How to avoid removable dentures on the upper jaw in cases where, due to its severe atrophy, even bone grafting, including open sinus lift, does not guarantee the possibility of classical implantation? This problem can be solved by Zygoma zygomatic implants from the American company Nobel Biocare and Zygomatic from the Israeli manufacturer Noris Medical. Roman Bespalov, a maxillofacial surgeon and implantologist at the Smile-at-Once innovative technologies clinic in Moscow, will tell you more about the features of their use, the pros and cons of each, in an interview with Startsmile.
What brands do they represent?
Zygomatic implants are represented by two brands – Zygoma and Zygomatic (“Zygoma” and “Zygomatic”). The first ones were developed by Nobel Biocare - it was the company that first introduced such models to the world community in 1988. The Zygomatic model is a development of the Israeli company Noris Medical. In fact, this is already a copy of the Nobel Zygoma model. The second company has less clinical data and scientific research, so there are no clear recommendations for installing Zygomatic implants today. However, the models are very similar, so if we talk about usage, then in general terms it is identical.
Contraindications
Like any surgical procedure, prosthetics using Zygom has its contraindications. Here they are:
- Viral hepatitis.
- Tuberculosis.
- Oncology.
- Diabetes mellitus (in the stage of decompensation).
- Kidney failure.
- Blood clotting disorders.
- Diseases of the skeletal system that impair its ability to regenerate.
In addition, experts also highlight time restrictions:
- Young age (under 18 years old).
- Lactation.
- Pregnancy.
- Inflammatory processes in the maxillary and nasal sinuses.
In any case, before the procedure, the client will consult with a dentist, who will provide all the necessary information.
Zygomatic implantation - advantages
Usually, implantation of the upper lateral teeth requires a sinus lift - an operation to increase bone volume by raising the bottom of the maxillary sinus. The main disadvantages of this operation are associated with significant time and financial costs. In addition, we are talking about additional surgical intervention, which is always associated with health risks. In addition, often after a sinus lift the grafted bone does not take root at all or takes place to a limited extent, which means that implants cannot be placed again.
The use of Zygoma and Zygomatic implants significantly speeds up the process of dental restoration, since patients do not have to wait six months for the material to engraft and the bone regeneration process to complete before it becomes possible to install the implant and proceed to fixation of the dentures. Another advantage of zygomatic implants is that they require immediate loading with a fixed prosthesis, which is also unacceptable after a sinus lift.
Indications for the use of Zygoma implants
- complete edentia (absence of all teeth) of the upper jaw,
- partial edentia of the upper jaw – absence of a segment of chewing teeth,
- pronounced atrophy of bone tissue,
- close location of the maxillary sinuses,
- the need for rapid dental restoration,
- refusal to wear removable dentures,
- the patient’s inability/reluctance to perform a sinus lift,
- damage and trauma to the jaw, for example, if after an accident or as a result of cancer the patient has lost part of the jaw bone.
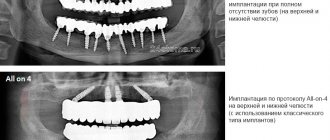
What are the features of installing zygomatic implants?
Zygoma zygomatic implants are often used when it is not possible to carry out a full implantation of the upper jaw using the classic All-on-4 (All on four) technology using traditional height implants. Thus, two or four zygomatic implants are implanted into the zygomatic bone at an angle of 30-60 degrees. During bone preparation in the maxillary sinus area, the surgeon works very carefully with the Schneiderian membrane, usually moving it away from the implant, maintaining integrity, or transsinus (less often). Also, implants can be combined with classical models in cases where, for example, there is enough bone in the frontal zone, but there is an acute shortage in the lateral zone. But, in essence, it will be an all-on-4 or all-on-6 solution, just with the addition of zygomatic models.
It should be added that, as in the case of the installation of other types of implants, planning of the entire process is carried out using computed tomography and 3D planning, which allows you to accurately determine the future location of the implant in the bone, predict the results and reduce the operation time, thanks to the specified list of necessary tools and clear task setting.
In addition, in our clinic, when performing zygomatic implantation, lithographic models are additionally used. These are exact copies of the patient’s jaws, made of plastic on a 3D printer. Even before the operation, they allow the doctor to evaluate its entire course on a model, which helps prevent mistakes.
Almost immediately after the operation, a permanent acrylic prosthesis is fixed on the installed titanium implants on a titanium beam, which is made according to individual impressions made after implantation. This allows you to maintain the attractiveness of the frontal zone of the teeth, the quality of speech and the ability to fully chew food.
Features of Zygoma implants
The length of zygomatic implants is up to 60 mm (Zygoma models from Nobel range from 30 to 52.5 mm). This allows you to use the zygomatic bone, which is not subject to thinning and inflammatory processes. As a result, the patient does not need to undergo a sinus lift, which avoids complex surgery, long-term rehabilitation and significantly reduces the final cost of treatment.
Modern Zygoma models are presented in two versions: with a straight and angular platform, i.e. beveled top edge. In the first case, angular multiunit abutments are used, in the second - straight ones. Implants with a beveled edge are specially adapted for inclined installation - in such situations, their edge will be flush with the gum, which does not require the use of angled abutments and somewhat facilitates the process of fixing the prosthesis.
In addition, implants can be two-piece or one-piece. The former require the installation of an abutment, the latter do not, because... it is immediately combined with the intraosseous part - one-piece zygomatic implants are presented in the Biomed brand line.
A special feature of Zygom models from Nobel is that they have a patented porous and active TiUnit coating with microgrooves. It ensures rapid implant healing due to the growth of bone cells inside the pores, which form a three-dimensional mesh surface. As a result, the implants are securely connected to the jawbone and practically become one with it.
On the contrary, Biomed zygomatic implants have a smooth surface. There is also an antimicrobial coating. All this significantly reduces the risk of developing peri-implantitis, and also allows you to install implants against the background of an inflammatory process - with periodontitis or periodontal disease.
What implantation and prosthetic techniques are supported by Zygoma zygomatic implants?
Implantation in the cheekbone is relevant when implementing the following techniques:
- “All on six”, when a fixed prosthesis is placed on six artificial pins;
- “All on four”, when a fixed prosthesis is installed on a support in the form of four implant roots;
- Basal implantation program, which involves the introduction of twelve artificial roots. Four of these artificial roots are zygomatic, and they allow you to restore teeth in the absence of teeth.
What could be an alternative?
Zygomatic implantation is used in cases of complete edentia and atrophic processes of the jaw bone as part of protocols with immediate loading. Therefore, only classical implantation with delayed loading or removable prosthetics can be possible alternatives.
Implantation with delayed loading
When choosing an implantation method with delayed loading of a denture in the presence of jawbone atrophy, a bone augmentation procedure is mandatory, otherwise the implants will not be able to be fixed. However, this is not the most successful option, since in the absence of a large number of teeth, such a procedure is extremely difficult to carry out due to the amount of work.
More about the protocol >>>
Removable dental prosthetics
Removable dentures in general can be considered as a method of restoring completely lost teeth. But it is necessary to understand that under the removable structure the process of bone atrophy continues, which over time will lead to sagging of the prosthesis - it will need to be adjusted regularly to avoid rubbing the gums. In addition, removable dentures have insufficiently good fixation in general. The service life of such prostheses is no more than 5-7 years.
Read more about removable dental prosthetics >>>
Basal dental implantation
This method is perhaps the only one that can become a worthy competitor to implantation using classic two-piece zygomatic models. At the same time, it is also more affordable in price. Basal implantation, unlike other methods of immediate loading, involves the use of 8 to 12 implants per dentition, which may also include zygomatic models, but single-piece ones. Due to the increased number of implants, the method has virtually no contraindications based on the condition of the jaw bone and periodontal tissue.
Read more about the basal implantation method >>>
COMPARISON OF IMPLANTATION METHODS WITH DELAYED AND IMMEDIATE LOADING: WHAT IS BETTER FOR COMPLETE EDENTIA?
Comparison of implantation methods with delayed and immediate loading in completely edentulous patients
| Comparison sign for complete edentia | Two-stage implantation with delayed loading | Zygomatic implantation with immediate loading |
| The cost of implantation and prosthetics (in rubles, the price is “turnkey”) | 900,000 for 2 jaws | 450,000 for 1 jaw (all-on-4 protocol, two Zygoma Nobel implants) |
| Duration of treatment | from 2-4 to 18 months | no more than 7 days |
| Number of visits to the doctor | 10-25 | 3-5 |
| Number of hours spent with a doctor | from 7 to 30 hours | to 10 |
| What are the differences between the methods? | ||
| The need to build bone tissue | Performed in 90% of cases, it takes 3-4 months after surgery. recovery | NOT required in 97% of cases, or carried out simultaneously with the installation of implants |
| Removing dental roots | Root removal and implant installation – 2 separate operations | 2 operations are combined |
| Installation of healing abutments | Only after complete implantation (2-4 months) | Not required |
| Installation of abutments | Only after complete implantation (2-4 months) | On the day of implant placement |
| Temporary prosthetics | REMOVABLE temporary butterfly prosthesis | FIXED prosthesis for 1-3 days |
| Permanent prosthetics | Only after complete implantation (2-4 months) | Not required, the service life of the prosthesis is 10 years or more, the warranty on the prosthesis is 5 years |
1 Aparicio, C., Manresa, C., Francisco, K., Ouazzani, W., Claros, P. and Potau, J. M. (2014). The Long-Term Use of Zygomatic Implants:A 10-Year Clinical and Radiographic Report, Clin Implant Dent Relat Res, 16, 3, Oct 18.
3D modeling of the implantation process
When performing zygomatic dental implantation, as a type of immediate loading methods, computer modeling of the treatment process is used. Before surgery, patients undergo computed tomography (CT) - the resulting images allow one to determine the quality and volume of bone tissue, as well as create a virtual model of the jaw on a computer.
One of the key aspects of achieving a high result of zygomatic implantation is careful planning of the entire process and the creation of an anatomically accurate model of the jaw. For this, patients are recommended to undergo not just cone-beam, but multislice computed tomography, which is characterized by higher detail. Especially when it comes to complex clinical cases.
In a special program, the doctor carefully works through the entire implantation process: from installing implants to fixing the prosthesis. Places for implants are selected taking into account the anatomy of the entire jaw system. Surgical templates or stencils are created for each patient - at the stage of implant installation, they allow precise fixation of the structures, without divergence from the virtual plan even by a millimeter.
A special feature of zygomatic implantation at the Smile-at-Once clinic is that in addition to computer modeling, we also cast a real model of the jaw and part of the patient’s face (that is, the jaw and zygomatic bones themselves). It is created on a high-precision 3D printer from soft polymer material. After virtual modeling, the implant surgeon installs analogues of zygomatic implants on a real model, assesses the accuracy of their insertion into the bone and their behavior in tissues. This allows you to take into account all the smallest details, eliminate any inaccuracies and guarantee the patient almost 100% treatment results.
In fact, this is a dummy jaw, which is used for the doctor to perfect the skills of installing implants before their actual implantation, because this process involves working in conditions of very acute, one might even say extreme, bone tissue atrophy.
We are proud to be the first dental center in Russia to use a new generation high-precision 3D printer developed by the Korean company Zenith. Now the time for creating models of the jaw system in our dentistry is only 1 day, and patients receive work done according to the highest standards.
Zygomatic implants: new design and rationale
With long-term adentia, patients note a decrease in the ability to tolerate the chewing function provided by the designs of complete removable dentures due to progressive atrophy of the bone crest of the upper jaw. Tallgren and Cawood described and systematized changes in the maxillofacial region that develop as a result of edentia.
Modern literature describes the successful experience of installing dental implants at an angle in the distal areas of the jaw in order to avoid the need for bone augmentation among patients with complete edentulism, in whom sufficient bone supply is observed only in the frontal areas of the jaw. In cases of severe bone resorption, zygomatic implants can be used as an alternative to support prostheses, which also eliminates the need for bone crest reconstruction. Success rates for zygomatic implants range from 94% to 100%, while Brånemark, Bedrossian, and Aparicio reported cumulative survival rates of 94%, 97.2%, and 97.7%, respectively. When planning the rehabilitation of patients with severe bone tissue atrophy, it is extremely important to ensure a multidisciplinary approach during the implementation of the entire complex of iatrogenic interventions. Assessing bone health using radiographic data is critical and one of the most important steps in planning zygomatic implant treatment. To optimize the algorithm for installing zygomatic implants, Bedrossian and Aparicio proposed systematic approaches that involve dividing the upper jaw into zones and a controlled implantation method based on anatomical features (ZAGA - zygomatic anatomy guided approach). These approaches can be used by surgeons as “road maps” when planning interventions involving the installation of zygomatic intraosseous supports.
Maxillary zones
On an orthopantomogram, the upper jaw can be divided into three zones: zone 1 - premaxillary bone (from canine to canine); zone 2 - premolar area; zone 3 - molar area. With moderate and severe resorption of the upper jaw, as well as with the anterior position of the pneumatized maxillary sinuses, the installation of implants at an angle in zone 2 is limited. Therefore, for patients with sufficient bone supply in zone 1 and bone deficiency in zones 2 and 3, placement of zygomatic implants as distal abutments along with two or four implants in the anterior maxilla is one of the possible rehabilitation options (Figure 1). In cases of almost complete absence of bone supply, as well as in cases of resection of part of the jaw due to various types of tumors, zygomatic implants remain, in fact, the only option for restoring dental status (photo 2).
Photo 1. The use of two zygomatic implants is indicated for bone supply deficiency in zones 2 and 3.
Photo 2. The use of four zygomatic implants is indicated for bone supply deficiency in zones 1, 2 and 3.
Guided approach to the installation of zygomatic implants (ZAGA - zygomatic anatomy guided approach)
In 2011, analyzing frontal sections of tomographic scans, Aparicio described an approach that determines the necessary trajectory for installing zygomatic implants, taking into account the anatomical features of the structure of the bone structures of the maxillofacial region. According to this approach, the doctor in the planning process must take into account the influence of three main factors: the degree of concavity of the lateral wall of the maxillary sinus; the degree of resorption of the maxilla in the palatal direction, and the bone supply in the projection of the zygomatic bone (photo 3). With a ZAGA score in the range of 0–3, zygomatic implants should be stabilized bicortically in the maxillary and zygomatic bone structure; thus, in essence, a fourfold level of support stabilization is provided. With a ZAGA score of level 4, the zygomatic implant needs to be stabilized bicortically only in the zygomatic bone structure.
Photo 3. Classification of clinical conditions according to the Zygomatic Anatomy Guided Approach (ZAGA) concept.
New zygomatic implant design
The experience clinicians have gained with the use of zygomatic implants over the past two decades has provided a better understanding of the biomechanical principles that influence the initial stability of the abutments as well as their long-term support of the final prosthetic structure. Bedrossian et al 2018 described how to prevent and, if necessary, correct complications that can develop with zygomatic implants. Taking into account preventive approaches, new designs of Straumann Zygomatic zygomatic supports were developed: the round ZAGA implant and the flat ZAGA implant. Changes to the original zygomatic implant design include the following characteristics: diameter, surface, thread design, mid-implant modification, apical geometry, and implant platform inclination.
Implant diameter
Patients who have a complete deficiency of bone supply in the upper jaw need to have two implants installed at once in the projection of the zygomatic bone (photo 4). This approach is justified by the so-called “rescue concept,” according to which, if one of the implants fails, the other can continue to function as a support. Considering that it is necessary to install two supports at once, it is preferable that their diameter be reduced. In the updated Straumann Zygomatic implant portfolio, the apical thread starts at 2.6 mm (D2) with a gradual taper towards the implant platform, and ends at 3.9 mm (D4) in front of the smooth mid-portion of the implant. The threads at the ridge level are slightly larger than those in the middle part of the structure at the level of 4.3 mm (D1), which allows for compression of the bone tissue in the area of its contact with the implant surface. The implant platform has a diameter of 4.3 mm and is characterized by the presence of an external hexagonal connection (photo 5). The reduced diameter of the apical part of the Straumann Zygomatic Round and Flat implants will minimize the amount of cancellous substance occupation in the body of the zygomatic bone. In turn, a reduced volume of implant penetration is associated with lower rates of osteocyte apoptosis along osteotomy channels, which also minimizes the effect of remodeling in the osseointegration process.
Photo 4. It is recommended to use implants of narrow diameter in the structure of the zygomatic bone.
Photo 5. Geometry of Zygomatic ZAGA Round (round) and ZAGA Flat (flat) implants.
Surface improvement
Both non-textured and coated implants offer different advantages in relation to their specific application. To achieve an increase in the contact area between the implant and bone surfaces, but at the same time be able to realize the “advantages” of non-rough surfaces, the Straumann Zygomatic design provides a combination of these (photo 5). The rough surface of the implant is localized in its apical part, and it is responsible for improving contact with the surrounding bone tissue and stabilizing the support during the period of osseointegration. The rough part of the surface is located near the platform and interacts well with the surrounding soft tissues. The middle part of Straumann Zygomatic implants is also smooth. The stability of the soft tissues around the implant platform is a key factor in the predicted success, because the risk of developing oroantral anastomosis can be minimized by tightly adapting the surrounding mucosa to the implant platform and the abutment body.
Carving design
The conical shape of the apical part of the Straumann Zygomatic implant allows for compression of the zygomatic bone structures, and thus provides increased stability of the support at the time of installation. To increase stability in the projection of the maxillary ridge, there are additional threads and microthreads of appropriate localization on the surface of the implant (photo 6). Freedman and colleagues in 2013 and 2015 conducted finite element analysis of biomechanical interactions and found that the main support of the zygomatic implant during function is in the area of the screw platform, which is why supporting a certain level of bone tissue around the platform is a critical criterion for the predicted success of rehabilitation .
Photo 6. Microthreads in the projection of the implant platform are designed to provide stability in the area of the bone crest of the jaw.
Modifications to the middle part of the implant
Since the middle part of the implant is located medial or lateral to the lateral wall of the maxillary sinus, where close contact between the surface of the implant and the bone tissue is not expected according to the protocol, this part of the screw is characterized by the absence of any thread.
Apical geometry
The apical part of the Straumann Zygomatic implant is rounded and smooth, which helps to minimize the risk of soft tissue damage if the support is seated too deep in the projection of the zygomatic bone, or in cases where its structure is too thin (photo 7).
Figure 7. Smooth apical geometry minimizes the risk of soft tissue damage.
Platform 55 degrees, abutment with screw fixation, versatility of prosthetic components
Resorption of the edentulous maxilla progresses upward, palatally and posteriorly. Because of this resorption pattern, the zygomatic implant platform is typically located palatally in relation to the dental arch. The 55-degree platform allows you to bring the position of the prosthetic elements closer to the most natural and characteristic of the normal position of the teeth of the upper jaw (photo 8).
Photo 8. 55-degree zygomatic implant platform with screw type fixation.
Two implant designs and a special abutment
The Straumann Zygomatic ZAGA Round implant is used in cases of ZAGA score in the range of 0-3 (photo 6). The emerging threads and microthreads provide stabilization of the implant within the zygomatic bone. In cases of significant concavity of the lateral wall of the maxillary sinus, for example, with a ZAGA score of 4, or in cases of complete or partial maxillectomy, the zygomatic implant will be located outside the maxillary sinus, directly under the soft tissue of the oral vestibule. Under such conditions, there is a possibility of damage to the overlying soft tissues due to muscle strain and physiological mobility of the mucous membrane and skin. To avoid excessive irritation of these tissues, the middle part of the implant is designed flat, which is why the implant is called Straumann Zygomatic ZAGA Flat (photo 9). Partial threading on the palatal surface helps optimize bone contact as the implant platform will overlap the lateral maxilla to some extent.
For Straumann Zygomatic implants, a special zSRA screw-retained abutment has been developed with a height range from 1.5 to 4.5 mm. The abutment is secured to the Straumann Zygomatic external hex connection and tightened to 35 Ncm. The ZSRA can use the same titanium cylinders that are used with existing Straumann Bone Level implants and are suitable for fabrication of a temporary prosthesis with the ability to implement an immediate loading approach (Figure 9).
Photo 9. zSRA abutments with external hex.
Conclusion
Two upgraded Straumann Zygomatic implants improve the quality of dental rehabilitation for patients with moderate to severe forms of maxillary crest bone resorption. To date, the use of these implants is characterized by fairly high rates of clinical success (photos 10-11), however, additional research is necessary to predict the results of the long-term functioning of this type of support.
Photo 10. Postoperative radiograph of a patient rehabilitated with two zygomatic implants.
Photo 11. Postoperative radiograph of a patient rehabilitated with four zygomatic implants.
Authors: Edmond Bedrossian, DDS E. Armand Bedrossian, DDS, MSD
Temporary and permanent prosthetics after zygomatic implantation Zygoma
Installation of the prosthesis will take some time. Either on the day of implantation or within the next week, the patient is given a temporary prosthesis. The design will help remove gaps, allow you to chew food, talk and smile. While the temporary system is in place, optimal load will be placed on the titanium roots, the tissue will regenerate, and the pins will successfully adapt to the bone.
Approximately 6 months after implantation, a permanent ceramic or zirconia prosthesis will be installed, based on the allocated budget.
Possibilities of prosthetics
Zygomatic implantation involves two stages of prosthetics. Immediately after installation of the implants (on days 1-3), a temporary adaptive prosthesis is fixed on a metal frame. The design splints and stabilizes the installed implants, and due to the chewing process it transfers the load to the bone - metabolic processes inside it are activated and the regeneration process is accelerated.
The prosthesis is fixed using special screws that are screwed into the abutments through the tops of the crowns. This allows, if necessary, to remove the structure, as well as to carry out its adjustment taking into account changes in the bite after implantation and rehabilitation of bone tissue.
Depending on the selected materials and the number of implants used (i.e. the treatment protocol itself), the service life of the adaptive prosthesis is five years or more. But in any case, replacement with a more aesthetic and permanent structure can be carried out no earlier than in six months or a year, that is, until the process of osseointegration of the implants is completed.