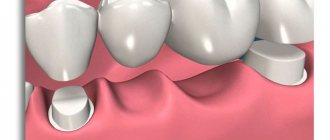
Let's continue our conversation about the structure of other periodontal tissues. Let's first remember what they are. Periodontal tissues - periodontal structure (highlighted in red in the figure):
- gum;
- periodontal ligament;
- tooth root cement;
- alveolar bone.
It is important that the gums and other periodontal tissues have different functions. The main role of the gums is protection. Protection of underlying tissues from external influences. Cementum, alveolar bone and periodontal ligament together form the so-called “supporting apparatus of the tooth.” Thanks to these tissues, the main function of the periodontium is performed - to hold the tooth in its rightful place, in the socket.
Disturbance = inflammation
Any disruption of the periodontal ligament and restoration is likely to cause inflammation. Any inflammation in this area can negatively affect the result of the entire work. Understanding the function and location of the ligament increases the likelihood of successful restoration. In particular, factors such as
- position of the gum edge,
- marginal fit,
- contact areas,
- prosthesis shape,
- Iatrogenic damage.
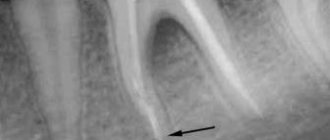
How does pathological resorption and resorption of roots with intact periodontium proceed?
If intact periodontium is in contact with the root, the process usually involves osteoclasts and, at later stages, pulp tissue. They promote more intensive resorption of dentin from the side of the tooth cavity.
If there is chronic inflammation in the periodontium, the cells of the inflammatory infiltrate are involved in the resorption process. Instead of connective tissue, granulation tissue is formed. As a result of resorption, small and medium-depth lacunae filled with granulations are formed. With a pathological course, resorption of not yet fully formed roots is possible. It also spreads to the rudiments of permanent teeth, accelerates the resorption of parts of the follicle and initiates the premature eruption of molars.
Impaired passive eruption
When planning restorations, if the volume/height of the gingival tissue is large, it is necessary to remember the phenomenon of altered passive eruption. Such a violation leads to changes in the connection of the periodontium and restoration, which should be taken into account.
Passive eruption involves displacement of the gingival margin in the apical direction, gradual exposure of the crown and securing the edge in the area of the tooth neck. Violation of this process leads to an expansion of the zone of fixation of the gingival margin, that is, it can “stop” away from the CEJ. According to a study by Garber and Salama (1996), impaired passive eruption occurs in 7-14% of the population, predominantly in patients with thick and flat gingival tissue biotypes.
In 1977, Coslet et al proposed the following classification of passive eruption disorders:
- type 1A – wider band of keratinized tissue, normal bone ridge level;
- type 1B – a wider band of keratinized tissue, a bone ridge at the level of the CEJ;
- type 2A – less wide band of keratinized tissue, normal bone crest level;
- type 2B – a less wide band of keratinized tissue, a bone ridge at the level of the CEJ.
Treatment options depend on the type of passive eruption disorder:
- type 1A – gingivectomy, displacement of the flap in the apical direction;
- type 1B – gingivectomy, bone grafting, flap displacement in the apical direction;
- type 2A – displacement of the flap in the direction of the apex;
- type 2B – bone grafting, displacement of the flap in the apical direction.
If passive eruption disorder remains undiagnosed and is not taken into account when drawing up a treatment plan, the complications mentioned above are possible, that is, periodontal inflammation around the restoration (thick biotype) or gingival recession (thin biotype).
Periodontal cells
Periodontal cells are
- connective tissue cells;
- epithelial islets of Malasse;
- protective cells (neutrophils, lymphocytes, macrophages, eosinophils, mast cells);
- cellular elements of nerves and blood vessels.
Connective tissue cells are mainly fibroblasts that synthesize collagen. They are also capable, if necessary, of protective reactions - phagocytosis, hydrolysis.
Closer to the bone, osteoblasts and osteoclasts, cementoclasts, -blasts, and odontoclasts are found near the tooth.
Epithelial islands of Malasse are remnants of epithelium walled up next to cement, which was destroyed during tooth eruption. In general, their role has not yet been studied. It is only known that with age they can either disappear without a trace or turn into cementicles or cysts.
The ground substance fills the space between cells and fibers. Its main difference from the intercellular substance of the adjacent connective tissue of the gums is the possible presence of cementicles. They can be attached to the tooth (1) or freely in a ligament (2):
We already know that they can be formed from the epithelial islands of Malasse. But there are other sources of their development, for example:
- particles of cement or bone;
- Sharpey fibers;
- calcified blood vessels.
The periodontal ligament is a key component of the periodontium. It is she who is responsible for most of its functions. We'll talk about functions a little later, but for now let's move on.
Coronal lengthening
Lengthening the coronal part is a procedure that can minimize the risk of violation of the biological width. When considering the applicability of this procedure to a specific case, one should calculate the feasibility of its implementation in general. Preparation for surgery should include determining the biotype of gingival tissue, assessing its condition, and high-quality x-rays. In some cases, such as severe abrasion/wear of teeth, a sensitivity test should also be performed. A wax up, a wax-up model, is often helpful in discussing the treatment plan with the patient.
Tooth cement
Cement covers the outside of the tooth root. It consists of
- collagen fibers and
- calcified intercellular substance.
- (+ cells).
(there are no vessels in cement)
External fibers are isolated - Sharpey's, from the periodontal ligament. And internal ones, which are directly formed in the cement by cementoblasts, as well as the intercellular substance.
Cells are not present everywhere in the cement. Where there is, there is cellular cement (CC). Where not - acellular (BC).
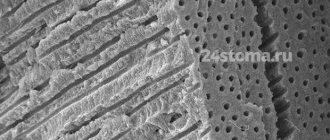
Acellular cementum
Acellular cementum is also called primary cementum. It is formed before the cellular one and until the moment the tooth reaches its antagonist, it does not become occluded. It covers the root up to half (in the direction from the crown to the apex). In the figure, AC is an acellular cementum that lies between dentin (D) and periodontal ligament (PL). You can notice that it is “striped”. These stripes, like rings on a cut tree trunk, indicate periods of cement formation:
Cell cement
Cellular cementum forms after the tooth reaches the occlusal plane. It is found in the apical third of the root and in the bifurcation area. Cell cement is less mineralized and contains fewer Sharpey fibers. In it (SS) separate spaces (lacunae) with cementocytes inside are found. Cementocytes are connected to each other through special tubules. Note the accumulation of cells in the ligament (PL). These are nothing more than cementoblasts:
It is noticeable from the figures that the width of the cement is greater towards the apical part of the root (approximately from 0.1 to 1 mm). An interesting age pattern: a 70-year-old has cement three times wider than an 11-year-old child.
Cement binds to enamel in different ways:
- there is a gap between them (sensitivity may bother you);
- butt connected;
- covers the enamel.
By the way, since we are talking about enamel, cement is much less mineralized in comparison with it. Cement is, in principle, the “softest” among the hard tissues of the dental system: it contains only about 50% hydroxyapatite. The figure is small compared to bone (65%), dentin (70%) and enamel (97%).
Speaking of bones.
Biotype of gingival tissue
When lengthening the coronal part, it is important to take into account the biotype of the gum. According to research results, the gingival margin can “grow” along the crown from the level determined during the procedure. This growth is more often observed in patients with a thick biotype of gingival tissue, but there are also individual characteristics. In addition, it is likely that the amount of gingival retraction depends on the position of the flap relative to the alveolar ridge at suturing, as described by Deas (2004). Therefore, if the patient has gum tissue of a thick biotype, it is possible to compensate in advance for the mentioned reverse movement of the edge during the formation of the gum during the operation. A temporary crown should be placed 6-8 weeks after surgery to ensure proper gum formation before the permanent crown is placed.
Periodontal fibers
The bulk of periodontal fibers consists of type I collagen. It is synthesized in fibroblasts. Next, tropocollagen molecules are formed, which form microfibrils, then fibrils, threads and bundles:
This structure of collagen fibers allows them to be both strong and flexible. In longitudinal section they have a wavy shape:
As with gingival fibers, many classifications of periodontal fibers have been proposed. According to one, there are 6 groups of periodontal fibers:
- transseptal;
- alveolar ridge fibers;
- horizontal;
- oblique;
- apical;
- intraradicular (interradicular).
The term “Sharpey fibers” is also often found in the literature, but this is not another group. These are the terminal, partially or completely calcified parts of periodontal fibers of all 6 groups, which intertwine and perforate the cement and alveolar bone. Plus, Sharpey's fibers are associated with non-collagenous proteins (osteopontin, bone sialoprotein) in bone and cement (red arrow in the figure), which ensures such a strong connection.
Transseptal fibers
Transseptal fibers (F) pass over the alveolar ridge (A) and connect two adjacent teeth (T). They are often classified as gingival fibers because they are not woven into the bone.
Alveolar ridge fibers
They originate in the area of cementum of the tooth root immediately below the attachment epithelium, go in an oblique direction and attach to the alveolar ridge or periosteum.
Horizontal, oblique and apical fibers also extend from the cementum to the bone. The only difference is in the angle at which they are directed and in which part of the periodontal ligament they are located. Horizontal ones are located at right angles closer to the edge of the tooth socket, apical ones in the area of the root apex. There are more oblique fibers between them. They are the ones who take on the vertical load that occurs during chewing and “transfer” it to the bone.
Interradicular fibers (as the name suggests) pass between the roots of a multi-rooted tooth (from the furcation) to the bone.
In addition to the main groups, the periodontal ligament also contains other, less ordered collagen and elastic fibers. Elastic fibers are mainly located parallel to the tooth in the cervical third of the root. They regulate blood flow in the vessels of the ligament.
Periodontal fibers are constantly renewed due to the work of periodontal cellular elements.
Gum enlargement after orthodontics
After orthodontic treatment aimed at lengthening the coronal part, enlargement of the gums is often observed, i.e. its edge rises above the desired level. In such cases, you should not immediately take up a scalpel and surgically remodel the gum. The gums will return to the desired shape on their own within 3-6 months after treatment. At these marks it is already possible to assess its condition and decide on the need for surgical correction of the edge.
In the “Orthopedics” department of the Stommarket.ru online store you will find a variety of materials necessary for successful restorations of various levels of complexity:
https://stommarket.ru/catalog/ortopediya/
Nice prices and excellent delivery conditions!