A salivary gland tumor can be diagnosed using ultrasound, salivary gland biopsy, sialography or sialoscintigraphy. For example, a biopsy of the salivary glands is usually combined with a morphological or cytological study.
Treatment of this disease is usually surgical, but can also be combined.
Interestingly, tumors can originate from both minor and major salivary glands, and can also affect them secondarily. If we talk about the percentage, then this type of tumor accounts for only 1.5% of all. Such tumors can arise and form at any age, but most often the disease affects people in the age group from 40 to 60 years, most often men.
A characteristic feature of salivary gland tumors may be their tendency to malignancy and local recurrence, not to mention metastasis.
Functions of the salivary glands
There are many functions that the salivary glands perform, but some of them deserve special attention. After all, having understood these processes, it is easier to understand how pathologies are formed and how to deal with them, how to treat them. The first and, perhaps, the main one is exocrine, that is, the production of enzymes involved in the digestion process. They enter the oral cavity through the ducts of the glands that open under the tongue, throughout the mucous membrane or above the upper molars. Salivary mucin moistens the food bolus, takes part in its formation and promotion, and ensures the initial digestion of carbohydrates. Enzymes are known to enhance the flavor of food. And saliva itself protects teeth from various damages. The second, no less important, is protective. Saliva contains antiseptic components, the same mucin, immunoglobulins, which provides local immunity. But this is not the only important thing. Saliva plays an unparalleled role in protecting the oral organs as well as preventing tooth decay. The fact is that it is it that saturates the enamel with minerals, maintains the processes of de- (exit) and remineralization (saturation) in harmony and balance. The salivary glands also ensure the removal of metabolic products and the filtration of blood plasma components from the capillaries of the oral cavity into saliva.
Pathological anatomy
Dystrophic changes in the salivary glands are often combined with a violation of their functions. Protein dystrophies (see Protein dystrophy) are characterized by cloudy swelling of glandular cells (granular dystrophy) and hyalinosis of interstitial tissue (see Hyalinosis). Granular degeneration of glandular cells is observed with sialadenitis (see), cachexia (see), as well as with poisoning with salts of heavy metals (mercury, lead, etc.), released with saliva and damaging glandular cells. Hyalinosis of the interstitial tissue leads to thickening of the interlobular septa; hyaline can be found in the walls of small vessels and in the basement membranes of the terminal (secretory) sections of the veins. With general amyloidosis (see), amyloid is occasionally deposited in the walls of blood vessels and basement membranes. Fatty degeneration of glandular cells (see Fatty degeneration) is observed in infectious diseases (diphtheria, tuberculosis) and chronic cardiovascular diseases. Lipomatosis S. is expressed in the growth between their lobules of adipose tissue (see Lipomatosis). Excessive development of adipose tissue in the thickness of the stomach. occurs in general obesity (see) and senile atrophy of the stomach.
Carbohydrate dystrophies (see) are observed in diabetes mellitus and are characterized by the appearance of inclusions of glycogen (see) in the cytoplasm of glandular cells.
Necrosis S. g. is rare and occurs. arr. with purulent denitis.
Disorders of blood and lymph circulation in the stomach. have no independent significance in the overall pathological picture. They are only local manifestations of general circulatory disorders, occurring in the form of venous hyperemia (see). Arterial hyperemia is observed, as a rule, during local inflammatory processes in the stomach. and in case of disruption of innervation. Hemorrhages in the S. g. are noted in blood diseases, injuries and certain inf. diseases (eg, typhoid and typhus).
An acute nonspecific inflammatory process in the gland—adenitis—occurs as a result of the introduction of pathogens of a viral or bacterial infection that penetrate the gland through the excretory duct, as well as by hematogenous or lymphogenous routes. There is a diffuse form of inflammation of the stomach. and limited (in the form of an abscess). Chronic nonspecific sleeping adenitis can occur primarily and less frequently, as an outcome of acute inflammation of the stomach. With chronic inflammation of the stomach decrease in size and acquire a dense consistency. Microscopically, infiltration of the stroma and parenchyma of the glands with lymphoid elements, atrophy of the terminal (secretory) sections and pronounced stromal sclerosis are noted.
Defeat S. zh. in tuberculosis it manifests itself in the form of a unilateral lesion and occurs secondarily as a result of lympho- and hematogenous dissemination. Development of tuberculosis S. begins with damage to regional lymph nodes of the gland, subsequently its parenchyma and stroma are involved in the process. In S. zh. detect miliary tubercles or small nodules undergoing caseous necrosis. Sometimes there is melting of caseous masses with the formation of a tuberculous abscess, which can cause fistulous tracts. With histol. The study reveals tuberculous tubercles of a normal structure (see Tuberculosis), and when the tissue melts, nonspecific inflammatory changes occur.
Defeat S. zh. It is rare in syphilis. Inflammatory changes are detected only in the secondary and tertiary periods of the disease and can be diffuse or limited in nature. With diffuse inflammatory infiltration (most often in the secondary period) S. It is affected throughout, and abscess formation and necrosis of individual areas of the gland often develop. Limited forms of damage are characterized by sclerosis and atrophy of the stomach. Histologically in the S. g. detect changes corresponding to the picture of specific inflammation in syphilis (see).
Actinomycosis of the salivary glands can develop primarily, as a result of the penetration of actinomycetes into the gland along the ducts, or secondarily, when the inflammatory process spreads from the surrounding salivary glands. soft tissues. Primary actinomycosis (see) proceeds slowly, with periodic exacerbations. In S. zh. a dense, limited infiltrate is revealed, which subsequently spreads to the entire gland with the formation of multiple abscesses. Secondary actinomycosis has less clear symptoms due to the development of a diffuse inflammatory process in the surrounding tissues. Specific inflammatory changes in actinomycosis of S. characterized by the development of granulation tissue with small pustules and pronounced signs of scarring. Druses of actinomycetes are often found in the inflammatory infiltrate, which, when localized in the excretory ducts, can be the basis for the formation of salivary stones.
Of the parasitic diseases of S. zh. Cases of echinococcosis are extremely rare. At the same time, S. are affected secondarily, and macro- and microscopic changes in them are similar to those with damage to other organs (see Echinococcosis).
Hypertrophy of the stomach. is a response to patol. processes occurring in the body. Increase in s. observed in endocrine diseases (eg, diffuse toxic goiter, hypothyroidism), cirrhosis of the liver and usually occurs as a result of reactive proliferation of interstitial tissue, which leads to interstitial sialadenitis. Hypertrophy of interstitial tissue is also observed in Mikulicz syndrome (see Mikulicz syndrome). In physiol. conditions of hypertrophy of the stomach. observed during pregnancy and the postpartum period. Sometimes, after removal of one of the paired glands, vicarious hypertrophy develops on the opposite side.
Atrophy of the s. characterized by a decrease in their size. Atrophic changes are observed when there is a violation of the innervation of the gland, age-related involution, as well as when the outflow of gland secretions is difficult, followed by atrophy of the parenchyma. Histologically, there is a proliferation of connective tissue with thickening of the interlobular septa, a decrease in the size of glandulocytes, and emphasized lobulation of the sternum.
Postmortem changes in S. zh. occur early (after 3-4 hours), which is associated with the self-digesting effect of salivary enzymes. Macroscopically, the glands acquire a reddish tint and soften. With pathohistol. The study reveals destructive changes in glandular cells, while interstitial tissue retains its structure much longer.
Examination methods include, in addition to general methods (questioning, examination, palpation, etc.), such special methods as probing the ducts, sialometry (see Salivation), cytol. examination of secretions, ultrasonic dowsing (see Ultrasound diagnostics), thermovisiography (see Thermography), scanning (see), sialography (see), pantomography (see), pneumosubmandibulography (see), computer tomography (see).
Classification of salivary glands
There are quite a lot of salivary glands located in the oral cavity, which can be divided into small and large - only 3 pairs of large salivary glands. There is a classification based on the nature of the secreted secret:
- protein;
- mucous membranes;
- mixed.
The minor salivary glands secrete mucous and mixed secretions and are located in the submucosal layer of the lips, cheeks, palate and tongue. Unlike the small ones, the large salivary glands are paired organs that play an important role in the digestion process, as well as protecting the oral cavity. The parotid gland is located in the retromandibular fossa, and its anterior section lies on the masticatory muscles. This is the largest gland, which is divided into segments and lobules by special bridges. Arteries, veins and nerves pass through these glands; they secrete saliva with a high concentration of protein.
Submandibular
The gland is smaller, and its ducts exit into the anterior section
of the sublingual
region. These are complex, branched glands that are located under the lower jaw. At rest, this gland secretes up to 70% of all saliva. The sublingual glands are the smallest among the large salivary glands. These are mixed glands that secrete protein, mucous and protein-mucus secretions. The size can explain the low productivity of the gland - only 4% of the total volume of saliva.
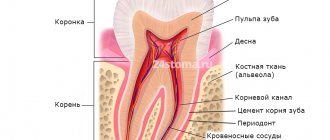
The structure of the salivary glands
In the structure of the salivary glands, stroma and parenchyma, the secretory section and excretory ducts can be distinguished. Parenchyma is a dense connective tissue capsule that gives rise to interlobular septa. The parenchyma consists of the terminal sections of the gland and small excretory ducts, which are then transformed into large ones and exit into cavity
at different levels, it all depends on the identity of the gland. The ducts consist of cells that have contractility, this promotes the release of secretions from the gland and its ducts.
Saliva and its functions
Each gland produces fluid, mixing in the oral cavity, mixed saliva is formed. Its functions are varied:
- digestive;
- protective, due to participation in the maintenance of local immunity, as well as the normal activity of the mucous membrane;
- antiseptic;
- communicative, that is, it takes an active part in the formation of speech;
- metabolic, ensures the maintenance of de- and remineralization processes in teeth, etc.
Saliva
- this is a viscous liquid with a variable composition, it all depends on the rate of its secretion. However, 99% of its composition is water. The rest is mineral and organic substances: chlorides, phosphates, bicarbonates, sulfates, as well as sodium, potassium, calcium, magnesium. These minerals take an active part in the formation of enamel and maintaining dental health. All these substances are found in the form of simple ions, as well as in the composition of salts, proteins and chelates. The organic component of saliva is represented by proteins, immunoglobulins, acids, and even cholesterol is found in it.
How is saliva formed?
Salivation is the secretion and release of saliva. This is an intracellular process that occurs in the glands. Periodic changes for the purpose of saliva production are called the secretory cycle, in which several successive stages or phases can be distinguished:
- Low-molecular substances that participate in the formation of enzyme synthesis are released from the blood into the secretory cell;
- synthesis of salivary secretion occurs in cellular structures and passes into the Golgi apparatus;
- secretion ripening;
- preserving the secretion in special granules, and they are stored there until a signal is received that saliva is needed. The nervous system regulates this process;
- if a signal has been received, salivation occurs, and this is a calcium-dependent process.
Inflammation of the salivary glands and other diseases
Treatment of diseases of the salivary glands directly depends on the cause of the reaction and the underlying disease.
Inflammation can be viral, bacterial, or fungal in nature, but more often it is a traumatic injury. Given the close proximity of teeth, pathologies of the dental system can also cause the development of pathologies. But systemic diseases cannot be ruled out, for example, some autoimmune diseases that affect the functioning of the immune system and predispose to infections. But whatever the cause of inflammation of the salivary glands, treatment should begin as soon as possible. There is a high probability that chronic inflammation will cause decreased saliva production and, as a result, oral diseases, digestive disorders, and even the likelihood of developing cancer. Text: Yulia Lapushkina.
Topography, anatomy
Depending on the location and place of confluence of the excretory ducts, the salivary glands are divided into glands of the vestibule of the oral cavity and glands of the oral cavity itself. The first group includes the molar (gll. molares), buccal (gll. buccales) and labial (gll. labiales) glands, as well as the parotid gland (see), the excretory duct opens into the vestibule of the oral cavity on the mucous membrane of the cheek on level of the upper second molar. The submandibular and sublingual glands, as well as the glands of the tongue (gll. linguales), hard and soft palate (gll. palatinae) belong to the glands of the oral cavity itself.
Large S. They are lobular formations that can be easily palpated from the oral mucosa (see Parotid gland, Submandibular gland, Sublingual gland).
Malye S. zh. have a diameter of 1 - 5 mm and are located in groups in the submucosa of the mouth (see Mouth, oral cavity). The largest number of small S. zh. located in the submucosa of the lips, hard and soft palate. Among the minor salivary glands of the tongue there are: Ebner's glands - branched tubular glands, the ducts of which open into the grooves of the circumvallate papillae and between the leaf-shaped papillae of the tongue; glands, the ducts of which open into the crypts of the lingual tonsil, as well as the anterior lingual gland (gl. lingualis ant.), which is a cluster of glands that open with 3-4 excretory ducts on the lower surface of the tongue and under it (nunova glands).
Research methods
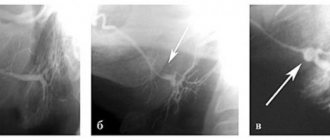
Rice.
1. Pantomosialogram of unchanged submandibular glands: 1 - parenchyma of the gland, 2 - ducts of the gland, 3 - submandibular duct (the contours of the ducts are smooth, clear). To determine the nature of the pathological process, probing of the ducts, sialometry (measurement of the amount of secretion released from the duct per unit of time), cytological examination of the secretion (see Saliva), radiography, pantomography (see) with artificial contrast of the ducts, or pantomosialography (Fig. 1) are used ), thermal imaging (see Thermography), ultrasonic dowsing (see Ultrasound diagnostics) and scanning (see).
Summary
Ultrasonography has established itself as the primary imaging technique in the diagnosis of salivary gland diseases. Sonographic examination is usually sufficient to diagnose sialolithiasis. If chronic sialoadenitis or sialoadenosis is suspected, and sonographic data are insufficient, standard sialography may be required in some cases. A histological examination is necessary as soon as the diagnosis of a neoplasm is established. If the tumor's enlargement and connection with surrounding tissues cannot be determined sonographically, subsequent computed tomography or magnetic resonance imaging should be performed. To conduct research, we recommend using a device from GE Voluson E8 .
Symptoms of the disease
The main symptoms of sialadenitis include the following:
- pain while chewing;
- redness, swelling of the cheeks, neck;
- violation of taste perception;
- unpleasant taste in the mouth;
- dry mucous membranes;
- general deterioration of health;
- difficulty opening the mouth.
In acute sialadenitis, symptoms increase quickly and can also subside quickly. However, in the absence of proper treatment, the disease can become chronic, so even if you feel better, it is important to consult a dentist.
Lack of therapy can cause complications, the most common of which include the formation of ulcers (abscesses), secondary infection - the addition of a bacterial infection to a fungal infection, etc. This will require more serious intervention and long-term treatment, so you should not postpone a visit to the doctor.