General overview
The term hygiene index in dental practice is understood as a digital indicator that can be used to evaluate a specific diagnostic criterion for the quality of care for teeth and gums.
In total, there are about 80 different indices that reflect the presence of pathogenic microflora in the oral cavity, the presence of carious cavities, mineralized deposits and other factors indicating the occurrence of pathological processes on the surface of the teeth and gums.
Today, dental indices are divided into 4 large groups, which take into account the following indicators in research:
- plaque area;
- thickness of deposits;
- mass of plaque;
- microbiological, chemical and physical parameters.
Most often, index systems are used in practice, which make it possible to determine the area of damage to the elements of the jaw row by plaque, as well as to determine its thickness.
By clarifying these points, the dentist performs a quantitative assessment of the following indicators:
- the degree of destruction of the elements of the jaw arch;
- the ratio of the number of healthy teeth to those that are damaged and cannot be restored, or have been removed;
- stage of damage to hard and soft tissues;
- the effectiveness of the implemented therapeutic measures.
RNR
Six teeth are coated with a dye that allows plaque to be found. To indicate the total number, you need to determine the number for each surface by summing the code values of individual areas. Then these values are added up and divided by how many teeth a person has in total.
The bite is assessed by the dental aesthetic index. It characterizes the health of the bite, dental location in the sagittal, vertical and transversal directions.
Important! Assessment begins at age twelve.
An external examination using a button probe is used.
An aesthetic assessment characterizes each component of the index and allows them to be arranged according to various pathologies of the rows of teeth and occlusion.
The score is expressed as a percentage. The number of people who were diagnosed with caries is divided by the total number of participants in the control group, and then the resulting number is multiplied by 100.
Classification and types of CPU
One of the most popular in dental practice is the KPU index - an indicator that reflects the intensity of the carious process.
It involves determining the following parameters:
- K – number of carious lesions;
- P – number of installed seals;
- Y is the number of removed elements of the series.
The total value of these indicators allows the dentist to draw conclusions about the dynamics of the caries process in the patient’s mouth.
There are three types of CPU, which carry important information about the state of the permanent elements of the human jaw row:
- KPU of teeth is a quantitative indicator of the damage to a number of elements by caries and the presence of fillings in them;
- KPU of surfaces - the number of hard tissue surfaces damaged by the carious process;
- The number of cavities is the number of holes formed in the tooth surface as a result of caries.
When assessing carious lesions in primary teeth, two indicators are used: K - the number of elements of the row affected by the disease and P - the number of units on which fillings are installed. Removed and fallen incisors are not taken into account.
In the case of a mixed dentition, it is customary to calculate and summarize both indicators - KPU and KP, which allows for an accurate assessment of the condition of the child’s oral cavity.
KPI
CPI is a comprehensive periodontal index. You can start research from adolescence, analyzing the condition of teeth 17/16, 11, 26/27, 31, 36/37, 46/47.
For a full analysis, you need to provide high-quality lighting with lamps. Use the same equipment as usual.
Important! Some pathologies suggest serious injuries.
If the doctor is in doubt, it is necessary to conduct electroodontodiagnosis.
Evaluation of indicators
There are three main directions for assessing caries lesion indicators;
- Extent of caries spread. This indicator is the percentage of the number of patients diagnosed with caries to the total number of people examined.
This technique is often used to compare oral health status in different regions of the country.
The levels of caries prevalence among 12-year-old patients are used as assessment criteria: a low level corresponds to an indicator from 0 to 30%, an average level from 31 to 80%, and a high level from 81 to 100%.
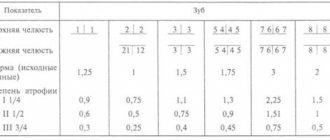
- The intensity of spread is an indicator that determines the degree of caries damage to the elements of the jaw row of a particular patient. For children under 12 years of age, the following assessment criteria apply:
- very low intensity – up to 1.1;
- low – up to 2.6;
- moderate – from 2.7 to 4.4;
- high – from 4.5 to 6.5;
- very high – more than 6.5.
For adults, this breakdown changes slightly and looks like this:
- very low – up to 1.5;
- low – from 1.6 to 6.2;
- moderate – from 6.2 to 12.7;
- high – 12.8-16.2;
- very high – more than 16.2.
- Increase in caries infection. This indicator allows you to assess the dynamics of the development of the carious process in an individual patient.
To determine it, the intensity of caries over a certain period of time is revealed.A change in the value of the indicator up or down indicates the effectiveness or ineffectiveness of the therapeutic process.
Components of the Opalescence home teeth whitening system and how it works.
Come here to find out if dental teeth whitening is harmful.
At this address https://zubovv.ru/krasota-i-uxod/otbelivanie/domashnee/limonom-i-kak.html we offer several effective recipes for teeth whitening with lemon.
Gingivitis index PMA (Schour, Massler) modified by Parma
Gingivitis index PMA (Schour, Massler) as modified by Parma (determination of risk factors) - papillary-marginal-alveolar index is calculated by adding the assessments of the gum condition of each tooth in % using the formula:
RMA = sum of indicators x 100%
3 x number of teeth
0 - no inflammation,
1 - inflammation of the interdental papilla (P)
2 - inflammation of the marginal gum (M)
3 - inflammation of the alveolar gum (A)
At the age of 6-7 years, the number of teeth is normally 24, at 12-14 years - 28, and at 15 years and older - 28 or 30.
The PMA index is very sensitive to the slightest changes in the clinical picture, and its value can be influenced by random influences.
Flaws
Despite the high information content, indicators of the intensity of the carious process in the oral cavity also have disadvantages.
The most significant of them are the following points:
- impossibility of accounting for caries at the stage of white spots and initial pigmentation;
- inaccurate results when new cavities form on treated units;
- unreliability of calculations when previously installed seals fall out.
These features affect the outcome of assessing the patient’s oral cavity, often leading to the formulation of incorrect conclusions.
Popular methods
There are many different methods for determining the health and oral hygiene of a patient.
They are aimed at identifying various indicators and can be used both separately and in combination.
Fedorova-Volodkina
Calculation of the hygienic index involves applying an iodide solution to the incisors of the lower jaw from the side of the labial plane, followed by assessing the saturation of its manifestation on the enamel and identifying Ki - the cleaning index of one unit.
Ki is determined separately for all six processed units and has the following criteria:
- with complete absence of staining - 1 point;
- if paint develops on the fourth part of the cutter - 2 points;
- if half the surface of the element is pigmented – 3 points;
- if coloring is detected on ¾ of the part - 4 points;
- with a complete change in the color of the front side - 5 points.
Next, the Fedorov-Volodkina hygiene index (Ksr) is calculated using the following formula:
in this formula is the total indicator of the purification indices of all elements treated with the coloring composition, and the number 6 means the number of elements being evaluated.
The evaluation of the calculation results is carried out as follows:
Indicator value
Characteristics of the degree of teeth cleaning
Green Vermilion
Green's Vermilion Hygienic Index (OHI-S) helps determine the degree of bacterial deposits and tartar coverage on the tooth surface.
The study is carried out as follows:
- Using special instruments or a staining agent, the state of cleanliness of certain units is assessed.
This is the surface of the first upper molars on the buccal side, the first lower molars on the lingual side, and the labial plane of the maxillary anterior incisors. Each of the elements is studied for the presence of two components - plaque and mineralized deposits.
- no deposits – 0;
- plaque on 1/3 of a tooth – 1;
- plaque on 2/3 of the surface – 2;
- accumulations located on an area of more than 2/3 of the tooth – 3.
The amount of stone found on the teeth examined is estimated in a similar way:
- no deposits – 0 points;
- supragingival stone on 1/3 of the plane – 1 point;
- supragingival mineralized plaque on 2/3 parts – 2 points;
- stone in the cervical part and above the gum in an area of more than 2/3 of the element - 3 points.
- The Green Vermilion index is calculated:
The assessment of the hygienic index is carried out taking into account the following accepted values:
OHI-S value
Assessing the quality of hygiene procedures
Silnes Low
To calculate the Silnes-Lowe index, the thickness of bacterial deposits on four surfaces of the tooth is determined - distal, mesial, labial and lingual.
This is done using a suitable probe on pre-dried enamel. Depending on the clinical situation, both all elements of the jaw arch and individual elements can be analyzed.
Each surface examined is assigned a certain number of points:
- with complete absence of plaque – 0;
- if a thin layer is detected after exposure to the probe - 1;
- in the presence of a thin or moderate layer of plaque that is clearly visualized – 2;
- with intense deposits in the area of the interdental space and gingival sulcus - 3.
The hygiene score for one unit is determined as the sum of the surface scores divided by the number of surfaces. To calculate the Silnes-Low index for the entire oral cavity, the average value is calculated for all examined elements.
This index allows us to evaluate the presence of subgingival and supragingival tartar on all four surfaces of the lower incisors and canines.
Each plane is graded on the following scale:
- no stone – 0 points;
- stone volume is less than 0.5 mm – 1 point;
- the width of the stone ranges from 0.6 to 1 mm – 2 points;
- stone thickness exceeds 1 mm – 3 points.
Calculation of the overall tartar spread intensity index CSI is carried out as the ratio of the total number of points of all examined surfaces to the number of analyzed units.
Quigley and Hein
The Quigley-Hein index allows you to estimate the area of elements covered with bacterial plaque. To do this, the vestibular surface of the organs of both jaws included in the smile zone is examined, onto which a solution of a coloring substance - fuchsin - is applied.
After the plaques acquire a rich crimson color, points are awarded:
- for lack of pigmentation – 0;
- in the presence of minor areas in the cervical region - 1;
- when painting in the form of strips up to 1 mm wide – 2;
- change in color of areas up to 1/3 of the part – 3;
- coating from 1/3 to 2/3 of the surface – 4;
- spread of plaque over an area of more than 2/3 of the part – 5.
To calculate the Quigley-Hein plaque index, the ratio of the sum obtained as a result of the assessment of points to the number of examined units is calculated - 12.
Check out the list of the most harmful foods for teeth and read about their destructive power.
In this post you will find fair reviews of teeth whitening pencils.
Here https://zubovv.ru/krasota-i-uxod/otbelivanie/domashnee/10-sposobov-sodoy-i-otzyivyi.html evaluate the result of teeth whitening with soda based on reviews from patients and specialists.
Lange API
The index allows you to identify the intensity of deposit formation on the proximal surfaces of the elements of the jaw arch, which are pre-coated with a liquid that gives the plaque a certain shade.
After this, the lingual sides of the first and third quadrants of the jaws, as well as the labial sides of the second and fourth quadrants, are carefully examined for the presence of stained plaques.
The presence of plaque is determined using the answers “Yes” and “No”.
The API index is calculated as follows:
Assessment of the quality of oral hygiene according to the index is carried out according to the following criteria:
- API less than 25% - optimal hygiene quality;
- API from 26% to 40% - a sufficient degree of hygiene;
- API from 41% to 70% - satisfactory state of cleanliness of the oral cavity;
- API over 71% is an unsatisfactory level of dental and gum hygiene.
Ramfiord
The Ramfiord periodontal index involves the study of the following elements:
- on the upper jaw – 11, 14 and 26;
- on the bottom – 31, 34, 36.
The palatal, lingual and vestibular planes are analyzed, pre-treated with Bismarck's solution, due to which the plaque turns brownish.
Assessment of the condition of row elements is carried out using the following criteria:
Number of points
Characteristic
No bacterial layer
Deposits on all planes exceed half of the total tooth area
The method is based on the study of the labial surface of the central incisors, pre-treated with a fuchsin solution.
The result is analyzed as follows:
- absence of plaque – 0;
- slight staining of the plaque in the area of the border with the gum – 1;
- clear line of plaque staining at the gingival border – 2;
- coating with deposits up to 1/3 part – 3;
- spread of plaques on 2/3 of the vestibular surface of the incisor – 4;
- plaque exceeds 2/3 of the area – 5.
The general index is the arithmetic mean of the condition indicators of the tested teeth.
Tureski
The methodology for determining the intensity of plaque and assessing the results of the study is similar to Quigley and Hein.
The difference lies in the plane of examination - this method involves examining both the vestibular and lingual edges of the frontal elements of the jaw row.
The scoring method is as follows:
- complete absence of plaque – 0;
- small areas in the cervical region – 1;
- deposits up to 1 mm in area – 2;
- plaque area more than 1 mm, but less than a third of the tooth – 3;
- Plaque covering up to 2/3 of the tooth – 4;
- staining area over 2/3 of the tooth surface – 5.
To calculate the Turesky index, the sum of the points obtained is divided by the number of units inspected.
Arnim
The Arnim method for determining the area of plaque spread is very accurate, although quite labor-intensive. It consists of performing the following actions:
- the central and lateral incisors of both jaws are coated with an erythrosine solution from the vestibular side;
- photographs of the processed elements of the row are taken, after which they are enlarged and printed;
- the contours of the studied units with colored areas are transferred to paper;
- Using a special device - a planimeter, the percentage of the colored area of the tooth surface is calculated.
PFRI Axelsson
The purpose of this index is to identify the conditions and factors that influence the rate of plaque formation on enamel. This is defined as follows:
- The patient undergoes professional cleaning of deposits in a dental office, after which he should not perform oral hygiene for 24 hours.
- After the specified time, the elements are stained with a special solution , which makes it possible to detect the presence of bacterial plaque.
- The condition of the units is assessed , the number of surfaces affected by plaques is identified, and their percentage to the total number of examined planes is calculated.
The result is assessed according to the following scale:
Proportion of surfaces contaminated with plaque
Deposit rate
Fedorov-Volodkina Index
(1968) was widely used in our country until recently.
The hygienic index is determined by the intensity of coloring of the labial surface of the six lower frontal teeth with an iodine-iodide-potassium solution, assessed using a five-point system and calculated using the formula:
,
where K avg
.
– general hygienic cleaning index; K u
– hygienic index of cleaning one tooth;
n
– number of teeth.
Staining the entire surface of the crown means 5 points; 3/4 – 4 points; 1/2 – 3 points; 1/4 – 2 points; absence of staining – 1 point.
Normally, the hygiene index should not exceed 1.
Green-Vermillion index
(Green, Vermillion, 1964)
.
The Oral Health Index Simplified (OHI-S) evaluates the area of tooth surface covered by plaque and/or tartar and does not require the use of special stains. To determine OHI-S, examine the buccal surface 16 and 26, the labial surface 11 and 31, and the lingual surface 36 and 46, moving the tip of the probe from the cutting edge towards the gum.
The absence of dental plaque is indicated as, dental plaque up to 1/3 of the tooth surface - 1
, dental plaque from 1/3 to 2/3 –
2
, dental plaque covers more than 2/3 of the enamel surface –
3
. Then tartar is determined according to the same principle.
Formula for calculating the index.
where n
– number of teeth,
ZN
– dental plaque,
ZK
– tartar.
supragingival stone on 1/3 of the crown
supragingival stone on 2/3 of the crown
supragingival calculus > 2/3 of the crown or subgingival calculus surrounding the cervical portion of the tooth
Index Score
Oral hygiene assessment
Silnes-Lowe Index
(Silness, Loe, 1967) takes into account the thickness of plaque in the gingival region in 4 areas of the tooth surface: vestibular, lingual, distal and mesial.
After drying the enamel, the tip of the probe is passed along its surface at the gingival sulcus. If no soft substance adheres to the tip of the probe, the plaque index on the tooth area is indicated as -. If the plaque is not visually detected, but becomes visible after moving the probe, the index is equal to 1
.
The plaque is thin to moderately thick and visible to the naked eye with a score of 2
.
Intensive deposition of plaque in the area of the gingival sulcus and interdental space is designated as 3
. For each tooth, the index is calculated by dividing the sum of the points of 4 surfaces by 4.
The general index is equal to the sum of the indicators of all examined teeth, divided by their number.
Calculus Index (CSI)
(ENNEVER' et al., 1961). Supra- and subgingival tartar is determined on the incisors and canines of the lower jaw. The vestibular, distal-lingual, central-lingual and medial-lingual surfaces are examined differentially.
To determine the intensity of tartar, a scale from 0 to 3 is used for each surface examined:
0 - no tartar
1 – tartar is determined to be less than 0.5mm in width and/or thickness
2 - width and/or thickness of tartar from 0.5 to 1 mm
3 - width and/or thickness of tartar more than 1 mm.
Formula for calculating the index:
Ramfjord index
(S. Ramfjord, 1956) as part of the periodontal index involves the determination of dental plaque on the vestibular, lingual and palatal surfaces, as well as the proximal surfaces of the 11, 14, 26, 31, 34, 46 teeth. The method requires preliminary staining with a Bismarck brown solution. Scoring is done as follows:
0 - absence of dental plaque
1 - dental plaque is present on some tooth surfaces
2 - dental plaque is present on all surfaces, but covers more than half of the tooth
3 - dental plaque is present on all surfaces, but covers more than half.
The index is calculated by dividing the total score by the number of teeth examined.
Navi index (IMNavy, E. Quiglty, I. Hein, 1962).
The color indices of tissues in the oral cavity limited by the labial surfaces of the front teeth are calculated. Before the examination, the mouth is rinsed with a 0.75% solution of basic fuchsin. The calculation is carried out as follows:
0—no plaque
1 - the plaque was stained only at the gingival border
2 - pronounced plaque line at the gingival border
3 - the gingival third of the surface is covered with plaque
4 - 2/3 of the surface is covered with plaque
5 - more than 2/3 of the surface is covered with plaque.
The index was calculated in terms of the average number per tooth per subject.
Turesky index (S.Turesky, 1970).
The authors used the Quigley-Hein scoring system on the labial and lingual surfaces of the entire row of teeth.
0—no plaque
1 - individual spots of plaque in the cervical area of the tooth
2 - thin continuous strip of plaque (up to 1 mm) in the cervical part of the tooth
3 - plaque strip is wider than 1 mm, but covers less than 1/3 of the tooth crown
4 - plaque covers more than 1/3, but less than 2/3 of the tooth crown
5 - plaque covers 2/3 of the tooth crown or more.
Index Arnim (S. Arnim, 1963)
in assessing the effectiveness of various oral hygiene procedures, determined the amount of plaque present on the labial surfaces of four upper and lower incisors stained with erythrosine. This area is photographed and developed at 4x magnification. The outlines of the corresponding teeth and colored masses are transferred to paper and these areas are determined with a planimer. The percentage of surface area covered by plaque is then calculated.
Hygiene Performance Index (Podshadley, Haby, 1968)
requires the use of dye.
Then a visual assessment of the buccal surfaces of 16 and 26 teeth, labial surfaces of 11 and 31 teeth, and lingual surfaces of 36 and 46 teeth is carried out. The examined surface is conventionally divided into 5 sections: 1
– medial,
2
– distal,
3
– mid-occlusal,
4
– central,
5
– mid-cervical.
0 - no staining
1 - there is staining of any intensity
The index is calculated using the formula:
G
den is the number of teeth examined.
Oral hygiene is one of the most accessible and at the same time one of the leading methods of preventing oral diseases. Regular and competent oral care is an integral part of all preventive measures. Mass population surveys conducted in all countries of the world have convincingly shown that systematic oral care has an undoubted preventive value. It is possible to objectively assess the level of oral hygiene only using hygiene indices.
To identify dental plaque in assessing oral hygiene in modern dentistry, objective indicators (indices) are used that characterize the quality and quantity of dental plaque. However, the number of assessment methods, which are based on different numbers of teeth from different functional groups, up to staining all teeth on both sides or collecting and weighing plaque around individual teeth, indicates the relevance of the problem under consideration and the imperfection of existing methods.
Cliche
The calculation formula is attached as follows:
IGR-u = sum of plaque values/number of planes + sum of stone values/number of surfaces.
The interpretation of the index (the IGR value at the level of medicine) is proposed as follows:
- 0.0-1.2 - flawless;
- 1.3-3.0 – acceptable;
- 3.1-6.0 – low.
The Green-Vermilion index has the following values for dental plaque standards:
- 0.0-0.6 – impeccable;
- 0.7-1.8 – tolerable;
- 1.9-3.0 – bad.
Oral hygiene indices.
Method for determining the Fedorov-Volodkina hygienic index // E.M. Melnichenko “Prevention of dental diseases”, Minsk, “Higher School”., 1990, pp. 3-17.
It is determined by the intensity of the color of the vestibular surface of the six lower frontal teeth by applying an iodine-iodide-potassium solution (Schiller-Pisarev liquid).
The calculation is carried out according to the formula:
Ksr (hygiene index) = Kn (total hygiene index for each of the six teeth) / n (number of teeth).
Coloring the entire surface of the crown is scored 5 points, 3/4 of the surface - 4, 1/2 of the surface - 3, 1/4 of the surface - 2 points. If there is no staining, 1 point is given. The indicator is assessed as follows: good index, satisfactory, unsatisfactory, bad, very bad.
However, the proposed method has a number of disadvantages:
— determination of the quality and quantity of dental plaque, assessment of the hygiene index was carried out only on one’s own teeth; — the use of known dyes is impossible when determining the amount of dental plaque on bridges, since these solutions are difficult to wash off from the surface of the dentures.
1. Fedorov-Volodkina index
3.5-5.0 - very bad
The vestibular surface of the six front teeth of the lower jaw - incisors and canines - is stained with Lugol's solution. Rating on a 5-point system:
5 points – the entire surface of the teeth is stained,
4 points – 3/4 of the tooth surface,
3 points - 1/2 of the tooth surface,
2 points - 1/4 of the tooth surface,
1 point - no staining
Then find the arithmetic mean by dividing the sum of the color of all teeth by their number: K av = Kp: p.
Good level of hygiene: Ksr=1.0-1.3 b
IG = sum of points of six teeth 6.
2. Green-Vermilion Index (1964) - universal hygiene index of the UIG
Schiller-Pisarev solution or Lugol's solution
Determine the presence of plaque and tartar on the buccal surface of the first upper molars, the lingual surface of the lower molars, and the vestibular surface 1| and lower |1
6 1| 6 6 | 1 6. On all surfaces, plaque is first determined, then tartar.
0 - no plaque (stone)
1 - plaque covers up to 1/3 of the tooth surface
2 - plaque covers from 1/3 to 2/3 of the tooth surface
3 – plaque covers more than 2/3 of the tooth surface
Tartar assessment:
0 – absence of tartar
1 – supragingival tartar covers no more than 1/3 of the tooth crown
2 – supragingival tartar covers from 1/3 to 2/3 of the tooth crown, or single formations of subgingival tartar are detected
3 – supragingival tartar covers more than 2/3 of the tooth crown, or significant deposits of subgingival tartar are detected along the entire circumference of the tooth.
SPI = sum of indicators of 6 teeth 6
The assessment of the tartar index is carried out similarly to UIG = IZN + IZK
1- staining up to 1/3 of the crown,
2- staining up to 2/3 of the crown
3- more than 2/3 of the tooth crown
Staining of the vestibular and lingual surfaces
The plaque index and stone index are summed up and the average is obtained.
RHP Index – Oral Hygiene Performance Index (Podshadley, Haley – 1968)
Color 6 teeth:
16, 26, 11, 31 – vestibular surfaces.
36, 46 – lingual surfaces
The examined surface is divided into 5 sections: 1-medial, 2-distal, 3-mid-occlusal, 4-central, 5-mid-cervical.
Plaque is assessed at each site:
0 – no staining
1 – staining detected
For each tooth, the site codes are summed up. Then the values of all examined teeth are summed up and the resulting sum is divided by the number of teeth.
1.7 or more - unsatisfactory
Index of need for periodontal disease treatment - CPITN
To assess the prevalence and intensity of periodontal diseases, almost all countries use the index of need for the treatment of periodontal diseases - CPITN . This index was proposed by specialists of the WHO working group to assess the condition of periodontal tissues during epidemiological surveys of the population.
Currently, the scope of the index has expanded, and it is used to plan and evaluate the effectiveness of prevention programs, as well as calculate the required number of dental personnel. In addition, the CPITN index is currently used in clinical practice to examine and monitor the periodontal condition of individual patients.
In this regard, the CPITN index can be considered a screening test at both the population and individual levels.
This index registers only those clinical signs that may undergo reverse development: inflammatory changes in the gums, which are judged by bleeding, tartar. The index does not record irreversible changes (gingival recession, tooth mobility, loss of epithelial attachment), does not indicate the activity of the process and cannot be used to plan specific clinical treatment in patients with developed periodontitis.
The main advantages of the CPITN index are the simplicity and speed of its determination, information content and the ability to compare results.
To determine the CPITN index, the dentition is conventionally divided into 6 parts (sextants), including the following teeth: 17/16, 11, 26/27, 36/37, 31, 46/47.
The periodontium is examined in each sextant, and for epidemiological purposes only in the area of the so-called “index” teeth. When using the index for clinical practice, the periodontium is examined in the area of all teeth and the most severe lesion is identified.
It should be remembered that a sextant is examined if it contains two or more teeth that cannot be removed. If only one tooth remains in the sextant, it is included in the adjacent sextant, and this sextant is excluded from the examination.
In the adult population, starting from 20 years of age and older, 10 index teeth are examined, which are identified as the most informative:
When examining each pair of molars, only one code characterizing the worst condition is taken into account and recorded.
For persons under 20 years of age, 6 index teeth are examined during the epidemiological survey: 16, 11, 26, 36, 31, 46.
CODE 1: bleeding observed during or after probing.
Note: bleeding may appear immediately or after 10-30 seconds. after probing.
CODE 2: tartar or other plaque-retaining factors (overhanging edges of fillings, etc.) are visible or felt during probing.
CODE 3: pathological pocket 4 or 5 mm (the edge of the gum is in the black area of the probe or the 3.5 mm mark is hidden).
CODE 4: pathological pocket 6 mm deep or more (with the 5.5 mm mark or black area of the probe hidden in the pocket).
CODE X: When only one or no teeth are present in the sextant (third molars are excluded unless they are in place of second molars).
To determine the need for periodontal disease treatment, population groups or individual patients can be categorized based on the following criteria.
0: CODE 0 (healthy) or X (excluded) for all 6 sextants means that there is no need for treatment for this patient.
1: A CODE of 1 or higher indicates that this patient needs to improve his oral hygiene status.
2: a) CODE 2 or higher indicates the need for professional hygiene and the elimination of factors that contribute to plaque retention. In addition, the patient needs training in oral hygiene.
b) CODE 3 indicates the need for oral hygiene and curettage, which usually reduces inflammation and reduces pocket depth to values equal to or less than 3 mm.
3: Sextant with CODE 4 can sometimes be successfully treated with deep curettage and adequate oral hygiene. In other cases, this treatment does not help, and then complex treatment is required, which includes deep curettage.
The prevalence and intensity of periodontal disease in the population is assessed based on the results of a survey of 15-year-old adolescents.
Prevalence of signs of periodontal damage (adolescents 15 years old)
Prevalence Bleeding gums Tartar
low 0 – 50% 0 – 20%
average 51 – 80% 21 – 50%
high 81 – 100% 51 – 100%
Level of intensity of signs of periodontal damage (adolescents 15 years old)
INTENSITY LEVEL BLEEDING GUMS CALCULUS
LOW 0.0 - 0.5 sextants 0.0 - 1.5 sextants
AVERAGE 0.6 - 1.5 sextants 1.6 - 2.5 sextants
HIGH < 1.6 sextants < 2.6 sextants