Problem: a 13-year-old patient complained of a “ball” on her lip - it turned out to be a retention cyst on the lip.
Solution: surgical treatment of a retention cyst of the minor salivary gland was performed using a laser. The result of treatment is complete healing. (The photograph shows a view 1 month after laser removal of the cyst.)
Mucocele - symptoms and treatment
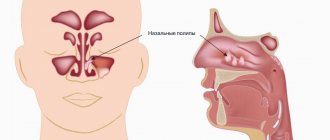
Mucocele is a stretching of the paranasal sinus by the thick secretion of the glands of the mucous membrane accumulated in it, which is accompanied by the gradual destruction of the bone walls of the sinus.
Over time, the contents of the sinuses bulge into neighboring areas and compress the organs located there. For example, due to pressure on the eyeball, vision deteriorates and the image doubles. If the lacrimal sac is compressed, uncontrollable lacrimation occurs. When the optic or trigeminal nerves are affected, pain in the orbit, upper jaw, or teeth occurs, as well as persistent headache. In addition, cosmetic defects of the face occur: protrusion near the inner corner of the eye or in the forehead, displacement (protrusion) of the eyeball.
The first mention of mucocele appeared in the 17th century, but scientific study of the problem began much later [11]. In 1895, Russian ophthalmologist Sergei Selivanovich Golovin summarized the literature data on 64 cases of the disease and for the first time reported cyst-like formations penetrating into the orbit from neighboring areas.
Such outstanding otolaryngologists as Vladimir Ignatievich Voyachek (1912) and Nikolai Dmitrievich Khodyakov (1928) also studied this condition. However, due to its rare occurrence, even the most thorough domestic work devoted to this disease, the monograph by Andrei Gavrilovich Likhachev (1948), summarized the results of treatment of only 45 patients operated on over 50 years. Only the advent of computed tomography made it possible to improve the detection of the disease, led to its active study and the development of new approaches to treatment.
The paranasal sinuses are air cavities that communicate with the nasal cavity through openings and canals. In the frontal bone there is the frontal sinus, in the cells of the ethmoid bone - the ethmoid, in the bones of the upper jaw - the maxillary (maxillary), in the body of the sphenoid bone - the sphenoid (main).
Humans are born with the rudiments of the paranasal sinuses. The ethmoid sinuses are the first to form. After 3 years, the maxillary sinuses are clearly visible, later - the sphenoid sinuses. The last to develop are the frontal sinuses.
Reasons for the development of mucocele
The inside of the paranasal sinuses is lined with mucous membrane. The glands of the mucous membrane produce a secretion, which is normally constantly evacuated from the sinus, cleansing it.
A mucocele develops when the outflow of secretions from the sinus is disrupted due to obstruction (blockage) of the excretory duct.
The causes of obstruction can be different:
- chronic inflammatory process in the nose or paranasal sinuses (rhinitis or sinusitis);
- severe curvature of the nasal septum due to facial trauma (for example, in the area of the nasal root) or surgical interventions in the nasal cavity and paranasal sinuses (surgical correction of the structures of the nasal cavity, sinus lift, surgery on the lacrimal ducts) [7];
- hypertrophic pathological processes in the zone of sinus anastomosis: polyp, tumor, hypertrophy of the middle turbinate;
- allergy.
An important role in the occurrence of this disease is played by the influence of external aggressive factors, such as: nickel, chromium, isopropyl alcohol, wood dust, various types of glue. The abuse of tobacco and alcohol is also of great importance, since this disrupts the self-cleaning mechanism of the nasal sinuses [14][15].
Prevalence
Mucocele is equally common in women and men, mainly between the ages of 10 and 45 years. In men, the disease most often manifests itself at 15–25 years of age [1]. This is due to the peculiarities of the development of the paranasal sinuses and the high incidence of injuries in men of active age.
The sinuses with narrow excretory canals are most often affected: the frontal sinuses (60–65%) and the sinuses of the ethmoidal labyrinth (20–25%). Less common are mucoceles of the maxillary (10%) and sphenoid sinuses (1–2%) [7][17][18].
Removal of retention cyst of the lower lip, local anesthesia
Make an appointment
Foot Alexander Anatolyevich Doctor of the highest category, maxillofacial, plastic surgeon, has the highest category. More than 27 years of experience.
Doctor of the highest category, maxillofacial, plastic surgeon, has the highest category. More than 27 years of experience. Graduated from Irkutsk State Medical Institute. Repeatedly completed specializations in maxillofacial and plastic surgery in Moscow, St. Petersburg, Chelyabinsk, Irkutsk. Has the highest category. Author of a number of articles in medical periodicals. From 2013 to the present time he has been working as a medical maxillofacial and plastic surgeon. He has extensive experience in performing reconstructive surgery operations: jaw resection with immediate replacement of the defect with autologous bone, osteoplastic surgeries, implantology, post-traumatic reconstructive surgeries and congenital pathologies (bite correction using intraoral access). The doctor performs operations of a high category of complexity; reconstructive operations; operations belonging to the category of high-tech operations, including circular lifting of the skin of the face and neck (including SMAS lifting), blepharoplasty, rhinoplasty, otoplasty, elimination of wrinkles on the forehead and nasolabial folds, liposuction, removal of benign formations of the maxillofacial area , as well as scar correction and dermabrasion. Certificates and diplomas in plastic surgery, maxillofacial surgery, dental surgery are valid until 2023.
View the embedded image gallery online at: https://www.medistar24.ru/chelyustno-litsevaya-khirurgiya/788-udalenie-retentsionnoj-kisty-nizhnej-guby-mestnaya-anesteziya-5-000-rublej#sigProId43fcb6fc79
A retention cyst of the lower lip is a benign formation formed from a minor salivary gland with a blocked duct. Such a cyst may form outside the gland, but the contents of the cyst will be the same, and its walls will consist of epithelial tissue. What can cause such a pathology and why is it dangerous? Small salivary glands are found in large numbers on the mucous membrane of the oral cavity, in particular on the inside of the lower lip. When biting your lip or as a result of another injury or inflammatory process, the gland duct can be blocked - temporarily or permanently. The saliva produced by the gland will accumulate, forming a cyst with liquid contents. Often, in addition to saliva, the cyst contains blood that has entered the cavity as a result of hemorrhage caused by injury. Temporary blockage occurs as a result of tissue swelling, and after 10-15 days the cyst caused by such blockage will resolve without a trace. If the duct is completely blocked (for example, during the epithelization of an injured area of the lip), such a cyst will increase in size, and at first it will simply interfere during conversation and eating. As it increases, it will begin to create aesthetic discomfort; the contents of the cyst may begin to decompose, causing suppuration, which may result in pain and additional swelling. In some cases, such cysts periodically break through, their contents flow out, but when the site of the break becomes overgrown, the liquid begins to accumulate again, and the process becomes chronic, threatening not only the expansion of the inflammation zone, but also infection with further complications. If the cyst does not break through, it can increasingly increase in size, as a result of which it is increasingly injured; inside it, the process of tissue degeneration into malignant can begin. The risk of malignant degeneration of the cyst is especially high in people who smoke or have a hereditary predisposition to cancer. Therefore, if during the first 15 days after the initial injury the newly formed cyst has not resolved, doctors most often recommend removing it surgically to avoid further complications. It is extremely important to find a competent and experienced doctor who, at any stage of development of the pathology, will determine the degree of danger of the cyst and carry out treatment in the safest and most effective way.
After an initial survey and examination, the doctor may prescribe the patient an ultrasound and probing of the salivary gland canals, as well as puncture of the cyst to obtain a sample of its contents and conduct a histological examination. Sialography may also be prescribed to obtain information about the condition of the salivary glands, the stage of development of the cyst (also called mucocele) and to identify or exclude an oncological process. If, as a result of research, a malignant component of the formation is excluded, the doctor proceeds to prepare for its removal. As with any other surgical procedure, the patient must refrain from drinking alcohol before removing a cyst; If the patient is taking any medications that reduce blood clotting, it is necessary to consult with the doctor who prescribed them regarding the advisability of temporarily discontinuing them. The procedure itself is not very painful, so it is performed under local anesthesia. The doctor can use either a regular scalpel or a laser, radio frequency or ultrasound method of performing surgical procedures. The doctor decides which removal method to choose based on the condition of the cyst, its location, inaccessibility and other information. After the anesthesia begins to take effect, the doctor pulls back the lip, allowing the most convenient access to the cyst. Since it is extremely difficult to fix the lip in a comfortable position, as a rule, the doctor’s assistant holds the lip while performing all manipulations. Next, the doctor makes several incisions along the edges of the formation so that the cyst shell can be completely separated from healthy tissue. Then the doctor completely removes the contents, washes the resulting wound and applies stitches.
After the operation is completed, the doctor gives the patient the necessary recommendations regarding wound care. If the sutures are not made of self-absorbable threads, the patient will need to return after the time specified by the doctor to have the sutures removed. You need to understand that the lips - and their inner part too - are an area with a large number of nerve endings. Therefore, after the anesthesia wears off, after the operation is completed, at first the patient may experience discomfort in the operated area. This is natural, and if the patient conscientiously follows medical instructions regarding the care of the wound and oral cavity during the rehabilitation period, he will soon be able to forget about the cyst and completely return to a full, healthy life.
In the multidisciplinary clinic “Medistar”, only highly qualified specialists, experienced and qualified professionals in their field practice medicine, who have performed a huge number of successfully performed operations of varying degrees of complexity. Modern technical equipment and our own laboratory allow you to go the entire way - from diagnosis to complete treatment - within our medical center, without leaving it in search of any procedures or diagnostic methods.