What is a dental cyst?
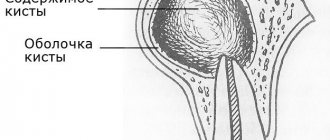
Tooth cyst - what is it? An odontogenic cyst is a pathological neoplasm that occurs in the upper part of the tooth root. The internal cavity of the cyst is filled with liquid or mushy purulent contents; it is enveloped by a dense layer of epithelium.
The size of the cyst starts from a few millimeters, with rapid development reaching several centimeters in circumference. Most often, the pathological process affects the upper jaw, since the roots of its teeth have a more porous structure.
In order to understand what a dental cyst is and how to treat it, you need to know why such a phenomenon occurs. The formation of cysts occurs as a result of inflammation, thus the body restricts healthy tissue from the affected areas, clogging them along with bacteria into bubbles.
Causes
There are several reasons why a dental cyst develops. The main reason is the activity of pathogenic microorganisms in a closed dental space; the following risk factors contribute to this:
- severe pathology, lack of timely treatment and incorrect treatment of dental diseases - caries, periodontitis, pulpitis;
- infectious complications after tooth filling, implantation procedures - in such cases, the doctor removes not only the cyst, but also the crown or implant, this avoids relapse;
- complications during teething, especially when wisdom teeth erupt - dental tissues injure the gums, bacteria get into microcracks,
- microorganisms also enter wounds that form due to mechanical damage to teeth;
- Nasopharyngeal diseases – infections in the nose and throat can spread to the oral cavity.
To provide adequate treatment, it is necessary to accurately determine the cause of the development of a dental cyst; based on it, the dentist will prescribe suitable therapy. So, in cases of injury, treatment consists of removing the cyst and tissue regeneration, but if the cyst is a complication of another disease, then in addition to removing the vesicle, the patient will be prescribed treatment for the underlying disease.
Types of dental cysts
Tooth cysts have different classifications, each of which is formed according to certain characteristic parameters of the pathology.
According to the nature of the disease, they are distinguished:
- residual cysts – occur after tooth resection (removal) surgery; this is the most common type of cyst;
- retromolar – formed during severe eruption of wisdom teeth;
- radicular - cysts are located on or near the tooth root;
- follicular – at the heart of such cysts is the germ of a permanent tooth; follicular neoplasms arise as a result of poor quality care of baby teeth.
Classification of neoplasms according to their origin:
- odontogenic – arise as a result of the transition of the inflammatory process from other dental diseases;
- non-odontogenic - the causes of the development of such cysts include problems not related to the teeth and oral cavity.
Locations of cystic formation:
- anterior teeth;
- teeth that are adjacent to the nasal sinuses with their roots;
- wisdom teeth.
How to avoid complications
To avoid missing a cyst in the early stages, check with your dentist at least once every six months, especially if your child has chronic pulpitis or periodontitis. The occurrence of cysts is most likely between the ages of 6 and 12 years, especially during the formation of the first molars in the lower jaw.
Teach your child proper and regular oral hygiene. This will reduce the likelihood of inflammation and caries in both milk and permanent teeth. For this, use high-quality children's toothpaste for a specific age. Asepta has developed Baby, Kids and Teens pastes that take into account the dental needs of children of different ages. For the little ones, specialized Asepta wet wipes designed in the form of finger pads are suitable - wipe the gums after each feeding.
It is necessary to treat infections and caries in a timely manner so that they do not lead to the formation of a cyst in the future.
Symptoms
The danger of a dental cyst lies in the fact that signs of pathology appear only when the neoplasm reaches a relatively large size. In the early stages, small cysts do not manifest themselves in any way, meanwhile the infectious process covers an increasingly larger area of healthy tissue. In the initial development of pathology, cysts are discovered by chance during routine examinations or treatment of other diseases.
The duration of the formation of a dental cyst takes only 1-2 days; as it develops, the following symptoms may occur:
- unpleasant and even painful sensations in the tooth, which intensify when chewing solid food;
- protrusion of the gum of a tooth, in the area of the root of which a cyst forms, the growth of the gum becomes larger over time, redness is observed;
- the formation of a fistula in the area above the root of the tooth, the release of serous or purulent accumulations from it;
- general weakness and malaise;
- increase in body temperature.
Note! When a dental cyst occurs, the symptoms are not immediately visible; they appear in the later stages of development. The pain when a tumor appears is aching in nature, but it is less pronounced than the pain caused by caries and pulpitis.
If a clinical picture occurs and you suspect a pathological process, be sure to consult a doctor. Under no circumstances should you resort to self-treatment - the dental cyst must be removed. In addition, taking the wrong medications can worsen the patient’s overall well-being.
Sometimes there is no pain in the oral cavity; instead, the basis of the clinical picture is intense headaches. The cause of this phenomenon may be a cystic formation in the maxillary sinus.
Symptoms of a maxillary sinus cyst
A cyst of the maxillary sinus does not have specific symptoms in the early stages; the first complaints appear when the tumor grows significantly (15 mm or more). The intensity of growth is an individual indicator for each patient, as is the severity of symptoms.
The main signs of a cystic formation in the maxillary sinus:
- Chronic nasal congestion on the affected side;
- Bursting sensations in the cheek area (closer to the eye);
- Persistent headaches, poorly controlled by analgesics;
- Accumulation of mucus at the back of the throat (especially in the morning);
- Intermittent mucous or clear nasal discharge;
- Frequent sinusitis with purulent discharge from the nasal passages;
- Pain when pressing on the causative tooth, redness and swelling of the gums;
- Facial asymmetry with pain in the anterior wall of the sinus.
Infection of the sinus by the odontogenic (that is, through the tooth) route most often develops in sinuses with a wide bottom and deep protrusions of the alveolar process into the jaw. The filling of the sinus with air is important - with moderate pneumatization, the risk of cyst formation is less.
During a diagnostic examination, the doctor identifies a hole in the bottom of the sinus. With an exacerbation of odontogenic sinusitis, sharp-smelling purulent masses are released from the nose, and upon rinsing, crumbly-granular white inclusions are found. An x-ray, as a rule, confirms the diagnosis of a maxillary sinus cyst, after which the doctor draws up a treatment plan.
Make an appointment
Types of operations
If a cyst of the maxillary sinus is detected, it will not be possible to limit oneself to therapeutic measures alone, but there is still a prospect of saving the tooth. The treatment of cysts is carried out by a dentist surgeon, who, based on the clinical picture and instrumental examination data, selects a surgical intervention technique:
- Cystectomy is an operation involving excision and curettage of the entire cyst cavity, followed by suturing;
- Cystotomy is an operation to excise the anterior wall of the tumor, and the doctor communicates the posterior wall with the oral cavity.
Indications for a specific technique are determined individually and depend on the type of cyst, the size of the neoplasm, and the number of teeth involved in the pathological process. Conservative treatment is possible only in the absence of obvious inflammation, it takes 3-4 months, but during this time the tumor can grow with the appearance of complications. That is why surgical opening of the sinus is considered the most reliable method of treating maxillary and other types of cysts.
Treatment of maxillary sinus cyst
Surgical activities carried out by a dentist in the clinic are aimed at:
- Relief of the inflammatory process;
- Elimination of the source of infection in the oral cavity;
- Removal of the root of a tooth with a cyst or extraction of the entire tooth;
- Sinus scraping, antiseptic treatment;
- Closing the communication between the oral cavity and the sinus;
- Creation of drainage for the outflow of liquid contents through the nasal passage.
First, the doctor determines which tooth caused the inflammatory process in the sinus, and the roots of several teeth may be affected. Using radiographs, the size of the sinus and the location of the cyst are analyzed, and the type of anesthesia is selected (usually local anesthesia with the latest generation of drugs). The surgeon will make every effort to save the tooth if possible. With shallow immersion into the cyst cavity, tooth-preserving operations (for example, root resection) show a good effect. When a tooth is immersed more than 1/3 of its length inside the tumor, it is recommended to remove it in order to prevent relapses of the disease.
The “Smile Factor” uses biocompatible modern materials to fill the cavity of the maxillary cyst, ensuring accelerated tissue regeneration. This tactic allows you to restore the jaw bone in a safe way; the prognosis for the intervention is favorable.
The protocol for working with the paranasal sinuses also includes a consultation with an ENT doctor. Treatment is considered successful when clinical symptoms of the disease disappear and there are no pathological changes in bone tissue on control radiographs.
Rehabilitation, features of care
After surgery, slight discomfort persists for 10-14 days. The turundas are removed from the nasal passages on the third day, and the sutures are removed after a week. Swelling, pain, difficulty breathing are temporary phenomena due to the specifics of the operation and do not require separate therapeutic measures. After removing the tampons from the nose, you should carefully follow the doctor’s instructions regarding rinsing the passages with antiseptics. Antibiotic therapy and instillation of vasoconstrictor drugs are prescribed.
During the first month after surgery it is recommended:
- Sneeze and cough gently with your mouth open;
- Follow a gentle diet with a predominance of soft foods;
- Limit intensive nose blowing;
- Avoid active facial movements;
- Postpone visiting the bathhouse, sauna, swimming pool;
- Do not go under water (even in the bathroom);
- Temporarily limit sports training;
- Sleep with the head of the bed raised on a comfortable pillow.
After treatment, you should visit the dental clinic once every 3-4 months throughout the year. During examinations, the attending physician monitors the progress of recovery, preventing relapses.
Possible complications
Treatment of a maxillary cyst should be carried out exclusively in a properly equipped clinic. Home measures to “resolve” the tumor are ineffective, and in many cases they contribute to the accelerated growth of the cyst due to improper actions by the patient.
Failure to contact a dental surgeon in a timely manner can result in serious consequences:
- Spread of the pathological process to healthy teeth followed by their loss;
- Penetration of infection into other air sinuses of the skull;
- Melting of the bone by purulent masses with the occurrence of osteomyelitis;
- Visual impairment, “double vision” due to compression of the eyeball by the cyst;
- Pronounced facial asymmetry with very large sinus tumors;
- Pathological fracture of the maxillary bone due to tissue thinning;
- Exhausting headaches, respiratory dysfunction, chronic malaise.
The most serious complication of a maxillary sinus cyst is considered to be the spread of inflammation to the membranes of the brain and the brain itself, which is extremely dangerous for the patient’s life.
Preventive actions
The following measures will help prevent the occurrence of a maxillary cyst and minimize the risk of complications with existing tumors:
- Sanitation of the oral cavity with competent treatment of teeth and gums;
- Timely treatment of ENT diseases (rhinitis, etc.);
- Correction of a deformed nasal septum;
- Treatment of allergic rhinitis;
- Early seeking medical help at the first symptoms of the disease.
Smile Factor doctors have modern techniques for treating jaw cysts of any size. Particular emphasis is placed on the painlessness and safety of the intervention, which is achieved by using proven drugs and consumables.
The patient receives competent advice during the rehabilitation period, so that recovery proceeds with maximum comfort. The exact price of treatment for a dental cyst is determined by the amount of work, type of surgery and other factors.
Consequences
Without adequate treatment, the dental cyst continues to grow and develop; in advanced stages, large neoplasms destroy the bone tissue of the skull, as a result it is replaced by connective tissue formations, which leads to the development of the following complications:
- dissolution of the jaw bone, which depends on the growth of the cyst;
- the formation of pus in the cyst, further purulent inflammation can lead to the development of an abscess;
- inflammatory process of lymph nodes located near the source of infection;
- development of osteomyelitis or periostitis;
- development of chronic sinusitis when the cyst grows in the maxillary sinus;
- pathological fracture of the jaw bones when the cyst reaches a large size;
- development of phlegmon due to a long-term purulent inflammatory process in the cyst;
- sepsis – blood poisoning;
- degeneration of a cyst into a malignant tumor without timely treatment.
Many patients are interested in why a dental cyst appears in the maxillary sinus, how dangerous it is and its symptoms. The formation of a cyst of this type occurs as a result of untreated inflammation of the tooth root in the upper jaw. A granuloma forms at the root of the tooth, which increases in size and becomes a peri-radicular cyst, then takes a position in the maxillary sinus. The volume of such a cyst can reach 9-12 cubic centimeters.
The symptomatic picture includes painful sensations, the nature of which is similar to trigeminal neuralgia, pain in the occipital, temporal and parietal regions of the head. Externally, a dental cyst can be identified by the asymmetry of the face. Tooth cyst - photo shows a cyst in the maxillary sinus.
Complications with cyst growth
Tooth trauma, advanced caries, nasopharyngeal or periodontal disease, dental malformations - one or more of these factors can lead to the development of a cyst. The danger is that the cyst grows unnoticed. It usually does not hurt and at the initial stage does not cause discomfort or reaction of the lymph nodes. With further development, suppuration and various unpleasant sensations may appear. But even if there is no pus, the cyst is very dangerous. Therefore, do not delay treatment.
A cyst can lead to intoxication of the body due to the fact that waste products of harmful microorganisms enter the blood. The consequence of this can be headaches, high fever and, in the worst case, sepsis.
In addition, complications are caused by local problems - phlegmon, abscesses, osteomyelitis. These complications are inflammatory in nature and often occur when the cyst suppurates. The spread of pus can lead to destruction of the jaw bones, damage to the internal organs of the digestive system, liver, and heart.
It is impossible to avoid the appearance of a cyst, but if you properly care for baby and permanent teeth and treat infections in a timely manner, you can reduce the likelihood of its occurrence. In addition, periodic visits to the dentist will allow you to notice the problem at an early stage, when treatment will be as simple and easy as possible for the body.
Diagnosis of tooth root cyst
To make a diagnosis and carry out appropriate treatment, the dentist collects and analyzes the medical history. During the initial diagnosis, many patients report the fact of endodontic treatment performed to eliminate periodontitis or pulpitis. Some patients indicate an exacerbation of the disease after intraoral dissection.
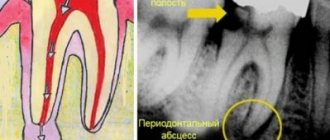
Radiography is used as the main diagnostic method. Below is a photo and x-ray of a dental cyst.
To obtain an x-ray, several methods are used, the first method is based on contact intraoral x-ray, the advantages of this technique:
- determining the degree of destruction of the jaw bones;
- assessment of the condition of the tooth root and tooth canal;
- assessment of the quality of canal filling;
- identifying the presence of perforations and fragments of instruments and materials in the tooth canal;
- determination of the relationship between the cyst and the roots located near the teeth.
The second method of performing radiography is an orthopantogram; the procedure is a panoramic photograph of both jaws and the maxillary sinuses of the upper jaw.
Another method of the procedure is a survey X-ray in the nasomental projection; the X-ray covers the bones of the skull from the nose to the chin; using the image, the doctor assesses the condition of the maxillary sinuses and detects cysts that have grown into the nasal cavity.
In addition to radiography, to detect a tumor, the patient may be prescribed an electroodontic diagnostic procedure. This technique helps to assess the degree of such an indicator as the electrical excitability of the teeth that are located next to the cystic tooth. If the value exceeds 60 microamps, the dentist prescribes endodontic treatment to the patient.
For diagnostic purposes, histological and cytological studies are used to determine whether the neoplasm is benign or malignant.
Diagnosing a dental cyst is not difficult, but only qualified dentists can carry it out in a hospital setting; under no circumstances try to independently determine the presence of a cyst and do not take therapeutic measures; strictly follow the doctor’s recommendations.
Eruption cysts
Eruption cysts are a type of soft tissue benign cysts associated with the eruption of primary or permanent teeth and appear before the appearance of these teeth in the oral cavity. This is a soft tissue analogue of retention cysts, but which belongs to a separate nosological unit.
Retention cysts develop around the crown of unerupted teeth embedded in the bone. Cutting cysts occur when the tooth has already begun to erupt through the soft tissue covering the bone.
The exact etiology of eruption cysts remains unclear. Agulio and others, in their retrospective studies, mention caries, trauma, infection, and lack of space for eruption as possible causative factors.
Despite the large number of theories of origin, cysts arise from the enamel epithelium of the tooth crown due to the accumulation of fluid or blood at the site of the follicle.
Analysis of the literature shows the infrequent occurrence of eruption cysts. Such data may be obtained due to the fact that many cysts appear and then disappear undetected, while dentists see only clinically manifested pathologies. Anderson reports 54 histologically confirmed cases over the past 16 years. Agulio data - 36 cases retrospectively analyzed over 15 years. Somewhat later, Bodner discovered the prevalence of eruption cysts in the form of 22% of all cystic formations of the upper jaw in 69 children. Bonder recently presented 24 new cases of eruption cysts in 2004.
Eruption cysts and hematomas usually occur in the first or second decade of life. Reports show that eruption cysts most often occur between the ages of 6 and 9 years, a period associated with the emergence of the first permanent molars and incisors.
Eruption cysts more often affect the right side than the left, and more often in men than women. However, Pinkham reports no gender predisposition.
Agulio in his study showed that 2.8% of eruption cysts occur in the incisor and molar areas, and 17.2% in the canines and premolars. Other scientists confirm the data presented, and explain the predominance of the incisor zone over the molar zone in a ratio of 2:1 by a better view of the anterior area.
Clinically, the disease appears as a rounded, fluctuating, often radiolucent swelling of the alveolar margin at the site of tooth eruption. In cases where the cavity surrounding the crown contains blood, the swelling appears purple or dark blue, hence the term eruption hemangioma. Differential diagnosis would include hemangioma, neonatal alveolar lymphangioma, pyogenic granuloma, amalgam staining.
On an x-ray, it is quite difficult to determine the cavity of an eruption cyst, because both the cyst and the tooth are located in the soft tissues of the alveolar process, and the bone remains unaffected, in contrast to a retention cyst, which looks like a well-contoured monocystic radiolucent crescent-shaped cavity above the crown of an unerupted tooth.
Histologically, this cyst has the same microscopic characteristics as a retention cyst: connective tissue covered with a thin layer of non-keratinizing epithelium.
Most of these cysts go away on their own and usually do not require special treatment. If the formation is painful, bleeding or infected, surgical excision is indicated to expose the tooth and drain the contents.
Description of clinical cases
We present two cases of eruption cysts in patients who sought treatment at our clinic.
Clinical case 1
The parents of an 8-year-old boy contacted the Department of Pediatric Dentistry with complaints of bluish swelling of the gums in the anterior segment of the upper jaw (Photo 1).
Figure 1: Preoperative photo showing an eruption cyst in area 21
The patient's parents were frightened, suggesting a malignant tumor. The medical history revealed that 61 were removed 1 year ago due to caries. The lesions began to appear 2 weeks ago as a radiolucent swelling on top of the normal mucosa, which slowly increased to its present size. The color of the mass has slowly changed from normal pink mucous to a true bluish-black color over the past week. No other changes or symptoms were observed. A general examination revealed no pathologies. There was no history of acute infections, trauma, or drug or food allergies. An examination of the oral cavity determined the child's mixed bite. All first permanent molars had already erupted; all but 21 incisors were in various stages of eruption. Carious lesions were found 52, 62, 73. Examination of the soft tissues of the oral cavity revealed no pathologies, with the exception of swelling in the area 21. Clinically, the gingival lesion looked like a bluish-black, round, fluctuating formation on the buccal side of the gums in the area of unerupted 21. The size of the swelling is approximately 1 ,5x2 cm, soft consistency. The overlying mucosa is smooth and without ulceration. X-ray examination confirmed the process of eruption 21 without pathological involvement of bone tissue or tooth. Clinically and radiologically, eruption cyst 21 was diagnosed.
The clinical situation was explained to the parents and advice was given to observe the swelling for the next 2 weeks, since the formation could resolve on its own without surgical intervention. The patient's appointment is scheduled in 15 days. The swelling remained, and a dull pain occurred when chewing. The meaning of the surgical procedure was explained to the parents and consent was obtained. Before the intervention, a blood test was performed. Treatment included excision of the eruption cyst and drainage of the contents. An incision was made 21 for easier cutting. Postoperative recommendations were given (Photo 2).
Photo 2: Cut made and exposure 21
The patient was observed a week later and normal eruption was observed.
Clinical case 2
An 8.5-year-old girl came to the clinic with complaints of a bluish-black discoloration of the gums, as well as swelling in the anterior segment of the upper jaw (Photo 3). Some change in sensitivity was also observed. The mass began to appear 2 months ago as a radiolucent swelling on top of the normal mucosa and slowly increased to its present size. There was a dull pain when chewing.
Figure 3: Preoperative photo showing eruption cyst in area 21
General physical health of the child without pathology. Examination of the oral cavity revealed a mixed bite. All but 21 permanent first molars and central incisors had erupted.
The dimensions of the swelling are approximately 2.5x2.5 cm. The consistency is soft and fluctuating. The overlying mucosa is smooth and without ulceration. X-ray examination confirmed that 21 was in the process of eruption without pathological involvement of the surrounding bone or tooth. Clinically and radiologically a diagnosis of eruption cyst 21 was made.
Surgical treatment was applied, the tooth was exposed. Subsequently, normal eruption was observed (Photo 4).
Photo 4: Cut made and exposure 21
Discussion
An eruption cyst is a soft tissue analogue of retention cysts, but is defined as a separate nosological unit. Clinically, an eruption cyst appears as a dome-shaped swelling on the mucous membrane of the alveolar margin, soft in consistency with a color ranging from blue, purple to blue-black.
During X-ray examination, it is quite difficult to determine the cystic cavity, since the cyst and tooth are located in the soft tissues of the alveolar ridge, without affecting the bone, which distinguishes an eruption cyst from a retention cyst, which is characterized by a clear monocystic radiolucent crescent-shaped zone near the crown of an unerupted tooth.
Histologically, this cyst has the same microscopic characteristics as a retention cyst: connective fibrous tissue with a thin layer of non-keratinizing epithelium.
Most eruption cysts do not require special treatment and disappear on their own. Surgery is necessary when there is pain, bleeding, infection or aesthetic problems. Treatment should be carried out to improve the child's quality of life. The high frequency of occurrence of such cysts, as well as localization in dynamically changing places, puts forward requirements for fairly conservative treatment in the population of young people. Surgery is not always indicated, as cysts may resolve on their own and be accompanied by normal tooth eruption. If this does not happen, simply excision of the roof of the cyst allows for faster eruption. Partial or complete excision of the underlying tissue and drainage of the cavity is indicated when eruption is inhibited or the cyst increases in size.
In case 1, a wait-and-see approach was adopted because the mass did not cause discomfort and the mass was expected to resolve on its own. But after 15 days, upon repeated treatment, the cyst continued to increase in size. Therefore, a decision was made to surgically excise and expose the crown.
In clinical case 2, excision of soft tissues followed by compression of the cyst was associated with a large size of the formation and a long duration of the disease. The swelling was observed for a long time, caused pain and gradually increased, so surgical tactics were immediately chosen.
New treatment technologies using Er, Cr-YSGG lasers have been proposed by Boj and other scientists. Advantages over standard techniques include no need for anesthesia, minimal bleeding during surgery and patient comfort. In clinical practice, the use of such equipment is limited by high cost and complexity.
Conclusion
Disturbances in the development of teeth can manifest themselves as anomalies in the form of various swellings of the mucous membrane, cysts of the eruption of temporary and permanent teeth in childhood. Eruption cysts are associated with erupting teeth and can vary in size, color, and morphology. Such formations can cause cancerophobia in children and their parents. Knowledge of this pathology among specialists is very important for making the correct diagnosis and choosing the appropriate treatment.
Authors: Preeti Dhawan, Gulsheen Kaur Kochhar, Sanjay Chachra, Shweta Advani
Treatment
Treatment of dental cysts is carried out through surgery, laser treatment and conservative therapy. The latter has a positive effect only in the initial stages of the disease; overgrown cysts must be removed.
Surgery
To eliminate the pathology, it is not necessary to remove the entire tooth; only the tooth root on which the cyst is located is subject to resection. After removing the affected area, the dentist seals the remaining root, treats the surgical canal through which he removed the bladder with its contents, and stitches it up.
After a few days, the doctor removes the stitches and monitors the wound healing process. It is important to make sure that there are no cyst particles left in the dental canal; to achieve this goal, repeat radiography is performed.
Note! Sometimes it is impossible to remove the root along with the cyst; in these cases, the doctor completely removes the tooth. Indications for complete tooth resection are a difficult-to-reach location of the cyst and a severe course of the disease.
After surgical removal of a cyst, the patient must regularly visit the dentist and follow the recommendations prescribed by the doctor.
Conservative therapy
Tooth cyst - treatment of the disease with conservative methods is possible only in the early stages of its development. In order to eliminate the tumor, the patient is prescribed injections and rinses.
During therapeutic treatment, the dentist opens the dental canal, which leads to a cystic neoplasm, and pumps out exudate from it. The doctor does not fill the canal for ten days; during this period, the patient uses antiseptic solutions and tinctures to rinse the mouth.
Upon completion of the treatment course, the dentist treats the dental canal with medications and then fills the tooth.
Laser removal
Laser treatment is a modern method of treating dental cysts. When performing the method, the doctor opens the dental canal and uses laser irradiation to treat the area where the cystic tumor is located. The laser destroys not only the epithelium of the cyst, but also hundreds of thousands of bacteria that are inside the bladder.
The advantages of laser removal are rapid tissue healing and no risk of secondary infection in the oral cavity and dental canal.
Treatment with antibiotics
In some cases, dental cysts are treated with antibiotics. Taking antibacterial drugs is an auxiliary measure to destroy an expanded infection or the main method of treatment if a dental cyst develops against the background of a primary infectious disease.
Antibacterial drugs can only be prescribed by the attending physician; the following drugs are most often used:
- amoxicillin – has a high antibacterial effect, greatly facilitates the treatment of cysts with other methods;
- Cifroploxacin is a broad-spectrum antibiotic that actively destroys bacteria and relieves inflammation;
- tetracycline - this drug is prescribed more often than others, it actively relieves the inflammatory process, pain syndrome, and facilitates other methods of treating dental cysts.
Sometimes a doctor can prescribe topical antibacterial agents to a patient, but taking such medications is not always advisable - local drugs - antibiotics are quite difficult to distribute evenly over the diseased area.
Note! Antibacterial drugs are potent drugs that also affect beneficial bacteria in the body. You can take such medications only as prescribed by a doctor, without increasing the number of doses or dosage.
Treatment at home
Treatment of dental cysts at home is possible only as an auxiliary therapy. A cyst should not be confused with a granuloma; the latter can resolve on its own, but the cystic formation must be radically removed. Home treatment is not used to remove the cyst, but to eliminate the inflammatory process and destroy harmful bacteria.
The main goal of therapy at home is to provide an antiseptic effect. Propolis tincture, calendula tincture, eucalyptus tincture have an antiseptic effect. Tinctures are used as follows: a small amount of medicine is applied to a cotton swab and applied to the affected area, held for 5-10 minutes.
Medicines with an antiseptic effect can be used before surgery to remove a cyst and after tooth root removal. The antiseptic effect allows these medications to be used in the treatment of caries and other infectious diseases of the oral cavity.
Prevention
It is always easier and faster to prevent any disease than to cure it, so one should not forget about simple preventive rules that will help avoid the development of a dental cyst. The basic rules for preventing dental cysts are based on compliance with the rules of oral care.
How to prevent the formation of pathology:
- do not trigger the course of dental diseases such as caries, periodontitis, pulpitis; if infections occur, consult a doctor immediately;
- Brush your teeth daily and prevent the appearance of plaque, which can later transform into tartar;
- monitor the condition of the teeth and oral cavity after operations and mechanical injuries;
- visit your dentist regularly;
- monitor the condition of filled teeth and dental implants;
Patients who have had their teeth filled or have dental crowns or implants placed are advised to periodically have dental x-rays taken. This will allow timely detection of pathological changes and increase the chances of successful recovery without serious consequences.
Note! All diseases must be treated in a timely manner; inflammatory processes reduce immunity, as a result of which infections move freely from one organ to another; in addition, secondary infections can be added to already developed pathologies. It is important to monitor your health and strengthen local and general immunity.
To strengthen your immune system, strengthen your body, include fresh fruits and vegetables in your diet, play sports and walk outdoors more often. It is more difficult for any infection to get into a hardened body than into a weakened body.
Causes
The key reason for the formation of a maxillary sinus cyst is dental disease. Especially when treatment was not carried out or performed poorly. Pathology develops against the background of advanced caries, periodontitis and pulpitis on chewing units. This is due to anatomical features. Premolars and molars are located closest to the paranasal sinuses and are separated from them by a thin septum.
Until recently, teeth with cysts were subjected to extraction. Today, dentists prefer to perform organ-preserving surgeries. All stages of work are performed under control using a dental microscope.
An endodontist removes the cyst, performs sterilization and filling of the canals.
The formation of a tumor can be caused by a deviated nasal septum, jaw abnormalities, or chronic blockage of the ducts of the nasal glands due to rhinitis or sinusitis.
Diagnosis of the disease
A neoplasm measuring up to 15 mm is diagnosed only with a CT scan. A dentist can suspect the presence of a pathology during a routine examination of the patient’s oral cavity based on existing complaints.
Clinical symptoms
As the cyst grows, the patient develops alarming symptoms similar to those of acute sinusitis. These include:
- acute headache;
- chronic nasal congestion;
- clear or yellow nasal discharge;
- a feeling of heaviness and fullness in the area under the eyes;
- the presence of a viscous mucous lump in the throat after waking up.
Clinical symptoms become more pronounced as the lumen in the nasal cavity closes. If there are concomitant dental problems, pain in the tooth and swelling of the gums occur.
Potential Complications
If left untreated, the infection spreads to adjacent teeth in the upper jaw. There is a risk of bone deformation or jaw fracture, the development of an abscess, phlegmon and other purulent complications.
The cyst is accompanied by sinusitis and chronic sinusitis. The growth of the tumor is dangerous due to visual impairment. The formation of a purulent cyst can lead to the development of meningitis or encephalitis.
Complex treatment
When treating pathology, dentists use medicinal and surgical techniques. The tumor is removed during surgery. Further drug therapy is designed to eliminate the symptoms of the inflammatory process and prevent complications.
Treatment in dentistry
Most patients go to the dentist when the size of the cyst exceeds 1 cm. The dental surgeon removes the bag of pus by cystectomy or cystotomy. The choice of technique is based on the size of the cyst and clinical indications.
The dentist is faced with a number of tasks:
- remove the source of inflammation in the oral cavity and stop the inflammatory process;
- provide drainage for the outflow of pus;
- if possible, save the diseased tooth;
- fill the resulting cavity with bone material;
- close the fistula between the oral cavity and the sinus.
Inpatient treatment in the ENT department
If the appearance of a cyst is caused by ENT pathologies, you should consult an otolaryngologist. Tumors are removed by surgery, laser or gentle endoscopic techniques. During endoscopy, the doctor gains access to the affected area through the nasal passages or an opening in the facial wall of the maxillary sinus. Control of manipulations on the monitor screen is carried out.