Periodontitis and periodontal disease - what are these diseases?
Periodontitis and periodontal disease are often confused with each other, considering them one disease with different names. Both in a neglected state actually lead to the same consequences - bone tissue atrophy and further tooth loss, have a pathological effect on the entire body, but at the same time they differ from each other in the nature of their occurrence, causes of development and symptoms. To understand the difference between periodontal disease and periodontitis, let's look at their definitions.
- Periodontitis is an infectious inflammation of the complex of tissues (periodontal) surrounding the tooth. It occurs as a consequence of gingivitis - superficial inflammation of the gums, which without treatment becomes chronic and affects the deeper layers of tissue - not only the gums, but also the cementum of the root, periodontium, and the upper part of the jawbone.
The prevalence of periodontitis is indicated by the figures: after 35 years, signs of this disease occur in 86% of cases, while 20% of dental patients have a severe form of this disease[1].
- Periodontal disease is a periodontal disease, which is based on tissue degeneration, disruption of their nutrition and, as a result, destruction. Periodontal disease is much less common; as an independent disease it is diagnosed in only 3-5% of patients. However, many experts attribute it to complications of gum inflammation, i.e. when they are literally “healed” to such an extent that their nutrition is disrupted, there is no longer inflammation, there is simply dystrophy.
New teeth in 1 day - All-ON-4 - 180,000 rub.
All inclusive!
3D modeling of the structure with a prosthesis, implantation of 4 Osstem implants, installation of a fixed prosthesis on the same day. Free consultation with an implantologist +7 (495) 215-52-31 or write to us
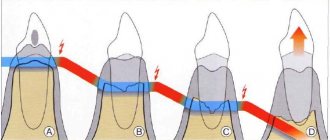
Bone atrophy of the lateral areas of the jaw
When molars are lost, a cosmetic defect such as sagging of the facial skin due to loss of bone tissue is observed. Another unpleasant complication can be considered a change in bite: in the front zone of the jaw, the teeth begin to “move apart”, the height of the face changes due to a decrease in the height of the jaw bones. A removable bridge prosthesis installed in the lateral area of the jaw not only does not stop the process of bone resorption, but also accelerates it. This is due to the fact that during chewing the denture puts pressure on the gum. To avoid strong pressure from the “bridge”, prosthetics should be carried out using a bridge-like prosthesis installed on implants. This way you can stop the change in bite and eliminate the risk of “sagging” of the face.
How diseases arise - features and differences
The reasons are the main thing that distinguishes these diseases. In most cases, inflammation of the gums and periodontitis are caused by prolonged accumulation of bacterial plaque and stone on the enamel and under the gums. It is poor and irregular oral hygiene that initially provokes slight inflammation of the gums, and its penetration deep into the tissue is a matter of time. Pathogens and mechanical trauma to the mucous membrane lead to irreversible processes in the periodontium[2].
Insufficient and unsatisfactory oral hygiene is the main, but not the only cause of the disease. A share of 10% falls on general diseases of the body, which serve as an impetus for the development of pathology, namely diabetes, osteoporosis, leukemia and others.
What is the difference between periodontal disease and periodontitis in dentistry? In addition to the terms and manifestations themselves, the difference is also in the reasons, which are not fully understood. On the one hand, the disease is non-inflammatory in nature and is caused by metabolic disorders. It is known that periodontal disease begins not from the gums, but from the bone parts of the jaw, where sclerosis of the feeding vessels occurs - a reduction in the diameter of the vascular tubes. For this reason, the supply of oxygen and necessary substances to all tissues is disrupted, which leads to the gradual death of cells. Most often, this is how the first (mild) stage of this disease develops. However, the next two are interrelated with periodontitis and are its consequence.
Also, long-term and conservative treatment of gum inflammation leads to periodontal disease, in which the infectious component is removed, but nothing is done to restore tissue (in the moderate and severe stages).
Alternatives to bone grafting –
In some cases, the use of small-diameter implants allows one to completely avoid or significantly reduce the amount of bone grafting. The fact is that for implants of small diameter, much less bone tissue is required. There are Straumann implants with a diameter of only 2.9 mm, and made of the unique material Roxolid (an alloy of titanium and zirconium). This material is much stronger than titanium and also has significantly better osseointegration - compared to implants made of ordinary titanium.
Thanks to these characteristics, the implant remains, firstly, mechanically strong, and secondly, it is able to bear a significantly larger volume of chewing load (compared to larger diameter implants made of traditional titanium). The only disadvantage of implants from this Swiss manufacturer is their higher price.
But if the bone height is insufficient (in situations where bone grafting in a patient is considered undesirable, for example, for medical reasons), another type of Strauman implants can be used, which is called “Standard Plus Short”. This type of implant is only 4.0mm long, which is the shortest internally connected screw implant available on the market. It is used specifically when the bone height is insufficient.
Key differences in disease manifestations
With periodontitis, there are three stages or degrees of the disease - mild, moderate and severe - without treatment, the disease increases over time. And the symptoms, accordingly, depend on the duration of inflammation. In general, the disease is characterized by acute redness of the mucous membrane, the formation of a large amount of plaque and hard stone on the teeth and under the gums. Due to the lack of comprehensive treatment, inflammation from the gums spreads to the bone, which gradually literally “melts” and shrinks in volume. In this case, mobility of the elements necessarily occurs with their subsequent loss from the hole. The photo below makes it clear what we are talking about.
With periodontal disease, the gums do not become inflamed, but decrease in size due to metabolic disturbances and become “whitish” (this sign can be seen in the photo). The patient may not even be aware that the bone tissue is shrinking. The disease can proceed completely unnoticed and will gradually lead to tooth loss. The condition of bone tissue can be determined by X-ray examination - there are three stages of development of periodontal disease depending on bone loss - mild, moderate, severe.
What is the danger of bone resorption in the frontal zone of the jaw?
The area where the incisors are located is a very thin bone, the degeneration of which occurs very quickly. Even if you install a bridge using, for example, fangs as a support for the “bridge,” after a while the gums will begin to collapse due to loss of bone, and the teeth will visually lose support. If the lost incisors are restored as a result of implantation, the implant replacing the root seems to give a command to the body that the tooth is in its place and resorption is not needed.
Comparison of characteristic symptoms of two pathologies
How these diseases differ from each other can be judged from the table.
At the initial stage
| Periodontitis | Periodontal disease |
|
|
In the middle stage
| Periodontitis | Periodontal disease |
|
|
At a severe (advanced) stage
With periodontal disease at this stage, bone tissue atrophy reaches 2/3 of the height of the roots, the teeth cannot be held in place - mobility occurs, the roots are exposed by 6 mm or more, pain increases while eating, even to the point of refusing to eat and oral hygiene in order to do not cause pain, dental units look unattractive - visually large crowns and narrow elongated roots violate the aesthetics of a smile.
The following symptoms occur with periodontitis:
- gums can be either inflamed and swollen, or pale due to lack of nutrition,
- severe pain with any impact, even with tongue movements and conversation,
- there is burning and itching,
- suppuration intensifies, pus is contained in large quantities under the gums,
- plaque and stone surround the tooth on all sides, fill periodontal pockets,
- periodontal pockets reach 5 mm or more,
- Pathological mobility of teeth occurs (grades II and III), when the teeth deviate not only to the sides, but also up and down by a distance of more than 1 mm, and can rotate around their axis. Often they are held in the holes only by accumulated stone,
- the root of the tooth is exposed more than half of its height,
- bone tissue declines catastrophically, its level has dropped to half the height of the root,
- teeth have nothing to hold on to - they begin to fall out,
- Traumatic occlusion occurs (closing of the jaws), malocclusion due to the loss of individual units.
Important! At the last stage, periodontitis can take on an acute form, when all the symptoms sharply intensify. Then patients experience fever, increased body temperature, severe pain and suppuration. All this affects both a person’s physical well-being and his psychological state - many people experience stress and depression due to problems in the oral cavity very acutely.
In this case, periodontitis can (though quite rarely) develop locally in one area or be generalized - widespread throughout the entire oral cavity. Periodontal disease is always a generalized form, when the disease affects both dentitions, and not individual units.
In addition to destruction in the oral cavity, the disease harms the entire body, affecting the functioning of internal organs. It has consequences for many systems and organs, no less dangerous than itself.
Completely edentulous
When all teeth are lost, the resorption process accelerates significantly. And in addition, there is a change in the structure of the jaws: the muscles slightly change the places of attachment to the bone. An unnatural sagging of the lips begins, and wrinkles appear. Changes in the structure of the jaws lead to disruption of chewing function, which negatively affects the health of the entire body, since a person cannot eat properly. Due to impaired chewing of food, the process of its digestion changes. This is the direct relationship between missing teeth and human health in general.
With complete edentia, some patients choose removable dentures for both jaws. But since prostheses do not stop the process of bone resorption and even accelerate it, after some time it is necessary to adjust the size of the prosthesis, changing its thickness, in order to compensate for the loss of bone tissue. However, if you install a removable bridge supported by implants, the bone crest of the gums is preserved, since the pressure of the “bridge” on the gums is eliminated. In the absence of tooth roots, resorption continues, but its rate slows down.
Complications that occur if the disease is not treated
In addition to destruction in the oral cavity, chronic inflammation harms the entire body, affecting the functioning of internal organs - the gastrointestinal tract, heart, liver and kidneys, and has a destructive effect on blood vessels. The culprit is pathogenic bacteria, which weaken the immune system and cause diseases no less dangerous than periodontitis. Thus, microorganisms of the oral cavity, together with food and saliva, penetrate into the stomach and intestines, causing digestive disorders - gas formation, indigestion and pain, followed by gastritis, duodenitis and other diseases [3]. There are cause-and-effect relationships between stomach diseases and disturbances in metabolism and in obtaining all the necessary microelements and vitamins.
An even more dangerous complication of chronic inflammation is kidney disease, such as pyelonephritis and renal failure. They develop in a non-obvious way: the bloodstream brings pathogenic microorganisms to the kidneys, where the immune system destroys “strangers”, as elsewhere, but the proteins of pathogens at the molecular level are very similar to kidney cells - the immune defense also works on the kidney’s own cells, simultaneously destroying them.
Periodontitis affects both blood vessels and the heart. All the same pathogenic bacteria cause endocarditis, heart attacks, heart attacks, affect the brain, 3 times increasing the likelihood of Alzheimer's disease. Scientists have proven the connection between the disease and a 6-fold increase in the risk of stroke and diabetes. 8 times more likely to develop pregnancy complications (miscarriage, premature birth, low birth weight) if the child’s mother has periodontitis.
Advanced periodontal disease provokes the development of periodontitis, which significantly worsens the clinical picture and requires complex and long-term treatment.
What is the diagnosis of diseases based on?
Accurate determination of the disease and its stage will allow timely and appropriate treatment to begin. But, unfortunately, many clinics limit themselves to x-rays and visual assessment of the oral cavity, which does not always allow a detailed understanding of the problem. But, in addition to the symptoms, for successful treatment it is necessary to determine the cause of the disease and evaluate what was the impetus for its development. To do this, a differential diagnosis is carried out, consisting of several successive stages:
- the doctor examines the oral cavity, noting signs of disease. Using instruments, measurements are made of the depth of periodontal pockets, the amount of deposits,
- an anamnesis is collected about the time of the disease, its manifestations, the patient’s feelings, as well as the quality of oral hygiene,
- to assess the condition of the bone and get details of the problem, a computed tomography (CT) scan is performed,
- Bacterial plaque and stone from periodontal pockets are taken for examination to determine the composition of the microflora and its resistance or sensitivity to drugs,
- The diagnosis is completed with blood tests (general and sugar); additional blood tests for hormones may be needed.
Diagnosis of periodontal disease at the initial stage of the disease is difficult due to the non-obviousness of the symptoms and is also not limited to one visual examination. However, even at the first stage, radiography can detect bone atrophy. The diagnosis is made on the basis of an orthopantomogram and visual and instrumental examinations. For greater accuracy, microscopic examination of the gums is used to assess the degree of disruption of microcirculation in them.
How to protect bone from atrophy: treatment of periodontitis and periodontal disease
Over decades of dental research and practice, many methods have been found to treat gums, dental ligaments and jaw bones with periodontitis and periodontal disease. In recent years, developments in microbiology and advances in the field of periodontics and biomaterials have brought the latest effective developments and drugs. Some time ago, periodontitis was considered an irreversible disease, and even at the initial stage it was necessary to take into account the fact that with all methods of treatment and prevention, a temporary result was achieved, albeit for a long time - for several years. Today, the first two stages of the disease can be successfully treated in adults and children, as well as restoration of bone and gum levels thanks to advanced methods and drugs.
To achieve results in restoring oral health, an integrated approach is essential. To treat this disease, you cannot choose just one effective and proven method, since you need to influence the problem from all sides: it is important to eliminate the cause, stop the inflammatory process and subsequently restore the periodontium and ligamentous apparatus.
However, at the third chronic stage of the disease, considerable treatment efforts are, as a rule, insufficient to completely eliminate the disease, and the only solution remains to remove the remaining affected teeth as the source of inflammation and the focus of the disease.
Periodontal disease has a different clinical picture, and the treatment of this disease is based on other methods. Let's look at them in more detail later in the article.
What methods of treating periodontitis exist and is it possible to restore bone tissue?
In each specific case, an individual comprehensive approach is chosen for treatment, depending on the manifestations of the disease and the time of its course. It is important to understand that treatment of the disease is long, complex, multi-level and quite expensive. It also provides for the simultaneous solution of several problems:
- stopping infectious inflammation,
- prevention of further spread of the pathological process,
- preservation of the functions of the dental system,
- prevention of complications,
- prevention of effects on the entire body and health in general.
Professional oral hygiene
The very first and mandatory stage is cleaning the teeth and periodontal pockets from deposits. The elimination of a huge number of pathogens contained in plaque and stone is carried out using ultrasound, devices such as Vector and Varios. Antiseptic treatment of the enamel and gum surfaces is also required to create a smooth and favorable environment for further treatment. Cleaning allows you to eliminate deposits on the surface and at a depth of up to 3 mm under the gums.
Closed and open gum curettage
These methods involve surgical intervention when the depth of deposits is more than 3 mm, and professional cleaning alone is not enough. Using a special dental instrument - a curette - periodontal pockets are cleaned and granulations are removed at a depth of 4 mm. If the deposits are even deeper, then open curettage is used. In this case, a gum flap is removed to allow access to and cleanse the affected tissue. After cleansing, the gums are returned to their place and stitches are applied.
Drug therapy
Along with cleansing the enamel and roots, a course of treatment with antibiotics is prescribed to strengthen the gums and improve tissue nutrition. During the year they return to courses up to 5-7 times.
Plasmolifting, or PRF membranes
This method involves the use of one's own protective and regenerative mechanisms. Point injections into the gums of the patient's blood plasma with his platelets promote rapid tissue healing and relief of inflammation. Blood cells rich in a special protein, fibrin, “seal” damaged and bleeding vessels and restore gums, thereby reducing inflammation.
Mandatory and regular independent oral hygiene
Without it, all therapeutic measures will be ineffective and simply useless. It is important to maintain the achieved results at home and independently prevent deposits in the oral cavity. Brushing with a toothpaste, using floss and brushes after each meal, and using antibacterial rinses are mandatory measures for patients.
Splinting mobile teeth
At the stage of mobility of units, bone atrophy reaches such a level that they can no longer be held in the sockets on their own. Further loosening of them will only speed up the moment of falling out - they are fixed artificially with special splints. Mobile units are combined into a group with relatively healthy ones using fiberglass or metal splints or a splinting prosthesis (clasp).
Important! Splinting without accompanying drug therapy and the above treatments will cause even more harm over time. If you simply splint a row and leave the periodontal areas without treatment and strengthening, then quite quickly, under load, the units of the dentition will loosen even more and fall out as a whole group along with the splint.
Application of biomaterials with active growth factors
Combining all of the above methods with advanced developments in the field of nanotechnology and biomaterials has made it possible to create revolutionary therapeutic periodontal complexes designed for a year. They can not only stop the development of periodontitis, but also reverse it. In the first two stages of the disease, up to 80% restoration of damaged areas is possible within a year thanks to the use of innovative materials and drugs. The Straumann company, one of the leaders in the field of implantology, has developed a new generation of biomaterials enriched with growth factors (primarily Emdogain® for gum restoration, artificial bone materials BoneCeramic®, Bio-Oss®), which allow you to return and re-grow lost during the disease process, root cement, periodontal ligaments, raise the level of bone and gum.
All of these methods are highly effective in the initial and middle stages of the disease. At the third advanced stage of inflammation, this approach will also bear fruit, but the solution will be temporary. At some point, the patient will still be faced with the question of prosthetics: despite the treatment, advanced periodontitis cannot be completely cured. Read below about how the issue is resolved at this stage of the disease.
Numerous scientific works in dentistry, otorhinolaryngology, traumatology and plastic surgery are devoted to the study of the structural features and topography of the facial part of the head, gender characteristics and age dynamics.
The anatomical structure of the bones of a given area largely determines its functionality. In particular, the features of the maxillofacial area of the head determine the functional ability of the digestive and respiratory systems, the phonetic apparatus, and also have great aesthetic significance.
At the same time, the development of bone tissue of the alveolar process is of interest to specialists from the field of practical dentistry, including those involved in the issues of dental implantation. Understanding this process largely determines the outcome of treatment.
It is necessary to take into account the pronounced dependence of the structure of the maxillofacial region on a number of physiological and pathological factors, primarily on the age-related restructuring of the bone tissue of the jaws, in particular their alveolar areas.
Numerous sources of scientific literature contain a large amount of information about the course of these processes, but over the past decades there has been a pronounced tendency towards changes in their duration and timing compared to the data of fundamental research 40-50 years ago.
Obviously, the reasons for such deviations are various factors, the influence of which on the body has intensified over the past few decades, both in connection with technological progress and the lifestyle of modern man. First of all, the condition of the oral cavity, jaws and teeth is strongly influenced by improper and irrational nutrition, low level of oral hygiene, as well as living in environmentally polluted areas.
Factors that influence the course of the formation and development of both the body as a whole and the maxillofacial region in particular include the phenomenon of acceleration, which is also confirmed by numerous scientific sources.
The research results convincingly prove that today, much earlier than indicated in the sources of the last century, the processes of eruption and replacement of teeth occur, which means that the period of their intramaxillary development is significantly reduced. As a result, the degree of mineralization of their hard tissues at the time of tooth eruption into the oral cavity is insufficient, and this, in turn, leads to rapid destruction of crowns and premature tooth loss.
Sources of professional dental literature indicate that another cause of adentia is the high incidence of periodontal diseases. Domestic and foreign authors confirm that pathological processes affecting the periodontium extend to the bone tissue of the alveolar processes of the jaw, the mucous membrane of the gums and the root of the tooth, leading to the loss of practically healthy teeth and, as a result, the restructuring of the alveolar areas.
It is necessary to take into account the complex anatomical structure of the upper jaw and the presence of the maxillary sinus, characterized by individual differences, the relative position of the sinus, the roots of the maxillary dentition and the bone tissue of the alveolar process of the upper jaw in different age periods. An in-depth study of these anatomical formations is important to ensure high-quality restoration of the structure and functionality of the dentofacial apparatus in pathological conditions of various etiologies, as close as possible to physiological ones.
Patterns of formation of skull bones
The processes of formation and development of the musculoskeletal system, in particular the skeletal system, have always attracted the attention of researchers. Domestic and foreign authors continue to thoroughly study the features of development and age-related restructuring of the skull, especially its maxillofacial part.
Numerous scientific studies are devoted to the study of the characteristics of the formation of the skull during the intrauterine period of ontogenesis. The author of the fundamental work “Fundamentals of Medical Craniology” V.S. Speransky described 3 stages of the intrauterine period of skull development - membranous, cartilaginous and bone.
At the first stage, the components of the membranous skull are mesenchymal cords, the placement of which is associated with the growth of the embryo’s head. Starting from the fourth week of intrauterine development, the formation of a cartilaginous skull occurs, the development of which originates from the occipital bone and spreads in the ventral direction. Ossification of the cartilaginous skull begins in the 3rd month of intrauterine development, but in some bones of membranous origin, ossification centers appear earlier.
The process of ossification of the skull has been well studied, but the results obtained often differ significantly from each other (according to 28 authors, there are from 115 to 120 ossification centers in the skull, some of which lie in the cartilage, some in the mesenchymal base).
However, the vast majority of researchers argue that the first points of ossification in the areas of jaw formation are formed in the 7th week of embryogenesis, and the boundaries between individual bones of the skull at the sites of future sutures are visualized starting from the fourth month of intrauterine development.
It is known that most skull bones have several centers of ossification, and therefore at the time of birth of a child the number of skull bones is much greater than in adulthood, and the fusion of individual parts in such bones continues for a certain time after birth.
The characteristic appearance of the embryo is determined by the gill arches, which are formed during 4-5 weeks of intrauterine development. The formation of the jaws begins in the cartilage zone of the first branchial arch, which consists of a dorsal part (maxillary protrusion located under the orbit) and a ventral part (mandibular protrusion), which contains Meckel's cartilage and forms a kind of rod. Around the latter, the formation of the lower jaw occurs.
Numerous studies by morphologists, anthropologists, craniologists, as well as representatives of practical medicine, whose area of professional interest is the area of the head, as well as organs and systems associated with it functionally or topographically, have been devoted to the study of the patterns of development of individual bones of the skull.
V.S. Speransky claims that the formation of the skull is characterized by an uneven course in different time periods. In particular, until the end of the intrauterine period of development, the skull is 70-80% represented by formed bone tissue. In this case, the bones of the base of the skull are separated by cartilaginous layers, between the bones of the vault there are remnants of membranous tissue that forms the theme, expanding at the intersection of the sutures, and the bones of the facial skull are combined using syndesmoses.
The development of the head, the bony basis of which is the skull, after the birth of a child is characterized not only by an increase in size, but also by a change in the shape and spatial relationships of its component parts. In particular, this concerns the relationship between the brain and facial areas of the skull.
Each of them is characterized by a different type of growth and depends on the structural and functional characteristics of a given area. The bones of the cranium are structurally connected to the brain and its membranes, as well as to the sensory organs. The bones of the facial skull, primarily the jaw, are associated with teeth of both generations and depend on the course and duration of the processes of their formation, formation, growth, development, change and loss, as well as on the degree of pneumatization of the air-bearing bones.
The upper jaw, frontal and sphenoid bones contain air sinuses, and the ethmoid bone contains a labyrinth. All this determines certain features of the growth and formation of bones in the maxillofacial region, which today attract the attention of scientists and practicing doctors.
Growth and remodeling of skeletal bones in general, and the skull in particular, occur as a result of the synchronous flow of two interrelated processes - opposition and resorption of bone tissue. Thus, the restructuring of bone structures is especially important for the upper jaw, since simultaneously with changes in its size and external shape, processes of formation and restructuring of the maxillary sinus, anlage, development, eruption and replacement of teeth occur in the thickness of the bone body.
Another significant feature characteristic of the head skeleton is that at different age periods the intensity and direction of growth of the skull changes. This fact must be taken into account in pediatrics, especially in the practice of neurosurgery, otorhinolaryngology and maxillofacial surgery.
Craniometric studies show that the size of the head changes especially rapidly during the first 3-4 years of a child’s life. Their intensity decreases somewhat at the age of 5-6 years and intensifies again after 7 years.
At the same time, different directions of growth prevail at different periods of time, and the longitudinal and transverse dimensions of the skull alternately change. The periods of the most intensive growth of the skull in length are 2-3 and 7-8 years, and the most active growth of bones in width continues during the 1st year of a child’s life.
The results of craniometric studies tell us that the formation of the alveolar areas of the jaws and the associated vertical growth of the anterior part of the face is completed after reaching 10 years of age.
The directions of skull growth in individuals of different sexes during adolescence are different. In boys, during this period, longitudinal head growth prevails, and in girls, the size of the skull increases synchronously in the vertical and horizontal directions. Scientists agree that the increase in the size of the skull in width continues in girls up to 15, and in boys up to 16 years; in height - up to 16 years for girls, and up to 18 for boys.
However, with the end of the main stage of growth and formation of the skull, its restructuring does not end. Under the influence of local factors that determine the individual characteristics of each part of the face (the intensity of the load on the masticatory muscles, the prevalence of nasal or mouth breathing, bad habits), remodeling processes continue throughout life.
This fact must be taken into account not only during surgical interventions in this area, but when planning orthodontic or orthopedic measures.
Craniometric studies undertaken in various areas of the facial skull over various time periods indicate that in the fetal period the size of the jaws increases by 3-4 times, and the most active growth is observed in width. After birth and until the formation of the permanent occlusion is completed, increased growth of the maxillofacial region occurs, as a result of which the size of the jaws in three mutually perpendicular planes increases by 7-9 times.
Development of bones of the maxillofacial region and alveolar process
Since with age the growth rate in individual areas has different dynamics, the proportional ratios of the width, height and length of the jaws change significantly throughout life. Consequently, in each age period, regardless of the general gradual slowdown in the rate of bone growth, the jaws have areas of increased and relatively slow growth.
In areas of increased growth, a quantitative increase in bone structures occurs, and in areas of slow growth, their qualitative restructuring occurs. In this regard, growth zones should be understood not as permanent, clearly defined areas, but as places where, in a given period of time, opposition processes prevail over resorption processes.
In adults, the formed upper jaw (UM) is a paired bone of a complex structure, consisting of a body and four processes - alveolar, palatine, zygomatic and frontal. The thickness of the bone body contains the air-bearing maxillary sinus (MSS), and the cells of the alveolar process contain fixed tooth roots that form the maxillary dentition.
Research shows that the alveolar process is built of spongy bone tissue, covered with a compact layer, which is better expressed on the palatal side. This structure of the bone tissue of the HF in general and the alveolar process in particular is largely determined by the load acting on the bone during chewing.
It is due to the uneven load, which is distributed and spread in a certain way by the bone beams, that in certain areas of the processes and body of the upper jaw its spongy structure is compacted, forming buttresses and thus changing the external relief of the bone.
The presence and severity of buttresses is associated both with the presence or absence of teeth (after their loss, not only the area of the alveolar process of the jaw is resorbed, but also bone tissue, a buttress is formed at the level of a given dentofacial segment and along the line of pressure distribution), and with the condition of periodontal tissues, pathology which changes the distribution of chewing load on the jaw.
Some studies are devoted to the structural features of the maxillofacial region and structures of the oral cavity, depending on the constitutional structure of the skull. The results of anthropometric studies indicate that dolichocephals always have a high palate and high alveolar processes of the upper jaw, while brachycephals always have a low palate and low but massive alveolar processes.
In adulthood, after the completion of the basic formation of the permanent occlusion and growth of the skull, a number of factors are identified that influence the condition of the bone tissue and the functional ability of the jaws. These include the general condition of the body, the presence or absence of chronic diseases and metabolic disorders, as well as the method of nutrition, which determines the load on the teeth, periodontium and jaw bone tissue.
However, of course, the main factor determining the characteristics of jaw restructuring in adulthood is the preservation or loss of teeth.
Among the causes of acquired adentia, trauma is common, as well as tooth loss due to periodontal diseases, complications of carious lesions and pathological processes in the bone tissue of the jaws (periostitis, osteomyelitis).
Restructuring of the bone tissue of the alveolar process of the upper jaw and the alveolar part of the lower jaw after tooth loss consists not only of a decrease in bone mass, a decrease in the height of the alveolar process at the level of one or several dentofacial segments. According to research results, with edentia, the quality of bone tissue also changes - the volume decreases due to a significant thinning of the bone layers, which is also confirmed by a decrease in their density.
According to a number of authors, whose professional interests concern the state of bone tissue and its age-related dynamics, changes in the density of skeletal bones, as well as its individual parts, are due to several systemic and local reasons.
General reasons include, first of all, age-related metabolic changes occurring in the body - changes leading to a decrease in the content of mineral elements (calcium) in the bones, as well as organic compounds. This mainly implies the development of osteopenia and osteoporosis.
Most scientists consider the main local reason for the decrease in the quality of bone tissue of the maxillofacial region and alveolar process to be the redistribution of the load during chewing - a sharp decrease and uneven distribution of pressure on bone tissue in edentulous areas with various types of tooth loss.
After tooth loss, atrophy of the alveolar processes occurs differently in dolichocephals and brachycephals. When the size of the alveolar process is small, bone atrophy under the influence of compression pressure increases, which causes a change in the width of the arch. The processes of bone tissue resorption have different intensities in different zones of the cellular areas, but they are most pronounced on the vestibular side.
When teeth are lost, atrophy of the alveolar process is not only an aesthetic problem. It leads to a change in the proportions of the face and may in the future become the root cause of the restructuring of a number of anatomical formations, including the displacement of the neurovascular bundles passing through the incisive and palatal canals, individual facial muscles, as well as all masticatory muscles, asymmetry of the jaws and dentition, and, as the consequence is dysfunction and even destruction of the temporomandibular joint.
Another important factor to consider when examining dental patients is the different visualization of the alveolar process in different areas of the jaw. In particular, in the central part of the jaw at the level of the incisive and canine dentoalveolar segments, the height and shape of the alveolar process are well visualized, and changes in their morphological parameters can be detected in a timely manner.
But in the lateral areas of the alveolar process, primarily at the level of segments of large molars, manifestations of bone resorption will be more difficult to establish, especially taking into account the shape, size and topography of the maxillary sinus.
Therefore, often an objective determination of the condition of the bone tissue of the alveolar process of the upper jaw in the lateral areas, both in the presence of teeth and in edentia, is impossible during a standard dental examination and requires additional examinations.
When planning surgical and orthopedic measures aimed at restoring the aesthetic appearance and functional ability of the maxillofacial area, it is necessary to take into account not only the condition of the bone tissue in general and the degree of atrophy of the alveolar process of the upper jaw in a certain area in particular, but also a number of others, no less important factors. These are the patient’s gender and age, the presence of systemic and chronic diseases, diet and quality of nutrition.
It is also necessary to take into account local factors that affect the condition of the bone tissue of the jaws, in particular the volume of previous dental interventions and the dental status in general, including the shape of the palate and the type of bite.
It should also be remembered that the presence of the maxillary sinus in the thickness of the body of the upper jaw of an adult person contributes to significant relief, but at the same time, weakening of the bone. Most often, the lowest point of the sinus is located in the projection of the first large molar, although both the shape and size of the sinus are characterized by significant variability, as well as their symmetry and relationship with the roots of the maxillary teeth.
Given the presence of a large number of scientific publications on the peculiarities of the formation and development of the maxillary sinus, its relationship with the rudiments (in the process of formation) and roots of teeth of the milk and permanent generation of teeth, the main emphasis in the study of this area is on its pathology. About 15-30% of patients in otorhinolaryngological and dental clinics suffer from sinusitis of various etiologies.
In the scientific literature we find the results of studies devoted to the study of the shape, size and degree of pneumatization of the sinuses, their topography and features of the relationship with the roots of the teeth of the upper dentition in adults and the rudiments of various groups of teeth in children and adolescents during all stages of the formation of the primary and permanent dentition.
Morphometric, radiographic and tomographic studies make it possible to classify the maxillary sinuses in accordance with the characteristics of their structure (size, shape) and the degree of pneumatization.
Researchers distinguish three types of maxillary sinuses:
- Pneumatic type: the sinus is large in size, with thin walls, the bottom goes deep into the thickness of the alveolar process, forming so-called bays, the roots of large and small molars are separated from the bottom of the sinus by a thin bone plate, and often directly contact the mucous membrane of the sinus.
- Sclerotic: the maxillary sinus is of small volume with pronounced, fairly massive bone walls.
- An intermediate type, having average characteristics between the first and second types of anatomical structure.
The relationship between the bottom of the maxillary sinus and the roots of the teeth of the upper dentition is also of great importance for practical dentistry and otorhinolaryngology.
As dental practice shows, 20% of patients have a risk of developing odontogenic sinusitis in the presence of dental pathology or dental manipulations on the teeth and periodontium of the upper dentition, since the roots of these teeth are located in the area of the bottom of the upper jaw or penetrate into the cavity. Only in 45-50% of dental patients the apices of the roots do not fit the bottom of the sinus, and the thickness of its bone wall is sufficient, that is, from 1 to 15 mm.
Of course, the cavity and walls of the upper jaw are characterized by certain age-related changes. If the formation of the sinus and its walls is completed with the completion of the formation of the permanent occlusion and the growth of the skull as a whole, then after 40-45 years, thinning of the bone walls of the sinus is observed, which progresses with age and leads to an age-related increase in bone pneumatization.
The distal areas of the upper jaw differ in a number of characteristic anatomical features. First of all, such features include the close location of the pterygoid venous plexus and the branches of the maxillary artery.
It is this topographical position of these structures that is important when planning surgical operations. Since older people have varying degrees of severity of alveolar process atrophy, during surgery the likelihood of vascular injury and massive bleeding increases.
Implications for practical dentistry
An analysis of the sources indicates that the restructuring of the maxillofacial region does not stop with the completion of skull growth, but continues throughout life.
Age-related features of the structure and topography of the maxillofacial region are closely related to a number of factors (from the general condition of the body to the method and mode of nutrition) and must be taken into account when planning therapeutic, preventive or rehabilitation measures.
It must be remembered that changes in the bone tissue of the jaws, which are quantitative in nature and diagnosed during examination of patients, are, as a rule, irreversible. Therefore, the presence or absence of qualitative changes in bone tissue, which can only be detected by additional examinations using radiation methods, is of decisive importance for dental practice.
Such an examination is necessary for the correct choice of treatment tactics for dental implantation to restore the integrity of the dentition and functionality of the jaws, and timely detection of qualitative changes in the bone tissue of the alveolar process of the jaws opens up opportunities for optimizing the choice of treatment.
Knowledge of the structural features of the maxillofacial region, understanding the patterns of their age-related dynamics is important for practical dentistry, since one of the main prerequisites for adequate diagnosis and treatment of pathological processes localized in this area.
What is the treatment for periodontal disease?
The treatment of periodontal disease differs significantly from periodontitis in methods and is aimed not at eliminating bacterial foci of inflammation, as in the first case, but at restoring nutrition to tissues, both bone and soft. For this purpose, all means are used to help restore blood circulation. However, often the moderate and severe stages of periodontal disease are combined with periodontitis and also bear all the signs of this disease. Then there is a need for a comprehensive solution.
Physiotherapeutic methods
They are presented in a fairly wide range: it is possible to use electrophoresis, phonophoresis, conventional and vibration vacuum massage, magnetic therapy, diadynamic currents and laser therapy. Each of the methods is aimed at reviving the activity of tissues subject to atrophy. Thus, electro- and phonophoresis together with the substance heparin reduces tissue hypoxia and improves blood circulation and transportation of necessary substances. Vacuum massage is carried out with a special device, creating areas of rarefaction and pressure in the tissues in order to stimulate metabolic processes. Laser therapy is also aimed at this. Treatment with such methods is a course course and requires repetition several times throughout the year.
But, unfortunately, not every clinic has its own physiotherapy department. Usually dentistry at medical universities can offer a solution to this issue.
Drug treatment
For the treatment of periodontal disease, medications have also been developed to stimulate metabolic processes in tissues. Antioxidant vitamins work for this: E, A, the entire group B, as well as P. Medicines also include anabolic steroids and blood circulation stimulants.
Partial grinding of tooth surfaces
In patients with periodontal disease, excess calcium is found in the enamel and its natural wear does not occur. This leads to the bite becoming traumatic, causing the front elements to move apart like a fan, causing pain and wedge-shaped defects. To reduce this phenomenon or prevent its development, enamel is polished in a dental office and normal tooth contacts are restored.
Splinting on mobile teeth
At the stage when tooth mobility has already occurred due to periodontal disease, they are fixed in a fixed position using fiberglass splints or clasp dentures, just as with periodontitis.
What are the obvious advantages of immediate loading implantation?
- no need for bone tissue augmentation. The volume of basal type implants is selected individually. They can be installed at an angle for reliable fixation, regardless of the size of the affected area;
- thanks to an individual approach, the master can select a design according to all parameters. It is also important that with this method the doctor can correctly calculate the interimplant pressure so that they take root as quickly as possible;
- bone tissue actively restores its original appearance - since the chewing load is immediate, this method quickly restores blood circulation, increasing the intensity of regenerative processes;
- guarantee of a positive outcome - due to the instant restoration of bone tissue, implants take root in the shortest possible time. The result will delight the patient with aesthetics, practicality and high functionality just a few months after the procedure;
- high degree of resistance to infections;
- has virtually no contraindications.
Bone atrophy, periodontitis and dental implantation
Is dental implantation possible for periodontitis and periodontal disease? It is important to understand that in the later stages these diseases cannot be completely cured. Of course, you can constantly undergo a course of treatment, do curettage, plasma lifting, and use other methods, but if you leave the diseased teeth or their roots in place, the inflammation will continue to progress.
The porous structure of the tooth serves as the environment for the development of the disease. If there is no focus of inflammation, then the pathological process caused by the accumulation of microorganisms also stops.
Many patients hope for prosthetics, but it is important to understand that in this case, classic prostheses will not help, but will only worsen the problem. Traditional bridges or dentures do not solve the problem of atrophy. Removable ones do not transfer the load to the bone, and bridges must be attached to supporting units, which require turning for this purpose (which already damages them). In the future, they too may fail, since atrophy under the “empty space” covered by the crown continues: all units move in a row into the resulting empty space, break the bridge and become loose themselves.
At the same time, restoration of oral health is possible with the help of dental implants. In general, this is the most effective method to get rid of periodontitis and periodontal disease forever. And here complex implantation often becomes the option of choice.
Modern implantation methods involve the restoration of lost units even with minimal bone volume without the need to build it up. These are all immediate loading techniques, such as All-on-4, All-on-6, basal and zygomatic technology. With the development of such a scenario, both partial implantation (restoration of a segment) and complete implantation of the entire dentition are possible.
Ways to Prevent Bone Dystrophy
To stop the resorption process, it is necessary to let the body know that the tooth root has returned to its place. This can be done in the only way: to perform a dental implantation operation by installing a titanium implant in place of the missing root. The implant, replacing the tooth root, takes over its function and stimulates the jaw bone, stopping bone resorption, which inevitably begins after tooth loss. Implants allow you to restore the functionality of the tooth, providing a natural process of chewing food. The visible part of the tooth is replaced with an abutment, which serves as a support for the crown.
Which implantation technique to choose in a specific situation?
Implantation at the initial and middle stages
If periodontitis is at an initial or middle stage, then the lost segments can be restored with implants, but under one most important condition - the remaining diseased teeth will be treated and the risk of implant rejection will be minimal. Periodontal complexes like Smile Recovery allow you to combine the treatment of periodontitis, periodontal disease and subsequent implantation. Only then can we talk about a successful result. However, there are unscrupulous dentists who offer the installation of implants near the affected elements, which is absolutely forbidden to do! In this case, there is a high risk of peri-implantitis and rejection.
If the patient has completed a course of periodontal restoration, then he may be suitable for classical two-stage implantation with delayed prosthetics - when a fixed prosthesis is placed 3-6 months after surgery. Or the express method, i.e. implantation with immediate prosthetics - here the patient will receive a full-fledged prosthesis either on the day of the operation or within 3-7 days after it. There is no need to wait here for months. The current concepts are called All-on-4, All-on-6 - they are used for mild or moderate bone atrophy, respectively.
Implantation at a late stage of pathologies
At the third stage of periodontitis or periodontal disease, it is difficult to talk about the effectiveness of conservative treatment. After examination on a computed tomography scanner, which clearly shows bone atrophy, it is recommended to remove diseased teeth and perform complex implantation with immediate loading of the prosthesis. This can even be a one-step technique, when implants are placed immediately after removal - and there is no need to wait for the hole to heal. For patients with pronounced bone atrophy and gum inflammation, solutions such as basal implantation (for the upper and lower jaw) on implants with antibacterial coating, and the zygomatic technique (only for the upper jaw) are suitable.