Reasons for education
The causes of this disease include previous injuries and inflammatory diseases of various etiologies. There are frequent cases of mucocele due to obstruction of the salivary gland of the oral cavity by stones. In an infant, mucocele symptoms can occur due to a number of different pathologies, such as atresia of the salivary gland ducts.
Experts do not have a consensus regarding the reasons for the development of ranulas - for example, many dentists believe that the frequency of formation of this pathology of the salivary gland is caused by the peculiarities of its structure. Others believe that the likelihood of this pathology occurring is determined genetically or at the stage of embryo development.
One of the significant reasons for the appearance of mucocele of the salivary gland is the habit of constantly biting the lower lip or injuring it in any other way. These constant mechanical microtraumas lead to the creation of a focus of infection and infection. Much less often, a tumor appears, for example, on the inner surface of the cheeks, on the upper lip or on the tongue.
Mucocele
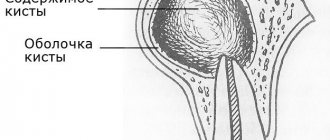
Mucocele is a benign, expansive cyst-like formation filled with mucus and lined with respiratory epithelium of the paranasal sinuses.
Etiology
: Mucocele is usually a complication of long-term sinus obstruction.
Pathogenesis
: It is believed that mucocele may cause obstruction of the opening connecting the sinus to the nasal cavity, which leads to the accumulation of fluid. Gradually, producing mucus, the mucocele increases in size and deforms the surrounding bone. The most common causes of mucoceles are chronic infections, allergic diseases, trauma and previous surgical interventions, while the causes of some remain unknown.
Epidimiology
: Most often affects the frontal sinus. About a third of all mucoceles are localized in the maxillary sinuses and cells of the ethmoidal labyrinth. The sphenoid sinus is rarely affected.
Clinical picture:
Since mucocele is a non-infectious lesion, its clinical symptoms are mainly due to the mass effect.
CT Imaging Data
Loss of airiness and increase in sinus volume with thinning of its walls. There may be erosions of the bony walls of the sinus.
MPT
• In most cases, mucoceles are hypointense on T1 and hyperintense on T2w images. In some cases, the sinus appears dilated, but with preserved airiness; it is hypointense on both T1 and T2.
Treatment:
surgical drainage.
Forecast
: favorable for early diagnosis and timely treatment.
Differential diagnosis:
Differential diagnosis presents certain difficulties. In the absence of bone erosion, mucoceles are distinguished from retention cysts, sinusitis and polyposis of the paranasal sinuses. In cases where bone damage is extensive, it should be differentiated from malignant conditions: spinocellular carcinoma, cystadenocarcinoma, plasmacytoma, melanocarcinoma, schwannoma and tumors of odontogenic origin.
Source
: Radiopaedia 1. Moritani T, Ekholm S, Westesson P. Diffusion-Weighted MR Imaging of the Brain. Springer Verlag. (2009) ISBN:3540787844. Read it at Google Books - Find it at Amazon 2. Mafee MF, Valvassori GE, Becker M. Imaging of the head and neck. George Thieme Verlag. (2004) ISBN:1588900096. Read it at Google Books - Find it at Amazon 3. Van tassel P, Lee YY, Jing BS et-al. Mucoceles of the paranasal sinuses: MR imaging with CT correlation. AJR Am J Roentgenol. 1989;153(2):407-12. AJR Am J Roentgenol (abstract) - Pubmed citation 4. Guttenplan MD, Wetmore RF. Paranasal sinus mucocele in cystic fibrosis. Clin Pediatr (Phila). 1989;28(9):429-30. — Pubmed citation Fidevs Akpek, researcher, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Ismail Akkas, Assistant Professor, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Orcum TOPTAS, Assistant Professor, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Fatih Ozan, Associate Professor, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey
Classification of salivary gland mucocele
Based on the location of formation and the course of the pathological process, dentists distinguish cysts of the minor and major salivary glands. If a mucocele is located on the lower lip, due to its origin it is divided into true and extravasal. A true, or, as they are also called, retention cyst does not have its own membrane, but is always covered with a gland capsule on top. The capsule is formed due to the fact that the duct of the salivary gland is clogged, and mucus stagnates.
Extravasal or post-traumatic neoplasm on the lower lip occurs due to a violation of the integrity of the external capsule, which was accompanied by the release of secretions into the external tissues. Absolutely all neoplasms-cysts of the salivary gland, regardless of the nature of their origin, are divided into two main categories:
- A true formation, the shell of which has an epithelial lining. The most popular location for retention cysts is the parotid-masticatory and submandibular areas.
- A pseudocyst lacking an epithelial base. This subtype also includes mucoceles of the salivary glands. They are most often diagnosed on the mucous membrane of the lower lip and in the sublingual area.
Unusual oral mucocele in a child
An oral mucocele is one of the most common benign tumors of the oral mucosa, and is a cavity filled with mucus, a secretory product of the salivary glands (muco means mucus, coele means cavity).
The mechanism of development of such pathologies usually comes down to two options: extravasation of mucus associated with a traumatic lesion, and retention of mucus as a result of obstruction of the minor salivary gland. When mucoceles are localized at the bottom of the mouth, they are called ranulae, since the inflammation resembles the cheeks of a frog. The most common location of mucocele is on the lower lip, there is no prevalence by gender and age of patients, the peak incidence occurs in the second and third decades, rarely occurring in children, which makes the diagnosis and treatment of pathology in this group quite difficult. Mucocele has common clinical features with many other tumors and ulcerations of the oral cavity, which requires a careful differential diagnosis. In this article, we describe an interesting and unusual clinical case of mucocele of the lower lip in a child, focusing on the etiopathogenesis, clinical presentation and various treatment options.
Clinical case
An 11-month-old boy was referred to the clinic with complaints of a “small ball” on his lower lip and associated difficulty sucking for more than 3 months.
The child was in good general health and showed no other symptoms. No bad habits or local trauma were detected. Clinical examination revealed the presence of a soft tissue nodule on the mucous membrane of the lower lip (Figure 1), which was similar in color to the mucous membrane and measured 5 cm at its widest diameter, was set on a wide base, had a soft consistency, clear boundaries and a smooth surface. Based on the medical history and clinical examination, a preliminary diagnosis of mucocele was made. After a thorough examination and obtaining written consent from the parents, an excisional biopsy was performed under local anesthesia. Due to the small age of the child, parents and an assistant took part in fixing the hands. Since the baby was constantly crying, this ensured that the mouth was always open. Infiltration anesthesia was administered around the formation (2% lidocaine with epinephrine 1:80,000, one carpule). Before the injection, anesthetic gel is applied topically for 2 minutes. The lip was then retracted using finger pressure to bring the mass into greater convexity. A thick silk suture is passed through the mass along the widest possible diameter, then a surgical knot is formed, followed by excisional biopsy using an electrocoagulator (Photos 2 and 3), thus minimizing pain and postoperative bleeding. On the first day after surgery, an analgesic was prescribed to eliminate possible pain after the intervention.
Photo 1: Mucocele on the lower lip of an 11-month-old child.
Photo 2: Excision of the formation using an electrocoagulator.
Photo 3: View immediately after surgery.
The tissue sample was sent for histopathological analysis, which revealed a large area of mucous secretion containing mucinophages, mucin containing cells, surrounded by a compressed connective tissue wall and developing granulation tissue (Figure 4). The diagnosis of mucocele was confirmed. After 2 hours, the patient began breastfeeding as usual. Recovery was uneventful with a return to a normal diet within a week.
Photo 4: Hematoxylin-eosin stain revealed keratinizing epithelium with underlying connective tissue consisting of a large accumulation of mucin surrounded by granulation tissue and chronic inflammatory cells.
The child was re-examined after 15 days, 6 and 12 months. No recurrence was observed after 12 months (Figure 5).
Photo 5: View of the surgical site 12 months after the intervention, without relapse.
Discussion
Yamasoba identified two main etiological factors that can lead to mucocele:
- Injury
- Salivary gland duct obstruction
Basically, it is physical trauma that can cause the secretion of the salivary glands to spill into the surrounding submucosal tissue. Then, due to stagnation of mucus, inflammation occurs. The habit of biting your lip and sticking your tongue are also aggravating factors for this pathology.
The extravasal type goes through three stages of development:
- At the first stage, mucous secretion is poured out of the duct into the surrounding tissues, and leukocytes and histiocytes are also detected.
- At the second stage, due to the presence of histiocytes, macrophages and giant multinucleated cells as a result of a reaction to a foreign body, granuloma develops. This stage is called the resorption phase.
- At the third stage, a pseudocapsule is formed from connective tissue without epithelium around the mucous formation.
The retention type of mucocele is often observed in large salivary glands. This happens due to stretching of the duct and block by a stone or dense mucosa. There is a relationship between the severity of the pathology and the degree of duct obstruction.
Clinical characteristics
Clinically, they are characterized as single or multiple, round, fluctuating nodules, varying in color from normal pink to dark blue, often asymptomatic. Tissue cyanosis and vascular block are associated with distension of the underlying tissue and the clarity of the collected fluid, which may produce a bluish color. Sometimes they can rupture, leaving a slightly painful erosion that heals within a few days. Parafunctions such as lip biting, lip sucking, and trauma explain why the lower lip is the most common location for extravasal mucoceles. They are mainly found in children and young patients with no gender predominance, and are also rarely observed in children under 1 year of age.
Diagnostics
The medical history and clinical studies allow us to make a diagnosis of superficial mucocele. The appearance of the mucocele is pathognomic, but a correctly collected history of the formation is also important: localization of the formation, history of trauma, frequent recurrence, variations in size, bluish tint and consistency. Typically, mucoceles are mobile formations of soft or elastic consistency, depending on the number of tissues involved in the formation of the pathology. Despite this symptom of fluctuation, a drained mucocele does not fluctuate, and a chronic mucocele fluctuates much less due to well-developed fibrosis. In the retention type of mucocele, the cystic cavity with well-defined epithelial walls is lined with cubic cells. This type shows less inflammatory response. The extravasal type is a pseudocyst without an epithelial wall and contains inflammatory cells and granulation tissue. But even in the absence of epithelial cover around the mucosa, good encapsulation is found.
Radiography is an important contribution to the diagnosis of ranula. Localization of such formations is carried out using CT and MRI. High levels of amylase and proteins can be determined by chemical analysis. Histopathological examination is critical to confirm the diagnosis and usually shows the presence of ductal epithelium, granulation tissue, mucin accumulation and inflammatory cells.
Mucocele clinically resembles many other tumor-like and ulcerative formations of the oral cavity, so differential diagnosis requires a careful approach. Palpation is also important to differentiate the formation from other pathologies. Lipomas and tumors of the minor salivary glands do not show fluctuations, while cysts, mucoceles, abscesses and hemangiomas do. A simple technique known as fine needle aspiration biopsy (FNAB) is very useful and informative, especially when angiomatous lesions are involved in the differential diagnosis.
Treatment
The most common treatment for this pathology is simple surgical excision. Other treatment options include CO2 laser ablation, cryosurgery, intralesional corticosteroids, micromarsupialization, marsupialization, and electrocoagulation.
There is no difference in the treatment of retention and extravasal mucocele. Small mucoceles are removed along with the marginal tissue of the gland, and in the case of large formations, marsupialization will help avoid damage to the labial branch of the mental nerve. Lacrimal catheters are used to dilate the duct and resolve retention-type mucocele obstruction. To prevent recurrence during mucocele excision, it is also necessary to remove the surrounding glandular acini, remove the formation below the muscular layer, and avoid damage to the adjacent gland and duct. If the fibrous wall of the mucocele is thick, the removed tissue is sent for histological analysis to exclude neoplasm of the gland. Micromarsupialization can be accepted as an alternative treatment method in pediatric practice, since this technique is relatively simple, painless and rarely leads to relapse. This technique (after disinfection and anesthesia) consists of pulling a thick silk thread through the formation along its largest diameter and then making a surgical knot. The suture is removed after 7-10 days, which is sufficient time for the mucocele to disappear. The advantage of the CO2 laser technique is to minimize recurrence and complications, as well as to quickly and easily ablate the formation. This method can also be used in patients for whom long-term interventions are contraindicated. The remaining alternative options have not objectively proven to be highly effective. The administration of corticosteroids and gamma-linolenic acid usually becomes necessary only with multiple mucoceles, when surgical excision of each formation is difficult to perform.
Conclusion
Mucocele is the most common benign lesion of the oral cavity. Since this pathology is painless, dentists often detect it during the next examination of the oral cavity. Treatment of mucocele is quite problematic, since the risk of relapse is very high. However, surgical excision with dissection of surrounding tissue and minor salivary glands can lead to positive and durable results.
Authors: Neha Bhargava, Prateek Agarwal, Nitin Sharma, Mayank Agrawal, Mohsin Sidiq, Pooja Narain
Diagnostics
The process of diagnosing this pathology includes a physical examination that reveals the presence of facial asymmetry, as well as a soft and elastic neoplasm that is painless on palpation.
Puncture of the salivary gland allows you to take a sample of its contents – a viscous yellowish liquid – for examination. Biochemical testing reveals an increase in salivary protein and amylase.
Ultrasound examination of the salivary gland is also used for diagnosis. It reveals the presence of a rounded neoplasm with smooth, clearly defined boundaries. To exclude the possibility of a false diagnosis (this is possible, since it is quite difficult to distinguish a true cyst from a pseudocyst), additional histological examination is recommended.
Symptoms
A mucous cyst (mucocele) is a thin sac filled with clear fluid. These formations are smooth in appearance and have a bluish-pink color. The size of the cyst can vary, but usually the width of the sac is about 5-8 millimeters.
A mucous cyst is usually not accompanied by any symptoms. There is no pain syndrome with mucocele.
Large mucoceles may interfere with chewing or speaking. There is also a chance that the cyst will burst, causing fluid to leak out of its cavity. In such a situation, infection cannot be ruled out.
Treatment
The main treatment method for mucocele is surgery. The operation is performed by making two converging incisions to help isolate the cyst and quickly remove it. After the operation is completed, stitches and a special pressure bandage are applied.
However, this method is good when localizing a tumor on the lower lip. If it is located in the sublingual region, the operation may be somewhat more complicated and include “husking” or cystectomy of the salivary gland, or removal of the tumor directly along with the salivary gland.
Since the tumor is covered with a thin membrane, it is not always possible to perform surgery to remove it. Only complete removal of the tumor along with the salivary gland can be considered a fairly reliable remedy.
Types of mucocele
There are two main types of mucocele:
- Oral mucous cyst. Such mucoceles develop exclusively in the mouth. They form near the openings of the salivary glands, often on the lips or floor of the mouth. A cyst in the mouth is known as a ranula. A cyst on the gums is called an epulis. They can also develop around holes made by piercings. Oral mucous cysts are more common in people under 30 years of age.
- Mucous cyst. A mucous cyst (mucocele) can develop not only in the mouth, but also in other areas of the body. These lesions appear as hard sacs near the joints of the fingers or toes. This type of cyst looks like an enlarged joint. They can also develop near the base of the nail. Mucosal mucous cysts are more often diagnosed in older people, usually over 70 years of age.
Treatment of mucocele
Treatment for mucous cysts is often not required. In most cases, a mucocele cyst will disappear on its own.
Under no circumstances should you try to remove a cyst yourself. This will create an open wound that can become infected. After healing, scars will remain. Over time, the cyst will burst on its own.
Rinsing with salt water will help disinfect the mouth and speed up the spontaneous disappearance of the mucocele.
You should try to avoid biting or sucking on the lips and cheeks, as this can cause complications.
You should see a doctor if the cyst causes discomfort or persists for more than a couple of weeks. A specialist can open the cyst with a sterile needle.
You can also remove a cyst using:
- Laser therapy. The cyst can be easily eliminated using laser radiation.
- Cryotherapy. By freezing the cyst, it can be easily removed
- Surgical intervention. In serious cases, the cyst can be removed through surgery.
A mucous cyst is usually removed surgically if it recurs.
Mucocele removal is usually a safe procedure. In rare cases, surrounding tissue may be damaged during the procedure.