Select a city to find an ENT doctor
A lump in the throat is a dense formation that can appear on the back of the throat, tonsils, neck, or under the chin. Its appearance is accompanied by discomfort and indicates the development of various diseases.
The symptoms and location of the tumor depend on the causes of the pathology. When the first signs of illness appear, you should consult a specialist. He will prescribe a course of effective treatment, taking into account provoking factors and the individual characteristics of the patient.
Reasons for appearance
There are many reasons for the appearance of a lump, most of them are not life-threatening, but still you should not put off visiting a doctor.
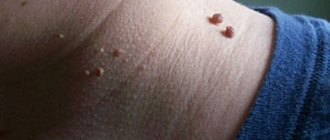
- Cyst. This benign formation practically does not hurt, is small in size, about the size of a pea, and does not differ in rigidity when pressed from other parts of the body. While palpating, the ball rolls under the skin and even disappears, but then appears again. However, the cyst is dangerous because the lump often contains lymph, pus, or other fluid. The reason for the appearance of a cyst is an infection under the skin with further blockage of the sebaceous glands.
- A lipoma is a soft lump under the skin on the neck. Its development occurs painlessly, and during palpation does not cause discomfort. Remove if the hard ball under the skin hurts when pressed or is very itchy. If there are no symptoms, the lump may not be cut out.
- Folliculitis is another reason why a slight thickening appears on the skin. The disease appears when infection or dirt gets into the hair follicles, where the inflammatory process develops. In most cases, this disease affects people who are overweight, have diabetes, or have weak immune systems. In this case, there is no need to remove the formation. A course of antibiotics and anti-inflammatory drugs is sufficient for treatment.
- A furuncle is a purulent inflammation of the hair follicle. The problem can be identified by severe itching and pain when pressing. This compaction appears when personal hygiene rules are violated, the immune system is weak, or hypothermia occurs. The development of the boil occurs within 2-4 days. These days, the lump gradually increases in size, acquires a red tint, is very painful and has a white core - pus.
- Inflammation of the lymph nodes on the side of the neck on the left or right. It is characterized by mild pain when pressed in the area of enlargement, as well as near the ear or under the lower jaw. Several lymph nodes can become inflamed at once, for example, in the armpits or groin. In addition, the person experiences a severe headache, weakness or chills, and there is also an increase in temperature to 37-38 degrees. This happens when a virus enters or during an inflammatory process of any organ. Enlarged lymph nodes on the neck on the right or left without pain are a dangerous signal. At this time, the body may develop lymphogranuloma or lymphocytic leukemia.
- A malignant tumor is characterized by a hard structure that resembles a stone when pressed. During palpation, severe pain appears, the formation practically does not move to the side. With the development of a malignant process, the tumor does not go away on its own, but only increases in size. A painful lump often occurs when cancer cells appear in the lymph nodes or thyroid gland.
Making a diagnosis on your own and starting treatment is not the best idea. Otherwise, the signs may go away and the disease will be asymptomatic. This will make it difficult to make a correct diagnosis and prescribe effective therapy.
Foreign bodies of the larynx and trachea in children
Foreign bodies (FB) of the larynx
Foreign bodies of the larynx, although less common than in the underlying tracts, pose a greater threat to the life of the child due to varying degrees of stenosis. Such children are usually admitted shortly after aspiration. The wide prevalence of cases of foreign bodies entering the larynx in childhood is due to both anatomical and physiological properties and underdevelopment of the child’s defense mechanisms, especially premature children, in whom protective reflexes are sharply reduced (B. M. Shevrygin, 1989).
In the larynx, a foreign body is retained primarily by protrusions formed by the vestibular and vocal folds. This body can then end up in Morgani's pockets. Much less often, the delay occurs in the anterior commissure or arytenoid region. An acute foreign body, for example a needle, a bone fragment, under the influence of uncontrollable coughing movements, penetrates deeper and deeper into the mucous membrane and underlying tissue. The consequence of this can be bleeding, catarrhal swelling and even submucosal laryngitis. In the Morganian pouch, a foreign body can remain in the resulting ulcer, which becomes covered with granulations and can heal in the form of a connective tissue scar. A foreign body can also linger in the subglottic region. It gets into the larynx when a child, holding an object in his mouth, inadvertently inhales. Such cases are very common, for example, during eating, laughing, screaming, crying, in other words, with all forms of forced breathing. Small flies and mosquitoes sometimes enter the larynx when yawning due to the deep inhalation that occurs. A child may choke on any food product or pull it into the larynx and trachea when trying to speak or in sudden fright (A. Risenberg, 1900; M. F. Tsytovich, 1922; A. Klinik, 1931; B. M. Mlechin, 1954; and etc.).
The sudden onset of the disease is a very significant symptom, indicating the presence of a foreign body in the larynx (I. M. Rosenfeld, 1958). As a result of a wide variety of foreign bodies entering the larynx, acute asphyxia occurs.
The most characteristic symptom of a foreign body in the larynx is stenosis, which, even with small FB sizes, can be the result of a reflex spasm of the muscles of the larynx itself. After a foreign body enters the larynx, the first attack of suffocation reaches its greatest extent and is usually accompanied by redness or cyanosis of the face. According to P. G. Lepnev (1956), in case of sudden persistent stenosis, one should always suspect the closure of the airways by a foreign body. Gradually increasing phenomena of stenosis are characteristic of pathological processes developing around a foreign body, or swelling of a foreign body. The initial period lasts, as a rule, 10-30 minutes, after which, due to the exhaustion of protective reflexes, calm occurs. After this, in certain positions of the foreign body, a latent period of the disease may begin, during which the patient does not experience any discomfort. However, such cases are the exception rather than the rule. Dyspnea is always inspiratory in nature. But thin and sharp foreign bodies (pins, sewing needles, nails, fish bones), when fixed in the subglottic region, cause swelling of loose connective tissue with subsequent development of stenosis.
Sometimes a foreign body stuck in the larynx changes its position; in such cases, there is an alternation of shortness of breath with periods of rest. Another constant symptom is a violation of voice function up to aphonia. But in cases where the foreign body gets stuck not between the folds, but in the subglottic space, this symptom may not exist.
Voice dysfunction can be short-term or long-term. According to P. G. Lepnev (1956), the first often appears as a result of overstrain of the vocal folds during the initial period and soon passes. With prolonged persistent hoarseness following aspiration, it is more likely that the foreign body is in the larynx and either mechanically interferes with phonation or has already injured the elements of the larynx. And if in the first case there is usually a sharp degree of aphonia, then in the second we are talking about a moderate disorder of the vocal function, accompanied by a roughening or slight hoarseness of the voice.
The manifestation of a disorder of vocal function some time after aspiration is characteristic of secondary changes in the larynx itself due to injury caused by a foreign body or a hysterical cough. However, an unexpectedly sonorous voice may also indicate the displacement of a foreign body from the larynx either into the underlying sections or outward, and vice versa, due to pinching of a ballistic object in the larynx, the voice may suddenly disappear. Sound breathing caused by narrowing of the larynx and trachea is called stridor (creaking) or stirtor (snoring). It is known that all kinds of forms of dysphonia and aphonia are observed due to a functional disorder of the nervous system, and the reasons for the disorder of the vocal function can be very diverse, which detracts from the diagnostic value of this symptom. Nevertheless, persistent pronounced aphonia, which occurred suddenly after aspiration, gives the right to consider this sign to be very reliable (P. G. Lepnev, 1956). A frequent symptom of a foreign body in the larynx is a cough, which has a pronounced paroxysmal character and sometimes does not stop day or night. In some cases, cough is accompanied by vomiting, whistling and hemoptysis (Yu. F. Isakov, S. P. Orlovsky, 1979; A. I. Tsyganov et al., 1986).
Hemoptysis is also observed in cases where a foreign body has sharp edges and injures the mucous membrane, as well as due to the formation of granulations during prolonged stay in the respiratory tract. In the literature there are descriptions of cases of leeches getting into the larynx. A feature of this living foreign body is the ability to quickly increase in volume, as a result of which asphyxia is possible. At the same time, since the blood sucked by the leech does not clot due to the presence of hirudin, the resulting bleeding is profuse and prolonged. If the leech is torn during removal, then bleeding into the trachea and underlying parts of the tracheobronchial tree can be fatal. P. G. Lepnev (1956) believed that the entry of a leech into the larynx causes the originality of the clinical picture: rapidly increasing, but usually unstable difficulty breathing and periodic hemoptysis. Sometimes a leech, sucked at the entrance to the larynx, moves and touches the vocal folds, thereby causing repeated bouts of severe coughing.
Pain syndrome occurs when a foreign body enters from the outside, for example during wounds. In these cases, there must be a wound channel through which this body penetrated into the laryngeal cavity. We have described two such cases. In one of them, a broken chip from a beech crutch, when hit on the neck, passed through the left plate of the thyroid cartilage in the area of the laryngeal ventricle and with the other end wedged into the right ventricle, as a result of which the folds lost their mobility and were fixed in one position. Attempts to phonate and swallow caused a sharp painful reaction. In another case, a fragment from a metal press penetrated through the anterior section of the right plate of the thyroid cartilage and ended up in the thickness of the ventricular fold with a small exit from it into the cavity of the laryngopharynx, where, during swallowing movements, it scratched the back wall of the pharynx and even the body of the 5th cervical vertebra, where the broken piece fell part of it (up to 3 mm long). Only three and a half months later these bodies were removed, and the pain syndrome disappeared.
In this case, the appearance of pain during swallowing, characteristic of foreign bodies in the pharynx and esophagus, can be observed when angular and pointed objects are fixed in the larynx or trachea. Localized pain behind the sternum in the depths, especially manifested during coughing or sudden movements, is characteristic of foreign bodies in the lower segment of the trachea and bronchi (P. G. Lepnev, 1956), stabbing pain in the throat with irradiation to the ear - for foreign bodies in the larynx (B. M. Mlechin, 1956).
Anamnestic indications of aspiration of a foreign body do not necessarily indicate that it is in the respiratory tract.
In children with acute respiratory disease, its onset may be accompanied by a loud barking cough, in which facial cyanosis and respiratory failure are observed at the height of the attack. In young children, the moment of aspiration in most cases goes unnoticed. Yu. F. Isakov and S. P. Orlovsky (1979) believe that this circumstance “is a feature of foreign bodies in the respiratory tract in young children and complicates not only diagnosis, but also treatment,” and therefore “with a protracted atypical course of pneumonia, it is always the possibility of undetected aspiration should be kept in mind.”
During the initial examination of a child, special attention should be paid to his breathing and skin color. The child, stripped to the waist, is examined in diffuse bright lighting. The number of respirations, their depth, the duration of inhalation, exhalation and respiratory pauses, the uniformity of excursions of the right and left halves of the chest, as well as the participation in breathing of auxiliary muscles, the wings of the nose, inspiratory lowering of the larynx, retraction or swelling of the jugular and supraclavicular fossae, intercostal spaces and epigastric region. Pay attention to the sonority of breathing, which can be silent, noisy, asthmatic, stridor, whistling. A forced position, which allows one to avoid coughing attacks and pain with an appropriate medical history, should be interpreted in favor of an indirect sign of a foreign body (P. G. Lepnev, 1956). M.F. Isakov and S.P. Orlovsky (1976) noted that in children “with foreign bodies in the larynx, when percussing the lungs, the sound is boxy, and during auscultation, weakened breathing is heard. Fluoroscopy data indicate a uniformly increased transparency of the lung fields.”
According to E. M. Aleksandrovskaya (1927), characteristic signs of foreign bodies in the larynx are stenotic breathing with difficulty inhaling, weakened fremitus pectoralis in the apex to the clavicle and rough dry rales in both lungs, more pronounced in the upper lobes. In this case, one can often observe a sudden retraction, especially in young children, of the supra- and subclavian cavities and the jugular fossa due to increased compensatory work of the sternocleidomastial and scalene muscles (B. M. Mlechin, 1954). Mlechin argued that “in the absence of reliable anamnestic data and clinical indications for direct laryngoscopy, the patient must be hospitalized, especially for children.” This provision remains relevant today. In cases where the moment of aspiration of a foreign body with its characteristic signs goes unnoticed by others and parents, the child is delivered with symptoms of asphyxia as a result of developed edema, and the doctor does not have time to make an accurate diagnosis, since his primary task is to restore breathing and eliminate the immediate danger of suffocation.
With foreign bodies remaining in the larynx for a long time, there is a high risk of mistaking the resulting granulations for a manifestation of respiratory papillomatosis, which can lead to medical error.
Thus, one of the patients had a denture plate in the right half of the larynx for a long time, which, due to whitish-colored deposits, was mistaken for a fungal infection of the larynx.
The diagnosis of a laryngeal foreign body is made on the basis of medical history, clinical symptoms and additional research methods. Currently, the main auxiliary method for diagnosing aspirated foreign bodies is x-ray examination (X-ray machines: OKO KRT, pr oline, OPERA, Medix-R, Arkom-2, Multix). A radiograph in a lateral projection according to the method of G. M. Zemtsov and direct tomograms, especially in children of the older age group, with radiopaque foreign bodies help to accurately localize them. Reactive and inflammatory manifestations, even in the presence of non-contrast foreign bodies, may indicate the affected side.
According to B.V. Shevrygin (1989), “tactics are dictated by the child’s condition.” Laryngoscopy has an important differential diagnostic value, since the detection of other diseases in many cases allows us to exclude the presence of a foreign body in the larynx. Therefore, indirect laryngoscopy (laryngoscopes: ENF-T3, Reda, Karl STORZ, Miller, Optima, LRVS-3) should be performed if a foreign body is suspected in all patients in whom it is technically feasible. If a mirror examination of the larynx cannot be carried out, then if a foreign body of the larynx is suspected, direct laryngoscopy must be performed (M. F. Tsytovich, 1922; B. M. Mlechin, 1954; P. G. Lepnev, 1956; A. G. Likhachev, 1971; and many others).
M. F. Tsytovich o.
In modern conditions, providing emergency care to children with foreign bodies in the respiratory tract requires highly qualified otorhinolaryngologists and anesthesiologists, as well as sufficient equipment and equipment. Foreign bodies should be removed in those medical institutions where there are conditions for endoscopic manipulation under anesthesia. Currently, almost all city and regional otorhinolaryngological departments have such capabilities. If there are no conditions for providing qualified specialized care, children with foreign bodies in the larynx and trachea must have a tracheotomy before being transported to a specialized institution (V.K. Trutnev, 1952; B.M. Mlechin, 1954; P.G. Lepnev, 1956; I M. Rosenfeld, 1958; A. G. Likhachev, 1971; etc.).
Sometimes after surgery, a ballistic foreign body pops out when coughing through the tracheostomy. M. A. Shuster et al. (1987) believe that transporting a child with a foreign body can pose a danger to his life. Therefore, children with foreign bodies in the larynx and ballistic bodies in the trachea should be considered non-transportable. A. G. Likhachev (1971) points out that “it is better to transport children with floating foreign bodies in a sitting position, so as not to cause displacement of the foreign body and possible suffocation.”
B.V. Shevrygin (1989) believes that a child with a foreign body in the trachea should be taken to the hospital in a sitting position in an ambulance, where, if necessary, he is given artificial respiration, given oxygen to breathe, and cardiovascular drugs are administered.
The overwhelming number of foreign bodies of any location that enter the child’s respiratory tract must be removed under anesthesia through natural routes using direct laryngoscopy. Adequate pain relief is achieved by intravenous or inhalation anesthesia such as nasopharyngeal. The currently widespread intravenous anesthesia with injection ventilation of the lungs cannot be used to remove foreign bodies from the larynx, since the powerful air flow coming from the injector can displace the foreign body into the underlying parts of the respiratory tract (M. A. Shuster et al., 1987).
When the aspirated object is localized in the larynx and upper trachea, the method of choice for endoscopy is direct laryngoscopy. The manipulation is performed quickly during apnea after mask hyperventilation for 3–5 minutes under conditions of total intravenous anesthesia with myoplegia. If it is necessary to continue the intervention, the patient is hyperventilated again and laryngoscopy is quickly performed again. The disadvantages of the proposed method are obvious. Due to the difficulties that may arise with mask artificial ventilation of the lungs or the possibility of bleeding during manipulation, it is dangerous to use this method. In addition, the time allotted to the surgeon for manipulation (1–1.5 minutes) is clearly not enough for successful and atraumatic removal of a foreign body, even with repeated attempts.
Laryngoscopy can be performed under so-called nasopharyngeal anesthesia. In this case, mask fluorotane-oxygen induction anesthesia is usually performed; after reaching the surgical stage of anesthesia, one or two catheters, respectively, are brought through one or both nasal passages to the entrance to the larynx. Anesthesia is maintained by administering a gas-narcotic mixture through these catheters. Due to the fact that the maintenance of anesthesia occurs virtually in an open circuit, the management of deep anesthesia is extremely difficult. We must also not forget that the surgeon has to work in an atmosphere with a high content of narcotic substances.
It should be noted that the use of fluorotane, which promotes sensitization of the myocardium to sympathomimetics and consequently leads to arrhythmias, limits the possibility of using drugs for anemia of the bronchial mucosa and granulations at the site of fixation of a foreign body, which worsens the conditions of manipulation.
If it is impossible to remove a foreign body through natural routes, its retrograde extraction through a tracheostomy is indicated.
Thus, the described methods of general anesthesia for the removal of foreign bodies of the larynx and upper trachea have a number of very significant disadvantages that limit their use and do not allow one to be confident in the possibility of successful laryngotracheoscopy.
However, the previously proposed methods of manually removing foreign bodies from the larynx blindly, as well as the use of a laryngoscope, which was administered to children without any anesthesia, currently have no supporters.
And medications (expectorants) are even less reliable when it comes to achieving the removal of a foreign body by coughing, so in this case you should forget about them. The latter method, in addition to its low efficiency, is also fraught with the loss of precious time (I. M. Rosenfeld, 1958). Therefore, if the appropriate conditions cannot be created on site, it is necessary to immediately send the patient to a medical institution where he can receive special assistance.
Tracheal foreign bodies
The clinical picture is very peculiar. Symptoms of respiratory failure are present in all cases, but it is not as pronounced as when a foreign body is localized in the larynx. There is a paroxysmal whooping cough, which is especially worse at night when the child is restless. Coughing attacks can be prolonged, painful, sometimes with vomiting, may be accompanied by cyanosis of the face, and in case of strangulation of a foreign body when it is displaced into the larynx, cause asphyxia. When a foreign body enters the trachea, a “piggy bank effect” occurs. Irritation of the reflexogenic zones of the larynx prevents the coughing up of a foreign body due to the rapid closure of the vocal folds, which contributes to its release in the trachea. It is a characteristic sign of unfixed tracheal foreign bodies that is the balloting symptom, which has great diagnostic significance. With anxiety, crying, laughter and coughing, flotation (“flapping”) is clearly heard, which occurs as a result of a foreign body floating and hitting the walls of the trachea and vocal folds during inhalation and exhalation. At this moment, a popping sound is heard, similar to the one that occurs when uncorking a bottle of sparkling water. Balloting of a foreign body is often heard at a distance, and is even better determined by listening with a phonendoscope or by placing the palm of the hand on the front surface of the neck. You can also hear a whistling sound resulting from a narrowing of the air stream between the walls of the trachea and the foreign body itself.
Balloting of a foreign body in the trachea can continue for a long time. At the same time, according to P. G. Lepnev (1956), “a foreign body can be retained in the trachea only in rare cases. To do this, it must either have a size that allows it to pass through the glottis and make it impossible for it to penetrate the bronchus, or a special shape that allows it to cling to the walls of the trachea or get wedged between them.” Getting into the right or left main bronchus at the moment of inhalation, ballistic foreign bodies can cause bronchospasm with contraction of the bronchioles, which immediately sharply worsens the patient’s condition (Yu. F. Isakov, S. P. Orlovsky, 1979).
The condition of patients with foreign bodies fixed in the trachea can be very severe. Breathing is rapid and difficult, retraction of the compliant areas of the chest is observed, and acrocyanosis is pronounced. The patient tries to take a position in which it is easier for him to breathe. The voice is usually clear. On percussion, a box sound is noted over the entire surface of the lungs, and on auscultation, breathing is weakened on both sides.
Particular attention should be paid to foreign bodies located at the tracheal bifurcation. This localization poses a great danger due to the threat of displacement of the foreign body in one direction or another and closing the entrance to the main bronchus, which causes its complete obstruction with the development of atelectasis of the entire lung. Such localization of foreign bodies presents certain difficulties for diagnosis and, most importantly, threatens severe breathing disorders. In the trachea, due to the weak expression of loose connective tissue fiber, a hyperergic reaction to the introduction of a foreign body does not occur, therefore, given its localization, respiratory disorders are more often a consequence of the entrapment of an object in the lumen of the glottis or the alternating closure of the lumens of the main bronchi during voting. The presence of the membranous part, which is quite easily extensible, makes it impossible to completely close the lumen of the trachea even with swollen aspirated foreign bodies. In the worst case, only significant difficulty breathing and drainage disorders can be observed.
An object in the trachea rarely remains in one position for a long time. Sometimes it runs, sometimes it closes either the right or the left bronchus more strongly. Children in whom foreign bodies are fixed at the tracheal bifurcation, as a rule, are admitted to the hospital with severe breathing problems: inspiratory, less often expiratory, shortness of breath, pallor of the skin, anxiety, etc. Balloting of a foreign body syndrome is most often absent.
At the first examination of the child, the impression may be created of the presence of asthmatic bronchitis or severe pneumonia (M. A. Shuster et al., 1987).
In these cases, an X-ray examination becomes crucial, which can confirm or exclude pneumonia, although, according to A.I. Feldman, S.I. Vulfson (1957), in young children the temperature rises already in the first hours after a foreign body enters the trachea . At the same time, the rise in temperature in a two-year-old child a day after the fact of aspiration of the seed, noted by the parents, and a subsequent tracheobronchoscopy, during which grayish films containing Leffler’s bacilli were found, gave V.K. Trutnev (1952) grounds to challenge the conclusions drawn the doctor conducting the examination, since he did not pay attention to the increase in temperature. This means that an increase in temperature cannot serve as a direct sign of the presence of a foreign body in the upper respiratory tract. Both M.F. Isakov and S.P. Orlovsky (1979) are inclined to this conclusion: “It is especially easy to mistake a foreign body migrating in the trachea for a respiratory infection. These diseases can be differentiated by high body temperature and catarrhal symptoms characteristic of infection.”
Obstructive emphysema occurs as a result of valve blockage of the trachea or bronchus and is caused not only by the presence of a foreign body, but also by swelling of the bronchial mucosa, accumulation of mucus, and fibrin deposition. Valvular tracheal stenosis leads to swelling of both lungs and is defined as uniform swelling with increased transparency of both lungs, which does not change with breathing. A low position of the diaphragm and widening of the intercostal spaces are also noted.
According to the opinion of E.M. Aleksandrovskaya (1927), if a foreign body of the trachea lies closer to one of its walls, then a weakening of the vocal tremor is noted at the corresponding apex of the lung. If the foreign body is located at the bifurcation of the trachea, closer to one of the main bronchi, then a slight muffling of sound is recorded in the corresponding lung. These symptoms are nonspecific, as they also occur in other diseases of the lungs and pleura, therefore some authors deny the importance of percussion and auscultation for recognizing foreign bodies (B. M. Mlechin, 1954).
With perforation of the tracheal wall, the formation of subcutaneous emphysema and penetration of air into the mediastinum, pleural cavity and neck are possible.
At the same time, small metal objects that have penetrated into the wall of the trachea and caused attacks of coughing, suffocation and other characteristic symptoms can subsequently remain in place for a long time and not cause any particular inconvenience to the patient (A. I. Feldman, S. I. Vulfson, 1957 ; and etc.).
When inserted into the trachea, sharp cutting objects cause superficial or deeper wounds to the mucous membrane. If the wound becomes subsequently infected, an ulcer may develop. Prolonged residence of these bodies causes the organization of granulations, and when the latter are replaced by scar tissue, persistent stenosis can occur. Therefore, when a foreign body remains fixed in the wall for a long time, inflammatory changes can significantly transform the anatomical relationships and distort the picture obtained during tracheobronchoscopy, making diagnosis difficult even for an experienced specialist (V.K. Trutnev, 1952).
Radiography and fluoroscopy (OKO KRT, Medix-r, OPERA, Arkom-2, Multix) play a certain role in the diagnosis of tracheal foreign bodies, especially metal ones. In many cases, this study helps to establish the nature and location of the aspirated object, its shape and determine which part of it is wedged into the mucous membrane. In a number of patients, it is possible to establish the change and position of the foreign body or its movement, especially with a polypositional study. Additional contrasting using various contrast agents, which B. M. Mlechin (1954) reminded, causes a very wary attitude on the part of other scientists (M. I. Perelman, 1972) due to possible complications. It should be recalled that in children, large foreign bodies fixed within the cervical part of the esophagus or deep in the laryngopharynx can compress the larynx or trachea, which is accompanied by severe breathing difficulties. B. M. Mlechin (1954), in differential diagnosis, draws attention to the possibility of compression of the respiratory tract by peribronchial glands, an enlarged thymus gland and a leaky abscess of tuberculous origin. The disintegration of tuberculous peribronchial glands due to their breakthrough into the respiratory tract can lead to immediate suffocation. V.K. Trutnev wrote about this complication (1952). A clinical picture of the presence of a foreign body in the trachea can be given by a polyp or other tumor of both the trachea and the main bronchus (M. I. Perelman, 1972), as well as goiter, anomalies of the aorta (double arch, etc.).
In most cases, foreign body aspiration is indicated by anamnesis, which is often unreliable and sometimes misleading. Information about aspiration may be absent in mentally ill patients, small children, as well as in case of endogenous foreign bodies (conglomerates and plugs of thick mucus and pus, clotted blood, fibrinous films and “casts”, pieces of caseous or calcified masses from peribronchial lymph nodes affected by tuberculosis) . An unclear history or complete absence of anamnestic data with negative results of an x-ray examination serves as justification for diagnostic laryngotracheobronchoscopy. It is also a necessary therapeutic measure. At the same time, many authors consider the possibility of performing other interventions to be a prerequisite for its implementation, the main one of which is tracheotomy (V.K. Trutnev, 1952; B.M. Mlechin, 1954; M.I. Perelman, 1972; etc.).
The main treatment measure is urgent removal of the foreign body. This also applies to the so-called “chronic foreign bodies”, due to the possibility of their sudden displacement and entry into the glottis area with subsequent asphyxia.
When choosing a method for removing a foreign body from the trachea, one must keep in mind its location, degree of mobility, shape, size, consistency, age and individual characteristics of the patient. V.K. Trutnev (1952), B.M. Mlechin (1954) at one time noted that the following methods can be used to remove tracheal foreign bodies: 1) direct laryngoscopy; 2) upper tracheobronchoscopy; 3) tracheotomy; 4) lower bronchoscopy. But already in 1987 M.A. Shuster et al. argued that foreign bodies of the trachea and bronchi, in the presence of modern Friedel-type bronchoscopes, should be removed only using subanesthesia tracheobronchoscopy, regardless of the patient’s age. At the same time, the remark of V.K. Trutnev (1952) is not outdated: “It is impossible to propose any single rule, the application of which will certainly ensure successful extraction of a foreign body.”
V. G. Zenger , Doctor of Medical Sciences, Professor of MONIKI, Moscow
How to recognize the disease
When a ball appears under the skin on the neck, a person may not feel any worsening of the condition at all. You should carefully monitor the well-being and behavior of the seal.
During the development of malignant tumors, a person sometimes does not experience pain in the area of the lump. The lump often reaches large sizes and is visible to the naked eye even under clothing. Most often, cancer is accompanied by weakness, chills, loss of strength, itching, loss of appetite, sudden weight loss and a temperature of up to 38 degrees.
If the lump is a wen or atheroma, then it does not hurt and moves under the skin. The boil develops quickly and causes severe pain, as well as itching and redness of the tissue.
Diagnosis and treatment of the disease
To accurately find out the diagnosis and begin treatment, you should first visit a surgeon. The doctor sends the patient for an ultrasound examination and, possibly, to an oncologist. However, this does not mean that a malignant tumor has been found in the body. A thorough examination by several doctors can help rule out certain diagnoses and prescribe effective therapy. Other necessary research procedures may also be prescribed: general blood test, x-ray, biochemistry and biopsy. In order not to blur the picture of the disease, it is not recommended to use medications before going to a specialist, and especially not to try to squeeze out or open the subcutaneous ball.
After undergoing the necessary diagnostic procedures, the patient is prescribed treatment. The following treatment regimen is possible:
- taking antibiotics, anti-inflammatory or antiviral drugs when an infectious disease is confirmed;
- a small incision or puncture to remove fluid from cysts and wen;
- surgical removal of a cancerous tumor, wen or cyst.
You can relieve inflammation using folk methods, for example, compresses with medicinal herbs, honey, lard or Vishnevsky ointment. It is strictly prohibited to use iodine or alcohol! They have a warming effect and increase the inflammatory process.
Sakania Luiza Ruslanovna
Dermatovenerologist, cosmetologist, trichologist
Ask a Question
If after treatment there is no relief within 2 weeks, you should definitely visit your doctor again. Also, while taking medications, you must give up alcoholic beverages and smoking.
Algorithm of action when a lump is detected in the throat
You can detect a lump on the back of the throat at home by visual inspection. If you experience discomfort while breathing, eating, or have a lump in your throat, you should examine your mouth with a mirror.
After identifying a lump, it is necessary to exclude provoking factors, monitor the cleanliness of the oral cavity, and consult a doctor. The specialist will conduct the necessary studies that will help determine the cause of development and the nature of the disease: pharyngoscopy, MRI, biopsy.
To eliminate the tumor, a course of therapy is prescribed taking into account provoking factors, the individual characteristics of the patient, and the nature of the tumor. It is not recommended to resort to self-medication or removal of the lump. Incorrect, untimely treatment can lead to the development of undesirable consequences, complications and death.
A ball under the skin on a child's neck
The appearance of a lump on the left or right side of a child’s neck will tell not only about the diseases described above, but also the so-called childhood diseases - mumps, mononucleosis and others. Children may also develop lipomas, atheromas, tumors and boils. To determine the exact cause, you need to visit a pediatrician or pediatric surgeon.
Most often, young patients are diagnosed with a wen, which is not dangerous to health. The cause of compaction is also the lymph nodes. Most often, such a ball does not reach more than 1 cm. Lymph nodes become inflamed during infectious diseases in the body, diseases and teething, otitis, measles, acute respiratory infections or inflammation of the tonsils. It is necessary to urgently visit a doctor if:
- the compaction became very hard and increased sharply;
- the lump hurts a lot and cannot be moved with your fingers when pressed;
- the area around the growth has changed color to bright red or blue, and is also covered in a rash;
- a core of pus appears on the ball, which begins to ooze over time;
- Several more lumps appeared both near the first bump and in other places.
If the child was previously diagnosed and prescribed treatment that does not bring results within 7 days, this is a reason to undergo the examination again. Perhaps there was an error in the analysis or the wrong medications were selected.
There is no need to be afraid of a lump, even if it has appeared and is rolling under the child’s skin. It is better to identify the pathology at an early stage and begin treatment. Therefore, if even a small nodule is detected, it is recommended to seek help from a surgeon. Reduced immunity, severe stress against the background of a suspicious ball and refusal of therapy will only worsen the condition.
You can ask your question to our author:
Factors that provoke the formation of lumps in the throat
The appearance of a tumor in the throat is accompanied by various symptoms.
Signs of the development of pathology are:
- pain while eating;
- impaired breathing;
- sensation of a foreign object in the throat;
- purulent discharge;
- a sore throat;
- high body temperature;
- hoarseness in the voice;
- inflammation of the tonsils.
The symptoms of the disease depend on the provoking factors.
The main reasons for the appearance of compaction are:
- colds, viral diseases;
- flu;
- thyroid dysfunction;
- infection;
- complications after tonsillitis;
- diseases of the kidneys, digestive system;
- cardiovascular diseases;
- hormonal imbalances;
- metabolic disorders;
- chronic respiratory diseases;
- radiation exposure.
A neoplasm of the larynx can be a manifestation of paratonsillitis, retropharyngeal abscess, syphilis, oncology, or benign tumors.