva into the mouth. In this case, saliva collects in the salivary gland, which becomes swollen and often painful. Depending on the location of the stone, pain and swelling occurs either under the jaw (submandibular gland) or in front of the auricle and in the area of the angle of the jaw bone (parotid gland). Some stones can be removed endoscopically through the mouth under local anesthesia as an outpatient procedure, but sometimes the entire salivary gland must be removed. Most often, stones are found in the submandibular gland.
The tumor is usually palpable as a nodule in the salivary gland and can cause swelling, pain, and facial nerve dysfunction. Even a benign tumor usually must be removed.
Indications
Indications for removal of the submandibular salivary gland are:
- chronic sialadenitis (inflammation);
- benign or malignant tumors;
- multiple cystosis;
- salivary stone disease;
- severe injury to the gland;
- complete blockage of the salivary ducts with the impossibility of restoring their patency.
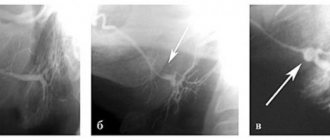
Depending on the diagnosis, various tests are prescribed before the operation - ultrasound, computed tomography or magnetic resonance imaging, chest x-ray. In the case of a tumor, a biopsy is also necessary to determine the nature of the formation. Salivary stone disease is examined using contrast sialography.
Salivary gland removal procedure
The operation to remove the salivary gland is performed under general anesthesia. The operation to remove the parotid gland lasts from 1 to 2 hours and the submandibular gland less than 1 hour.
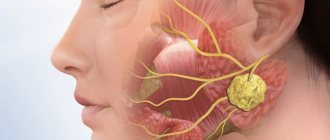
The facial nerve passes through the parotid gland and the inferior branch of the facial nerve is located in the surgical site. Therefore, when the parotid gland is removed, small needle cables are placed on the face for the duration of the procedure to identify the facial nerve.
During surgery to remove a tumor, we also try to remove nearby tissue, but this is not always successful due to the location of the facial nerve. The submandibular gland is usually removed completely.
Salivary gland cancer
Cancer of the major salivary glands in the initial stages is characterized by the appearance of a painless, round, dense tumor anterior to the auricle or in the submandibular region. In a fairly short period of time, it increases in size, ulcerates the skin of the face, and affects the facial nerve. The person’s smile becomes skewed, the nasolabial fold becomes smoothed, and the lower eyelid droops. There is lacrimation. Metastases to the cervical lymph nodes manifest as tumor-like formations on the lateral surface of the neck. Signs of distant metastases are determined by their location, most often dysfunction, pain.
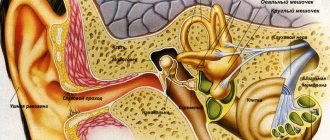
The stages of cancer are determined both by the degree of damage to the salivary glands themselves, and by the degree of damage to the cervical lymph nodes, as well as the presence of distant metastases. A primary tumor of the salivary gland is designated by the letter T: TX – there is insufficient data to evaluate the primary tumor, TO – the primary tumor is not determined, T1 – a tumor up to 2 cm in the greatest dimension without spreading beyond the gland, T2 – a tumor less than 2 cm but not more than 4 cm in the greatest dimension without spreading beyond the gland, T3 - tumor with spread beyond the parenchyma without affecting the VII nerve and/or from 4 to 6 cm in the greatest dimension, T4a - tumor more than 6 cm in the greatest dimension with spread to the mandibular bone, external auditory canal and/or with damage to the VII nerve, T4b - tumor spreads to the base of the skull, pterygopalatine space, internal carotid artery. The letter N denotes cervical lymph nodes: NX – there is insufficient data to assess the condition of the lymph nodes, N0 – there are no signs of metastatic lesions, N1 – metastases in one lymph node on the affected side up to 3 cm and less than 6 in the greatest dimension, N2 – metastases in one or several lymph nodes on the affected side up to 6 cm in the greatest dimension or metastases in the lymph nodes of the neck on both sides, or on the opposite side up to 6 cm in the greatest dimension, N2a - metastases in one lymph node on the affected side up to 6 cm in the greatest dimension, N2b – metastases in several lymph nodes on the affected side up to 6 cm in the greatest dimension, N2c – metastases in the lymph nodes on both sides or on the opposite side up to 6 cm in the greatest dimension, N3 – metastasis in a lymph node more than 6 cm in the greatest dimension. Letter M – distant metastases: MX – there is not enough data to determine distant metastases, M0 – there are no signs of distant metastases, M1 – there are distant metastases.
Grouping by stages of salivary gland cancer.
Complications after surgery
During surgery to remove the parotid gland, the facial nerve can be impacted, sometimes causing facial nerve palsy, usually the inferior branch, which can cause the corner of the mouth to droop. Typically, facial nerve paresis recovers within a few weeks with facial exercises, and only in rare cases does the facial nerve fail to recover.
Sometimes the cancer affects the facial nerve and then the facial nerve is completely removed, in which case the paralysis is permanent. However, the condition can usually be improved through various surgical interventions.
After removal of the parotid salivary gland, the pinna of the ear is usually partially numb, but over time some sensitivity returns. Due to the risk of frostbite, the auricle must be properly protected from the cold.
During surgery to remove the submandibular gland, the facial nerve may be injured (stretched), causing temporary dysfunction of the corner of the mouth, but permanent damage caused by this branch of the facial nerve is very rare. Damage to the sensory and motor nerves passing under this gland is extremely rare.
After parotid surgery, saliva may leak from the wound, especially when eating. Salivary secretion is harmless and usually ends spontaneously. Surgery to remove one salivary gland does not cause noticeable dry mouth.
Removal of cervical lymph nodes (cervical dissection)
When removing a malignant tumor of the salivary gland, the cervical lymph nodes are usually removed, a so-called cervical dissection is performed. The lymph node is usually small, surrounded by a bean-shaped capsule, and lymph fluid flows through it. There are a large number of lymph nodes in the neck.
The first metastases of salivary gland cancer are usually found in the cervical lymph nodes and therefore it is believed that their removal is necessary in the case of cancer. Typically, surgery to remove the salivary gland, which also involves a cervical dissection, takes 1 to 2 hours longer.
Submandibular gland
Removing the pancreas is an important surgical procedure. It is one of the two largest salivary glands in the human body, the other being the parotid gland. The most common reason for gland removal is due to recurrent infections and/or blockages that cause swelling (chronic sialolithiasis). Another reason is the presence of an abnormal mass contained in the gland (benign or malignant).
The pancreas and inflammation of the glandular ducts are the causes of swelling and, as a result, pain and discomfort. When a blockage occurs, backflow occurs, causing saliva to accumulate behind the occlusion. When this happens, the salivary glands swell in size. Over time (for example, between meals), the body resumes saliva production, and the saliva is compressed back and forth until the next meal, which activates the gland and produces more saliva, leading to the development of edema.
Initial (surgical) treatment is as follows:
Apply hot compresses to the widened area of the mouth two to three times a day. After applying the warm compress, give a very gentle (orthogonal) massage to the swollen areas.
Mix dry and sour candies. These sweets stimulate saliva production.
Increase your water intake to two liters per day. Try to avoid caffeine as it acts as a diuretic and can dehydrate the body.
The gland may or may not become infected. If there is inflammation, your doctor will prescribe an antibiotic, usually over a 3-week period. Use the antibiotic as directed and complete the full program even if symptoms subside.
Over the course of 3-4 weeks, the gland slowly returns to its normal shape. If the above precautions do not help, surgical removal is the next step.
If there is an abnormal mass, it may not change in size or even disappear. Unlike a blockage, swelling due to a mass does not change with food intake. Most masses grown in the submandibular gland are caused by benign tumors such as aphthoma or Warthin's tumor. These tumors are usually painless and move easily when palpated. Even if they are benign, tumors must be removed because they will not heal themselves and will continue to grow over time, causing facial distortion. Usually after decades, these benign tumors can also develop into cancer (carcinoma in pleural adenoma).
Unfortunately, some masses can be cancerous and include mucoepidermoid carcinoma, basal cell carcinoma, and metastases from skin cancer (squamous cell carcinoma is the most common). If there is pain, numbness over the chin or teeth, tongue or mouth, or facial paralysis, the likelihood that the mass is cancerous increases.
Typically, submandibular mass testing involves a CT scan as well as a fine needle aspiration (FNA) of the mass itself. Obtaining an FNA is useful in determining the extent of surgical removal. If malignancy is detected, a more extensive surgical procedure is required, including complete removal of the gland as well as surrounding lymph nodes (lymphatic clearance).
A common concern patients have regarding surgery is whether it will affect their saliva production. The answer is NO.
Sialolithotomy
In cases where there is a stone in the submandibular gland duct, an option you can try before removing the entire gland is a procedure called saliototomy. In fact, only the stone itself can be removed. If the stone is located near the mouth, this procedure can be performed at a local anesthesia clinic.
If the stone is more than 1.5 cm from the canal opening, the procedure must be performed in the operating room under general anesthesia. In this case, a small catheter is usually left in place to prevent scar tissue from closing the lumen and is removed after about 5 days.
Dangers of this process include infection and bleeding. A rare risk of this process is the development of scar tissue in the canal, which leads to recurrent swelling of the gland. There is also a small risk of numbness in the mouth.
Removal of submandibular glands
In cases where saliototomy cannot be used as an option or where a true mass exists, the entire gland should be removed. This is achieved by reducing approximately 3 cm below the body of the mandible to a length of approximately 4-5 cm. Anatomically, the omentum is prepared by carefully ligating the large vessels and preventing damage to the nerves. The defect is detected and it is ligated. The incision is closed with a plastic suture. The whole process takes about 1-2 hours.
Depending on how the surgery goes and how healthy the patient is, he may leave the clinic the same day or the next day. Surgical drains are usually removed within 24 hours and sutures 5-7 days after surgery. Pain after surgery is minimal, and in most cases people do not even need painkillers. Patients can eat as they please, but any exercise or heavy lifting is prohibited for the first 1-2 weeks after surgery.
Surgical risks include bleeding and infection. However, rare risks of subnuclear ablation include permanent lip paralysis, permanent tongue paralysis, and numbness in the lower part of the mouth.
Why is this happening? Because the nerves that go to the rim, tongue and larynx pass through the subeye and are at risk of injury.
Sometimes there may be temporary damage to the nerves and their function may return over time (weeks or months), but in some cases it may never return. The use of radio wave diathermy for vascular ligation and basal nerve conduction monitoring with a neurostimulator significantly reduces intraoperative and postoperative risk.
Endoscopic salnioscopy
Pancreatic endoscopy is performed by introspection, resulting in minimal (if any) incisions in the mouth or throat.
If you have problems with the submaxillary gland, please contact our clinic to schedule an appointment.