From this article you will learn:
- how is bone grafting performed in dentistry,
- bone grafting methods – price 2021,
- Jaw bone augmentation for a dental implant: reviews,
- forum of patients and implantologists.
Bone grafting during dental implantation (synonym – bone augmentation) is a surgical operation that allows you to increase the volume of bone at the site of installation of one or more dental implants. The need to increase bone volume is dictated by the fact that after the removal of teeth in a person, the bone tissue in the area of missing teeth undergoes gradual atrophy, which leads to a decrease in the width and height of the alveolar process of the upper and (or) lower jaw.
Bone tissue growth during dental implantation is necessary not only for the normal functioning of the implant (from the point of view of bearing the chewing load), but also for aesthetic reasons. The fact is that too thin bone walls around the implant are always subject to resorption (absorption) - as a result, the gum level drops and the metal neck of the implant is exposed. More than 90% of all negative reviews from patients after implantation relate specifically to the unsatisfactory appearance of the gums around the neck of the implant.
Scheme of bone grafting –
The optimal thickness of the bone walls around the implant is
→ Implantation techniques that do not require bone grafting
The most important points (according to Fig. 1) –
1) Firstly , the thickness of the vestibular bone wall (i.e., the one located on the side of the lip/cheek) should be at least 2.0 mm, and 2.5 mm is very good. If the front surface of the implant is covered with bone less than 2 mm thick, this means 100% bone resorption around the implant neck, accompanied by lowering of the gum level and exposure of the dental implant neck. In this case, the implant will still bear a functional load, however, if it stands in the smile zone, the appearance of the gums around the implant will eventually become aesthetically unacceptable.
2) Secondly , the thickness of the bone wall between the implant and the root of the adjacent tooth should preferably be at least 2.5 mm. If this distance is less (for example, 1.5-2.0 mm), then the following problem arises. The fact is that even normally there is always slight bone resorption around the neck of the implant. If the bone partition between the implant and the tooth root is too small, bone resorption will occur not only around the implant, but also at the root of the adjacent tooth. This means a lowering of the gum level and the absence of an interdental gingival papilla (i.e., there will definitely be poor aesthetics).
3) Thirdly , the thickness of the bone wall between two adjacent implants should ideally be 3.0 mm. If it is less, then, as in the previous case, this means significant resorption of the bone septum between the implants, and as a consequence of this process - receding gums in this area, absence of the gingival papilla, exposure of the implant (i.e. poor aesthetics).
Causes of bone deficiency:
1) The main reason for the decrease in bone tissue volume is the natural atrophy (resorption) of bone, which occurs in the area of extracted teeth. This happens because the bone loses support in view of the tooth root, and also because in the absence of the tooth root, chewing pressure ceases to be exerted on the bone tissue. As a consequence, there is a decrease in bone volume, which can occur both in height and in width of the alveolar process of the jaw.
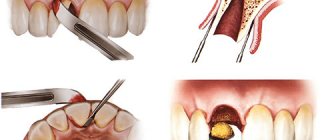
2) The second reason is the traumatic removal of decayed teeth by dental surgeons. Usually, during removal, the surgeon does not think at all about the safety of the bone walls of the alveoli around the tooth, biting them off with forceps. If you are planning extraction followed by tooth implantation, then it is best to carry out such removal by an implant surgeon, who will try to preserve the bone tissue as much as possible.
There are 3 types of bone resorption –
- horizontal resorption (Fig. 2), when the width of the alveolar process decreases,
- vertical resorption (Fig. 3), i.e. when there is a decrease in the height of the alveolar process,
- + combined form.
According to the type of resorption in a particular patient, a bone grafting technique is selected, aimed at increasing the width and/or height of the alveolar process of the jaw.
Bone grafting for dental implantation: reviews
There are many different bone grafting techniques, but they can be divided into 2 large groups. Firstly, horizontal bone augmentation techniques aimed at expanding the narrow alveolar process. Secondly, vertical bone augmentation techniques aimed at increasing the height of the alveolar crest.
The most commonly used techniques are
- splitting of the alveolar process,
- bone block transplantation,
- technique of guided bone regeneration (GBR),
- sinus lift method (used for insufficient bone height in the lateral parts of the upper jaw).
All these operations are performed under local anesthesia; if necessary (at the patient’s fear), intravenous sedation can be performed.
The duration of the operation can be from 1 to 2 hours, which will depend on the technique used, the volume and complexity of the operation. The stitches are removed on the 10th day. Important: all methods have their pros and cons... Histological studies have shown that after bone augmentation using different methods, a completely different structure of the newly formed bone tissue is observed, which can lead to subsequent resorption of the newly formed bone. In addition, a lot depends on the nature of the bone material being implanted.
Osteoplasty – what is it and why is it needed?
When introducing a titanium root, it is very important that it is surrounded on all sides by bone. If there is a deficiency of tissue, the titanium pin will be rejected. Moreover, if the root is installed in the upper jaw, there is a risk of touching the maxillary sinuses, which can lead to serious ENT diseases. Also, if there is insufficient bone, the implant will become loose and sink below the gum, which will affect the aesthetics of the prosthesis and the overall picture.
Osteoplasty is recommended in the following cases:
- if it is necessary to install a root in an area where a tooth was removed several years (or months) ago;
- if the patient has anatomically large maxillary sinuses;
- when physiologically a person has a minimum volume of hard tissue.
The operation is not performed if:
- the patient has chronic ENT diseases (sinusitis, sinusitis, rhinitis);
- lack of calcium in the body;
- there are pathologies in the structure of the respiratory system;
- oncology;
- polyps and other formations in the nose;
- diabetes.
Also, osteoplasty is not performed on pregnant and lactating women. Otherwise, the operation is done relatively quickly and with a guarantee.
In many cases, patients are recommended to take a course of hormonal medications and antibiotics before surgery in order to neutralize edema and possible inflammation.
Splitting of the alveolar process -
Used in horizontal bone resorption to increase the thickness of the alveolar process. Can be performed on both the lower and upper jaws. It must be said that this is the most effective method of expanding the alveolar process today, which also has a low cost (it does not require expensive bone materials and membranes). There are several varieties of such splitting, but we will especially focus on the “Split-Control” technique, which allows for simultaneous expansion and installation of implants.
The content of the “Split-Control” technique (Fig. 5-10) - after detachment of the mucoperiosteal flaps (gum) in the center of the alveolar ridge, a cut is made with a milling cutter or other special tools to the height of the future implant (Fig. 6). Next, a pilot drill is used to mark a hole for the implant(s) and spreaders are screwed into the prepared holes (Fig. 7). By using different sizes of spreaders from smaller to larger, you can increase the width of the ridge and immediately install the implant.
There is always a gap left on the sides of the implant, which is filled with bone material, which, if necessary, can be applied in excess to the outside of the alveolar process, covering it all with a special resorbable membrane (Fig. 9). After which the wound is sutured, and we wait for osseointegration of the implant within 3-4 months.
Bone grafting of the lower jaw (splitting method) –
Advantages of the technique –
- Firstly , thanks to the splitting of the ridge, we get a bone defect that has bone walls on all sides (except on top).
Thanks to this, rapid and high-quality osteogenesis (new bone formation) occurs, because the spongy bone deep in the alveolar process is rich in blood vessels, osteoblasts, mesenchymal cells, growth factors... Speaking of why it is much worse to increase the width of the bone not due to splitting (from within the alveolar process), and do this by externally attaching bone blocks or bone chips outside cortical plastic surgery of the alveolar process (24stoma.ru). The fact is that the outer cortical layer of bone is very dense and there are practically no blood vessels in it. Accordingly, the implanted bone material will take a very long time to grow blood vessels, bone formation will be slower, and there will be a greater risk of failure and complications of such bone grafting.
- Secondly , there is no need for expensive bone materials and membranes, again due to the fact that this is a three-wall defect inside the alveolar process, and not outside it. There are enough inexpensive materials, for example, the bone material "Osteodent-K" and the membrane "Osteodent-Barrier". But if you are principled, then you can also use expensive materials like “Bio-Oss”.
- Thirdly , installation of implants with this technique is possible in most cases immediately. If the implants are installed later, then only 3-4 months will have to pass between operations, which is significantly less compared to other bone grafting methods.
Splitting of the alveolar process: animation and video of the operation
Important: There are several types of splitting techniques. With “Split-Control”, the cutter makes only a cut along the crest of the alveolar process + a pair of vertical cuts to the thickness of the cortical plate. But there is a variation of this method, where an additional horizontal cut is made at the level of the tops of future implants, which leads to complete detachment of the bone block (vestibular cortical plate).
Then this block is fixed with screws, which often break it. With this modification of the technique, implants are not installed immediately, but after 3-4 months. In addition, it is quite traumatic and there is a greater risk of complications. This type of technique should only be used for the thinnest alveolar process (2 mm), but some doctors use it even in cases where this is not necessary.
Bone block transplantation –
This method can be used both to increase the width of the alveolar process and its height. This technique predominantly uses an autogenous bone block (this means that the bone block is taken from the patient himself in other areas of the jaws). The block can be collected in the area of the tubercle or zygomatic-alveolar ridge of the upper jaw, or in the area of the ramus or mental area of the lower jaw. Bone blocks of allogeneic and xenogeneic origin (bovine bone) are used less frequently, which is associated with their much lower efficiency.
An example of a bone block transplantation operation - in photos 11-16 you can see an example of how bone grafting of the upper jaw (in the area of the central incisor) is performed using two bone blocks. Please note that 2 blocks were used because in this case it was necessary to increase both the width and height of the alveolar process in the area of the extracted tooth.
Bone blocks are first screwed to the bone using special titanium micro-screws (Fig. 12). The block can be additionally covered with bone shavings, after which the blocks and surrounding bone tissue are necessarily covered with a collagen membrane (exactly the same as those used for the guided bone regeneration technique). The membrane is fixed to the bone using special metal pins (Fig. 14), and after this the mucous membrane over the operation site is sutured tightly.
Bone block transplantation: animation and video of the operation
The pros of this method are that it is an excellent method for increasing bone volume with predictable results. The gold standard when using this method is the use of an allograft (a bone block taken from the patient himself). Moreover, it is very important that the graft being transplanted is “cortical-spongy”, i.e. had not only a cortical plate, but also cancellous bone tissue. In this case, you can get a predictable and positive result from a bone block transplant.
Disadvantages of this method –
- Additional surgery is required to remove the bone block.
- Secondly, with this technique, the possibility of simultaneous installation of implants is most often excluded, because this greatly increases the risk of rejection of both the implant and the bone block itself.
- Thirdly, such bone blocks require longer engraftment, i.e. After such an operation, it will be necessary to wait about 6-8 months before installing implants at all. This is because the bone block is screwed to the outside of the jaw. The superficial cortical layer of the jaw bone has very few vessels, and therefore the growth of vessels into the transplanted bone block occurs very slowly.
- Fourthly - again due to the slow growth of the bone block by blood vessels (during the subsequent installation of the implant at the second stage) - sometimes the bone block can be separated from the jaw due to its insufficient integration with the bone tissue of the jaw.
Guided tissue regeneration (GTR) –
This method can also be used to increase both the width of the alveolar process and its height. In addition, if the lack of bone tissue volume is not critical, then simultaneous installation of implants is possible along with bone grafting. However, the method also has its drawbacks, which we will discuss below.
Directed tissue regeneration (synonymous with directed bone regeneration) involves the use of two components: firstly, implanted bone material, and secondly, a special barrier membrane, the use of which will isolate the bone defect from the effects of adverse factors.
Guided bone regeneration: examples of operations
1) Clinical case No. 1 - in photo 17 (in the area of planned implantation) a significant bone defect is visible, which will be filled using a bioresorbable membrane and Bio-Oss bone material. In photos 21-22, taken 5 months after inert grafting, you can see the installation of the implant in this area...
2) Clinical case No. 2 – the use of guided bone regeneration techniques simultaneously with the installation of implants. The materials used were the inert material “Bio-Oss” and the resorbable membrane “Bio-Gaid”...
The significance of the barrier membrane - the barrier membrane performs the following functions: it allows you to give the desired shape and volume to the area of bone tissue being built up, protects the grafted bone from being absorbed by osteoclast cells (located in the periosteum), prevents the mechanical impact of the soft tissue of the gums on the grafted bone material and its deformation...
There are different types of membranes, resorbable (Bio-Gaid), non-resorbable (Gore-tex or titanium mesh membranes). The former dissolve on their own over time and do not need to be removed, but they hold their shape much worse compared to mesh titanium membranes or membranes with titanium reinforcement. All these membranes are expensive, but the use of cheap membranes (such as Osteoplast) is not suitable for this technique.
Selection of bone material - there are many different materials: based on synthetic hydroxyapatite, biopolymers, tricalcium phosphate, bioglass, based on bovine bone, etc. Below we will focus on the most effective types of bone materials (in descending order of their effectiveness).
- Use of a bone autograft – an autograft should be understood as bone material that is taken from the patient himself in other parts of the jaws (for example, in the form of bone chips or a bone block). There is only one downside - the need for an additional small intervention to collect bone material.
- A combination of autograft + xenograft - in a 1:1 ratio, bone chips (taken from the patient) are mixed with material of xenogeneic origin, i.e. based on bovine bone. An example of this is such high-quality and effective material as “Bio-Oss”. This is a very effective combination for increasing bone volume.
- The use of allograft - this type of bone material is also very effective, but is used much less frequently. The fact is that the source of bone material in this case is cadaveric material (of other people). These materials are purchased from a special tissue bank; all materials undergo careful processing and are completely safe, but for psychological reasons they are used less frequently.
- The use of pure xenograft - the Bio-Oss material (based on bovine bone) can be used without mixing it with the patient’s own bone chips, but then the efficiency of bone augmentation will be lower.
Guided bone regeneration with simultaneous implantation: video of the operation
- Video 1 – using Bio-gaid resorbable membrane,
- video 2 - using a mesh titanium membrane.
Important: it should be noted that this method is not always effective enough. The fact is that the bone material is “planted” outside the cortical plate of the jaw (a very dense surface layer of bone). The newly formed bone differs in structure from the native jaw bone, does not have its own cortical plate on the outside and therefore has a tendency to subsequent partial resorption.
Therefore, it is necessary to carry out bone augmentation using this method “with a reserve” for the planned degree of future resorption, which will be more pronounced the thinner the gum biotype (gingival thickness). This is due to the fact that the surface layers of the bone will receive less oxygen and nutrients due to their less blood supply.
Bone tissue augmentation during dental implantation: price 2021
How much does jawbone augmentation for a dental implant cost in 2021?
Augmentation of bone tissue for implantation - the cost will differ from the type of technique and the volume of the operation (in the area of how many teeth it is performed), as well as from the type and volume of bone material and membrane used. Bone tissue augmentation during dental implantation: price 2021
- Splitting of the alveolar process - in the area of 1-2 teeth will cost about 15,000 rubles + the cost of materials, which in this case can be used inexpensively and the materials will cost 3-5 thousand rubles.
- The operation to collect and transplant a bone block will cost about 36,000 rubles (this cost includes both the collection and transplantation of a bone block, but does not include the cost of additional materials, for example, a membrane, which will cost another 13,000 rubles).
- The technique of directed tissue regeneration - the NTR technique in the area of 1-3 teeth will cost approximately 25,000 rubles (excluding the cost of the membrane and bone material).
If we take high-quality European materials, then the cost of the Bio-Guide membrane is about 13,000 rubles, and the cost of the Bio-Oss bone material (0.5 g packaging) is about 12,000 rubles. If this technique is carried out simultaneously with the installation of an implant, then the price of the service (excluding the cost of bone material and membrane) will be from 5,000 to 10,000 rubles - in addition to the cost of installing the implant. Additionally, the patient will incur costs for bone material and membrane (prices are indicated above).
- Sinus lift surgery is performed in the lateral parts of the upper jaw and consists of raising the bottom of the maxillary sinus. The cost of a closed sinus lift starts from 10,000 rubles, an open one – from 25,000 rubles, but keep in mind that this cost does not include additional materials (membrane, grafted bone material).
Sinus lifting: cost in Moscow
The cost of the procedure is by no means secret information, quite accessible to everyone on the Internet; when comparing prices in different clinics, it is important to consider what is included in the list of services. Most often, the cost of the operation is indicated, taking into account all types of diagnostics and consumables. You can find prices for dental services on the prices page.
We guarantee the quality and effectiveness of the procedure to our patients. It should be borne in mind that the final decision regarding the method of operation can only be made by a specialist after appropriate diagnosis.
Bone grafting: complications
Bone grafting during dental implantation - reviews will depend on the surgeon’s precise execution of the surgical technique. Any deviation from the surgical technology most likely leads to failure and even rejection of the transplanted bone. In addition, in most cases, a lot depends on the quality of the bone material used, the membrane.
With both surgical techniques, the membrane may be exposed through the suture line, which in many cases leads to purulent inflammation of the wound. The use of a bone block grafting technique with insufficient vascularization rate can lead to sequestration (rejection) of sections of the bone block or its entirety. Both with purulent inflammation and with sequestration, it will be necessary to remove all materials from under the mucous membrane (both membrane and bone material).
In addition, when using bone blocks, there is a loss of volume of the bone block during the process of integrating it into the tissue - sometimes up to 50%, which can be critical and require repeated surgery. It is also possible for the implanted bone block to tear off (during screwing in the implant at the second stage), which is due to insufficient integration of the block into the jaw’s own bone tissue.
Important for smokers: jaw bone grafting (as well as the installation of implants itself) is a relative contraindication in smoking patients, especially heavy smokers. The fact is that nicotine leads to a sharp narrowing of the lumen of blood capillaries in the tissues of the oral cavity, which sharply reduces blood flow to the bone graft or implant. Lack of blood flow leads to insufficient supply of oxygen and nutrients to the tissue, which interferes with both bone formation and simple osseointegration of the implant.
If you want bone tissue augmentation for dental implantation to proceed without complications, you must stop smoking at least 2 weeks before bone grafting surgery and for 4 months after surgery. If the implants are not installed simultaneously with bone grafting, but at the second stage, you will have to quit smoking again at the same time. If you are unable to quit smoking, you may want to consider dental implants that are designed specifically for smokers and do not require bone augmentation.
Choose the right experts
For the operation to be successful, you should choose the right specialist and clinic so that the treatment is carried out without additional costs. Patients are offered a choice of materials for implantation in different price categories. The doctor also selects the method of surgery, taking into account the characteristics of the patient’s problem.
Contact our clinic today to correct a natural defect and feel the joy of life again. Professionals will make your smile irresistible and help you regain lost self-confidence! To find out the current price in St. Petersburg and insert a tooth implant, contact any of our specialized specialists.
Alternatives to bone grafting –
In some cases, the use of small-diameter implants allows one to completely avoid or significantly reduce the amount of bone grafting. The fact is that for implants of small diameter, much less bone tissue is required. There are Straumann implants with a diameter of only 2.9 mm, and made of the unique material Roxolid (an alloy of titanium and zirconium). This material is much stronger than titanium and also has significantly better osseointegration - compared to implants made of ordinary titanium.
Thanks to these characteristics, the implant remains, firstly, mechanically strong, and secondly, it is able to bear a significantly larger volume of chewing load (compared to larger diameter implants made of traditional titanium). The only disadvantage of implants from this Swiss manufacturer is their higher price.
But if the bone height is insufficient (in situations where bone grafting in a patient is considered undesirable, for example, for medical reasons), another type of Strauman implants can be used, which is called “Standard Plus Short”. This type of implant is only 4.0mm long, which is the shortest internally connected screw implant available on the market. It is used specifically when the bone height is insufficient.
Instead of an epilogue. What are the best biomaterials?
Geistlich Biomaterials, definitely)))). Because RegenerationDay.
Not only patients, but also osteoregenerators would like to hear the answer to this question, and perhaps not at all from me, but from Vladimir Vladimirovich Putin, a more authoritative person. For in all medical forums, in all professional communities, in all discussion forums, there are endless debates about what is better and why.
In my opinion, to answer this question, it needs to be, at a minimum, reformulated. Something like this: