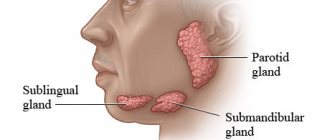
Salivary stone disease is a disease that affects both men and women equally. Moreover, the age range for salivary stone disease is very wide: cases of salivary stone disease occur both in childhood and in middle and old age. In general, the entire pathology of salivary stone disease occurs in 20.5% - 60.1% of cases with a predominant lesion of the submandibular salivary gland. In this article we will look at the clinical picture, diagnosis and treatment of salivary stone disease.
The submandibular salivary gland often suffers from salivary stone disease due to:
- Saliva flow against gravity;
- Long and winding channel;
- Contains two types of terminal sections: protein (predominant) and mucous.
In general, salivary stone disease is manifested by the appearance of stones of various sizes and shapes, both in the gland itself, but most often in its duct. The process of stone formation is long and may be asymptomatic.
Etiology of salivary stone disease
No matter how trite the phrase may sound: “The etiology of salivary stone disease is not fully known,” but it is true. The fact is that in some patients, factors that seem to play an important role in the occurrence of salivary stone disease do not lead to the development of pathology at all. And the opposite: patients who do not have the supposed etiological factors come with a huge stone in the duct of the salivary gland. But still, among the factors that may play a role in the etiology of sialolithiasis, there are:
- Increased saliva viscosity;
- Change in acid-base balance -> alkalization;
- Narrowing of the duct;
- Inflammation of the duct;
- Entry of foreign bodies into the duct;
- Disruption of metabolic processes in the body when calcium levels are higher than normal;
- Genetic predisposition;
- Incorrectly developed gland and its duct during anthogenesis;
- Hypovitaminosis/vitaminosis group A;
- Chronic diseases of the salivary gland.
Pathogenesis of salivary stone disease
The pathogenesis of salivary stone disease is a rather difficult process to understand and study. The difficulty in studying salivary stone disease is determining the triggering moment and factor in the occurrence of salivary stone, because patients arrive at later clinical stages.
But if we talk about the chemical composition of the salivary gland stone, then these stones are complex in their structure, consisting of both organic and mineral substances. Moreover, the mineral component is predominant at 60 - 70%. Representatives of the mineral component in salivary gland stones are phosphates, calcium, calcium-based salts, and brushite. The organic component is bacteria, the lining of the ducts and the organic composition of saliva. Of course, salivary gland calculi grow gradually, which reveals their layered structure. There are differences in the composition of salivary gland stones. Thus, the parotid salivary gland is characterized by a predominance of the organic component over the mineral one, which is the opposite for the submandibular salivary gland.
There are several theories about the pathogenesis of salivary stone disease. Some authors believe that the pathogenesis of salivary stone disease is based on a violation or instability of the state of the components that participate in the formation of the stone, which leads to their coagulation and crystallization. The point is that a core is formed from an organic component. Then the process of mineralization begins around this core, that is, the mantle is formed. These processes occur due to adsorption, and initially have the consistency of jelly. Subsequently, due to calcium, phosphate ions and their salts, the stone becomes dense.
There is another opinion. The basis of stone formation is the core, which is always an organic component. And most often, the trigger point in the occurrence of minerals and their adsorption is inflammatory diseases in the salivary gland, a change in the rate of salivation, saliva viscosity or pH.
An interesting fact: in the saliva of mammals (I mean animals) and humans, microconcretions were found in the healthy salivary gland that did not in any way affect the functioning of the salivary gland. Consequently, the occurrence of a stone in the salivary gland will not always be a pathological process.
The process of stone formation is long. And there is no direct relationship between the size of the stone and the duration of its formation. However, stones can be either smooth or rough. There are grooves or channels on the surface of the stones. They are very variable in form. Thus, there are stones of oval, round, ovoid, elongated, and oblong shapes. There is a difference in the density of stones depending on their location. So the stones that are located in the gland itself will have a denser consistency. Most often, such stones are round in shape.
Complications and relapses
Even if the treatment is successful and the examination results show no signs of the presence of cancer cells in the patient’s body, a relapse may occur in the future. Therefore, you need to regularly see an oncologist, come for examinations, undergo various studies and take tests.
Typically, the doctor prescribes examinations once every few months for several years, then less frequently.
- If cancer recurs, treatment options may vary:
- If the tumor can be removed, surgery is performed followed by a course of radiation therapy.
- If the tumor cannot be removed surgically, the doctor prescribes radiation therapy in combination with chemotherapy.
- If there are distant metastases, chemotherapy becomes the main treatment method. Radiation therapy and surgery can be used to control some symptoms.
With advanced cancer with metastases, achieving remission becomes extremely unlikely. In this case, treatment will be aimed at slowing the progression of cancer, combating symptoms, and prolonging the patient’s life.
Euroonco doctors undertake cancer treatment at any stage. For us there are no hopeless patients. You can always help, and we know how to do it correctly, we have all the necessary technologies, the latest generation drugs.
Clinical picture of salivary stone disease
The clinical picture of salivary stone disease consists of three main stages:
- The initial stage of salivary stone disease;
- Clinically pronounced stage of salivary stone disease;
- Late stage of salivary stone disease.
The initial stage of salivary stone disease is characterized by the complete absence of any acute clinical signs. Here the changes occur at the histological level (and those who remember histology will now understand what I mean):
- Dilation and congestion of blood vessels;
- Swelling and loosening of connective tissue;
- Formation of lymphocytic infiltrates;
- Preservation of acini;
- Expansion of intralobular, interlobular ducts;
- Enlargement and compaction of collagen fibers.
One of the very first and main clinical signs of the initial stage of salivary stone disease is a change in the rate of salivation, especially when eating food or at the sight of food. Patients experience so-called “salivary colic.” Salivary colic with salivary stone disease is a common occurrence. Characterized by enlargement of the salivary gland; patients say: “It’s as if something is bursting,” pain occurs. The pain interval can be short: from a few seconds, but with the progression of salivary stone disease it increases to several hours.
If you palpate the salivary gland, the doctor notes its softness and painlessness, the secretion is released normally. When palpating the duct of the submandibular salivary gland, a dense calculus can be detected. When examining the oral cavity, no changes in the mucous membrane are noted.
The clinically expressed stage of salivary stone disease is a progression of the initial stage. The name of the stage speaks for itself: at this stage of the development of salivary stone disease, there is pronounced inflammation of the salivary gland. Symptoms are similar to acute sialadenitis:
- Acute onset: increased body temperature to 38.5 degrees, general malaise, weakness, headache;
- Facial asymmetry due to swelling of soft tissues in the area of the salivary gland;
- Edema;
- Difficulty eating;
- Painful palpation of the salivary gland;
- When examined from the oral cavity, hyperemia of the mucous membrane is noted on the corresponding side;
- Upon palpation, a stone is identified.
In the absence of treatment, with each exacerbation the disease reaches the late clinical stage of salivary stone disease. This may also be preceded by a purulent-necrotic form of salivary stone disease.
The late stage of salivary stone disease is characterized by complete atrophy of the salivary gland acini with replacement of the parenchyma by connective tissue.
The clinic of sialolithiasis at a late stage is characterized by:
- Constant aching pain in the gland area;
- Rare “salivary colic”;
- Swelling of soft tissues;
- Eating is difficult or impossible;
- The general condition is disturbed;
- Facial asymmetry due to edema, but only within the gland;
- On palpation – painlessness;
- When massaging the gland -> mucous-purulent discharge from the duct.
- The mouth of the duct is widened.
Prognosis of salivary gland tumors
If a patient has been diagnosed with a benign tumor of the salivary gland, and timely and high-quality surgical treatment has been performed, then the recovery process, although long, has a positive trend. Such diseases recur in one third of cases.
When treating tumors of the salivary glands of a malignant type, the prognosis for recovery is unfavorable. Recovery occurs in only 25% of all cases of the disease, and complications are noticed in half of the cases. The same applies to situations with the appearance of additional lesions, which are observed in 50% of patients.
Diagnosis of salivary stone disease
Diagnosis of sialolithiasis consists primarily of a thorough collection of complaints, life history and illness. This is followed by an examination, both external and intraoral. For qualitative diagnosis of stones in the ducts of the salivary glands, the technique of bimanual palpation is used. To do this, the fingers of one hand are placed on the mucous membrane in the projection of the gland and its duct, the fingers of the other hand are placed on the side of the skin.
After bimanual palpation, it is recommended to massage the gland, which will determine the consistency of the secretion and the rate of its release. Probing the duct in case of salivary stone disease is not recommended at the time of exacerbation, as this can lead to perforation of the duct wall. And so probing with the help of special probes is allowed. Using probes, you can determine the fistula tracts if there was a perforation of the stone.
For a high-quality diagnosis of salivary stone disease, you need to understand two points: when the stone is localized in the salivary gland, there are no clinical symptoms. Such stones are discovered purely by chance. But when a stone moves either from a gland into a duct or along a duct, the clinical picture is entirely variable.
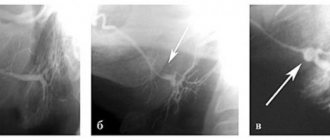
The main methods for diagnosing salivary stone disease are radiation methods. Due to the mineral component in salivary stones, these stones are X-ray positive.
Radiation methods that can be used:
- Survey radiography. Survey radiography can be of the floor of the mouth, which is recommended for examining the anterior and middle sections of the excretory duct of the submandibular salivary gland, or it can be in a lateral projection to determine the calculus either in the submandibular salivary gland itself or in its initial section.
- Contrast sialography, which has not lost its importance both for the diagnosis of salivary stone disease and for other diseases of the salivary glands. Verografin, urografin, and cardiotrast are used as contrast agents. All substances are water-based and do not have a pathological effect on glandular tissue.
- Digital subtraction sialography. This diagnostic method is good because there is no overlap of images of the salivary glands and the skull. This occurs due to the fact that before the contrast agent is introduced, the study area is recorded in the computer memory, which is then subtracted from the image with the contrast agent injected.
- Cone beam computed tomography;
- Ultrasound examination of the salivary gland can be carried out both from the skin and from the oral mucosa. Due to the different ability of tissues to display sound, it is possible to determine X-ray negative stones, their location and size.
- In order to determine structural and functional changes in the salivary glands, radionuclide studies and magnetic resonance computed tomography can be carried out.
- Fiberendoscopy of the salivary glands is based on the use of ultra-thin fiber optics, which are inserted into the main duct of the salivary gland. It is the newest method in the study of the salivary glands.