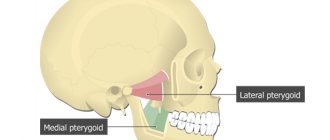
Benign tumors of the pharynx, which include a cyst on the tonsil, are quite common, especially in people with chronic tonsillitis and adenoids. Such neoplasms are most often benign in nature. But, despite this, experts recommend using predominantly surgical treatment, since excessive tissue growth can at any time lead to malignancy of cells. In addition, cysts on the tonsils create obstacles to swallowing and breathing, often cause exacerbation of chronic ENT pathologies and reduce a person’s quality of life.
Tonsils are a filter for pathogenic microorganisms and perform a protective function. But with excessive tissue growth, they turn into a source of chronic infection. Cysts on the tonsils are treated mainly surgically, since conservative therapy is ineffective.
At the CONSTANTA Clinic in Yaroslavl, tonsils and cysts are removed by experienced otolaryngologists using modern endoscopic equipment. Endoscopy in otolaryngology is the gold standard of surgical treatment, which is characterized by minimal trauma and maximum efficiency. We provide our patients with qualified services and assistance from wide-ranging ENT specialists.
Why do cysts appear on the tonsils?
Only a qualified specialist can indicate the exact cause of the appearance of a cyst on the tonsil, using examination data and a comprehensive examination. Chronic infectious and inflammatory processes in the oropharynx come first in this disease. If the patient suffers from diseases such as tonsillitis, sinusitis, laryngitis, in which there is pronounced swelling of the mucous membrane in the mouth and nose, then favorable conditions are created for tissue proliferation and the growth of pathological neoplasms.
But there are other reasons that lead to the growth of cysts on the tonsils:
- changes in hormonal levels;
- weakening of the body's defenses;
- bad habits (smoking, drinking alcohol);
- tonsil injuries;
- work in hazardous industries associated with inhalation of polluted air poisoned by chemical vapors;
- sluggish inflammatory process in the oropharynx;
- development of autoimmune pathologies;
- untreated tonsillitis.
How does the disease progress?
A cyst on the tonsils does not bother the patient for a long time. But as it grows, it begins to compress the surrounding soft tissues and can cause breathing problems, even asphyxia. Therefore, it is so important to contact specialists in a timely manner and carry out scheduled preventive examinations, especially in the presence of chronic ENT diseases.
Patients with cysts in the tonsil area present the following complaints:
- decreased quality of nasal breathing;
- feeling of a lump in the throat;
- pain and discomfort when swallowing food;
- sore throat;
- hoarseness of voice;
- frequent exacerbations of chronic diseases of the ENT organs and respiratory tract.
If you often suffer from respiratory viral diseases, tonsillitis, laryngitis, you need to consult a specialist who will conduct an examination using innovative equipment that allows you to examine the tissues of the hypopharynx with maximum efficiency. Based on the diagnostic data, the doctor makes a diagnosis and prescribes treatment.
If the tumor is often injured by rough food, it may begin to bleed. As a result, the patient will detect traces of blood in the saliva. This is an alarming sign that requires immediate consultation with a specialist. Cysts on the tonsils also occur in childhood. The child begins to complain of discomfort when swallowing saliva, sore throat on one side, and a change in voice. Often children begin to chew food poorly, clear their throats and are afraid of short-term breath holding.
If the tonsil cyst is small and not prone to active growth, a wait-and-see approach can be used. But when the tumor rapidly increases in size, it is necessary to undergo surgery as soon as possible.
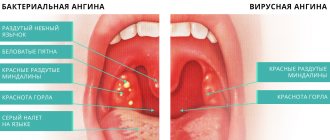
Signs and symptoms of purulent sore throat in a small child
The appearance of the first signs of purulent tonsillitis occurs very quickly. The time between infection and the onset of symptoms ranges from several hours to several days.
The first to appear are several signs that relate to the typical symptoms of tonsillitis: the occurrence of severe pain in the throat, a sharp increase in temperature to the highest levels (up to 40℃), the occurrence of chills, and enlargement of the cervical lymph nodes. A sharp manifestation of the “high temperature” symptom can cause seizures.
The baby's behavior changes dramatically. He becomes lethargic, moody, and loses his appetite. The child complains of headaches and aching joints. The development of purulent tonsillitis can be the cause of a reaction from the gastrointestinal tract: the occurrence of nausea and vomiting during this period is not uncommon. All these symptoms are signs of intoxication of the body
A typical pathological symptom of purulent tonsillitis is purulent plaque on the surface of the palatine tonsils.
The occurrence of these symptoms is a good reason to urgently show the baby to an ENT doctor in order to treat him quickly, effectively and avoid dangerous consequences for the little body.
Complications of tonsil cysts
A cyst on the tonsil is a chronic source of infection that can behave in an unknown way, causing various complications. The neoplasm in the pharynx is constantly rubbed with food, which leads to the formation of a chronic inflammatory process. The longer the patient does not seek medical help, the longer the infection progresses; along with the bloodstream, infectious pathogens are carried to all cells and organs, disrupting their normal functioning.
A long-term infectious process is accompanied by general intoxication of the body. Toxins produced during the activity of pathogenic microorganisms disrupt the functioning of the liver and kidneys, provoke the development of chronic fatigue syndrome, reduce immunity and make a person vulnerable to even the most harmless infections.
Only an otolaryngologist can choose the treatment for a cyst on the tonsils, based on the results of pharyngoscopy. If the doctor suspects the development of a malignant process, a consultation with an oncologist will be required. Other studies may also be prescribed: rhinoscopy, audiometry, computed tomography and magnetic resonance imaging of the brain, otoscopy. In advanced cases, the tumor can grow into nearby tissues, including brain structures.
Treatment of tonsil cysts
Treatment of cysts can be either conservative or surgical. Often, specialists first prescribe effective drug therapy to relieve inflammation and prepare the patient for surgery. Conservative treatment of a cyst will not reduce its size, but can stop the active growth of the tumor and prevent complications. Treatment tactics should be selected by a competent specialist based on medical history, diagnosis and professional examination.
Conservative therapy for tonsil cysts includes the following measures and procedures:
- gargling with herbal decoctions, antiseptic solutions that disinfect tissues and have an anti-edematous and anti-inflammatory effect;
- physiotherapy: ultraviolet irradiation, massage, ultrasound - physiotherapeutic treatment methods are used to increase blood supply to tissues in the area where the tumor is located, to ensure lymph outflow;
- pumping out pus using hardware methods, which makes it possible to stop the development of the infectious process and the spread of infection to surrounding tissues;
- injection rinsing of the tonsils with anti-inflammatory drugs and antiseptics to cleanse plaque and purulent contents;
- strengthening the immune system with multivitamin complexes and immunostimulants;
- giving up bad habits that contribute to traumatization of the tonsils and the preservation of the chronic inflammatory process.
Some specialists practice opening the cyst and pumping out its contents. But, as a rule, the therapeutic effect does not last long and the tumor is filled with fluid again. Therefore, if the cyst has not disappeared after several weeks of active medical therapy, it is better to remove it surgically.
Drug treatment, do you need an antibiotic?
Treatment of tonsillitis in a child should be comprehensive!
To treat tonsillitis in a child, the following groups of medications are used:
- Antiseptics. These include special solutions for rinsing and treating the inflammatory focus, as well as various aerosols for irrigating the oropharynx: Hexasprey, Miramistin, Tantum Verde, Hexoral, Cameton.
- Antihistamines. These drugs are used to relieve swelling of the tonsils and pharyngeal mucosa. The best drugs in this group are considered to be the latest generation of drugs that do not have sedative properties: Cetrin, Suprastin, Telfast.
- Analgesics. Used for acute pain when swallowing and sore throat.
- Immunomodulatory drugs. For children from this group of drugs, it is advisable to use natural-based immunomodulators.
- Antipyretics. They are used in case of high temperature in a child - more than 38 degrees. Children are usually prescribed Paracetamol or Nurofen.
In addition, the otolaryngologist can prescribe physiotherapeutic procedures for tonsillitis. For example, in the chronic form, it is recommended to undergo laser treatment twice a year. Specialists often prescribe ultraviolet irradiation, climatotherapy, and aromatherapy.
One of the frequently asked questions by parents is: “Do I need to take antibiotics for tonsillitis?” Otolaryngologists necessarily prescribe antibacterial drugs for exacerbation of the chronic form of the disease, as well as for acute tonsillitis, the causative agent of which is pathogenic bacteria.
Useful video - How and when to remove tonsils:
The best syrup for dry and wet coughs for children under one year old
Children are usually prescribed drugs of the penicillin, macrolide and cephalosporin group. Such antibiotics for the treatment of tonsillitis include Sumamed, Augmentin, Flemoklav Solutab, Clarithromycin, Azithromycin, Cefadroxil.
To prevent the development of dysbiosis during antibiotic treatment, probiotics are used, for example Linex, Laktovit, Hilak Forte.
It is important to remember that such drugs are prescribed by an experienced otolaryngologist. Parents, in order to avoid aggravating the problem, as well as not to harm their child, are not allowed to independently select medicine and treat the patient with it. The choice of antibiotic is made taking into account the individual characteristics of the child’s body, the form and severity of the disease, and it also depends on the pathogen that provoked the development of the disease.
- Why do joints hurt after a sore throat - complications in acute and chronic tonsillitis
Gargling and inhalation
At elevated body temperatures, inhalation is prohibited!
The complex treatment of tonsillitis in children also includes a rinsing procedure. It is done using medicinal solutions such as Furacilin, Miramistin, Iodinol. It is recommended for young children to treat their tonsils with a gauze swab, since they do not yet know how to gargle properly.
The rinsing procedure can be done with saline solution. The finished drug can be purchased at pharmacies. At home, you can prepare it by dissolving a teaspoon of salt, preferably sea salt, with boiling, cooled water. You can rinse the oropharynx with a solution with the addition of essential oils or infusions of medicinal herbs, for example, calendula, chamomile, marshmallow, sage, St. John's wort. You can treat the disease by gargling with beet juice.
Inhalations are considered an effective method of treatment for tonsillitis.
It is better for children to do them using a special device that can be purchased at pharmaceutical institutions. This device is called a nebulizer.
Inhalations are carried out using various medicinal solutions. Procedures using herbal decoctions are also considered safe and effective for children. For these inhalations, you can use the following plants, which have bactericidal, anti-inflammatory and analgesic properties:
- Sage
- Eucalyptus
- Calendula
- Pine needles
- Oak bark
- Coltsfoot
- Chamomile
It is useful to perform inhalations using aromatic oils. For tonsillitis, mint, peach, eucalyptus, rose and sage oils are considered effective.
Surgeries for tonsil cysts
The smaller the size of the cyst, the easier it is to perform surgical treatment. Small neoplasms with a thin wall are usually opened and the contents are pumped out. In the future, treatment continues and consists of the use of anti-inflammatory drugs and high-quality antiseptics. If this technique turns out to be ineffective, a classic operation is performed, when a specialist removes the tumor itself or all the tonsils if they show signs of hypertrophy and do not perform their protective functions.
The extent of surgical intervention depends on the size of the tumor, the condition of the ENT organs and the general well-being of the patient. The operation can be performed either under local anesthesia or general anesthesia. As a rule, long-term hospitalization of the patient is not required. It is very important to remove the cyst completely to eliminate the risk of recurrence of the pathology in the future. If the tumor is large, actively growing and often worsens tonsillitis and other ENT diseases, then a tonsillectomy is prescribed - an operation to remove the tonsils.
In our Clinic, such surgical interventions are performed using high-quality endoscopic equipment. Often, tonsillectomy is the only correct solution for frequently recurring tonsillitis and cysts on the tonsils.
After surgery, the patient is under the supervision of specialists for some time. Doctors monitor the patient’s condition and, if problems occur, provide the necessary medical assistance. The first day after removal of cysts or tonsils, you must observe relative rest: sports, visiting baths and saunas, and public swimming pools are prohibited. These restrictions are necessary to prevent bleeding and prevent the development of infectious complications. Food should be warm and as gentle as possible. During the first weeks, you should not eat foods that can injure the oral mucosa.
In the postoperative period, specialists can prescribe medications whose actions are aimed at relieving sore throat, relieving signs of inflammation and preventing secondary infections. Local procedures for gargling and irrigating the throat with antiseptics are also prescribed. Antiseptic treatment of the wound remaining after surgery must be carried out several times a day.
You should be attentive to your well-being and if you have any complaints, contact your doctor. Surgeries to remove cysts are successful, but in any case, patients must visit an otolaryngologist for several more months so that the doctor can monitor the quality of healing of the mucous membrane and, if there is a risk of relapse of the disease, can take all necessary therapeutic measures.
If you follow all medical recommendations and avoid heavy physical activity in the first weeks after surgery, the risk of relapse of the disease and complications will be minimal. You can ask the specialists of our Clinic in Yaroslavl all your questions. We will be happy to advise you and help you even in the most difficult clinical situations. For this, doctors have everything they need: innovative technology of European quality, rich practical experience of otolaryngologists, professional knowledge.
Prevention and treatment of tonsillitis in children
What are the difficulties in treating chronic tonsillitis? What procedures are included in the complex of preventive treatment?
In the structure of diseases of the ENT organs in children, a significant part is made up of infectious and inflammatory diseases of the palatine tonsils, which account for 20% of cases in the general population and up to 43% in the group of frequently ill children.
In the etiology of acute tonsillitis (angina), the main role is played by the following microorganisms: Hemophilus influenzae, Moraxella catharralis and beta-hemolytic streptococcus, the relevance of which in the development of the pathological process is still high.
Other microorganisms, such as viruses, streptococci of other groups, Neisseria, etc., are of significantly less importance.
Infection occurs by airborne droplets, the source is a sick person or, more importantly for children attending preschool institutions and schools, an asymptomatic carrier.
The clinical picture of acute tonsillitis, as a rule, is quite typical and does not cause diagnostic difficulties: there is an acute onset with a rise in body temperature from low-grade fever to severe hyperthermia, general weakness, headache, sore throat, aggravated by swallowing, enlargement and tenderness of the tonsillar lymph nodes.
During pharyngoscopy, the picture is also typical: hyperemic and edematous tonsils, soft palate, posterior wall of the pharynx, as well as lateral columns (in Western countries the diagnosis of tonsillopharyngitis is accepted; in the lacunae of the tonsils there are inflamed purulent follicles or widespread white-yellow overlays on the tonsils (but not extending beyond the tonsils, that is, not spreading to the arches and soft palate).The plaques are loose, easily removed from the surface of the tonsils. After removing the film, the tonsil does not bleed.
Diagnosis of catarrhal tonsillitis may present some difficulties when there is no plaque on the tonsils. But this is a somewhat special case: there is currently a discussion about the legitimacy of such a diagnosis, that is, the existence of catarrhal tonsillitis as such is being questioned. In these cases, it is proposed to make a diagnosis of acute respiratory disease.
A clinical blood test determines changes typical of the inflammatory process.
Ideally, before starting therapy, a microbiological examination of a smear from the tonsils is carried out to determine sensitivity to antibiotics.
Therapy for acute tonsillitis remains traditional: it is antibacterial therapy, and aminopenicillins with clavulanic acid (amoxiclav, augmentin) remain the drugs of choice. Synthetic penicillins retain their value only in the treatment of acute tonsillitis caused by beta-hemolytic streptococcus. Today, from the group of penicillins for oral administration, amoxicillin is the most important, surpassing other drugs in this group in its pharmacokinetic properties. Along with penicillins, cephalosporin antibiotics are used, with preference given to drugs of the first (cefadroxil) and second (cefuroxime, axetil, cefaclor) generations.
In case of intolerance to penicillins and cephalosporins, macrolides are used.
Along with systemic antibiotics, topical antiseptics are also used that have an anti-inflammatory and analgesic effect (hexasprey, hexoral, stopangin, tantum verde, etc.).
Irrational treatment of acute tonsillitis, in particular refusal of systemic antibiotic therapy or its unjustifiably shortened course, is one of the reasons for the chronicity of the process.
Treatment of chronic tonsillitis, both in the acute stage and in the remission stage, is associated with a number of difficulties. In particular, it is necessary to take into account that in a chronic process, as a rule, not an isolated flora is detected, but a mixed infection, which is much less amenable to antibacterial therapy. The most obvious way to treat chronic tonsillitis is surgery - bilateral tonsillectomy. In adult patients, this route is justified in any case. But as to whether tonsils should be removed in children, and if so, at what age, expert opinions differ. This is due to the fact that the lymphopharyngeal ring performs protective functions and is an immunocompetent organ. Therefore, a significant number of pediatricians believe that if chronic tonsillitis occurs in a compensated form, it is necessary to carry out conservative treatment.
The standard complex of preventive conservative treatment of chronic tonsillitis includes a set of procedures aimed at combating pathogenic microflora that is constantly located in the lacunae of the tonsils, improving the drainage of the tonsils, and correcting the body’s immunological defense. This complex includes washing the lacunae of the tonsils, lubricating the tonsils with antiseptic solutions, physiotherapeutic procedures (ultrasound in the submandibular area or laser therapy), and the use of immunomodulators. The course of treatment is carried out twice a year.
Our study was conducted to identify the most optimal scheme for the preventive treatment of chronic tonsillitis.
From April 2000 to June 2002, 68 children aged 7 to 12 years with a diagnosis of chronic tonsillitis, compensated form, were under our supervision. (Children under 7 years of age were excluded from the study, since contact with them was difficult and, therefore, there were limitations in carrying out the full course of complex therapy.) In 24 (35%) children, the disease occurred with exacerbations in the form of sore throats 1 time per year or 2 every three years, 6 of them had a history of peritonsillar abscesses. All parents categorically refused surgical intervention. The remaining 44 (65%) people had a compensated non-anginal form of chronic tonsillitis. (There was no documented diagnosis of tonsillitis in the medical history.)
All children complained of increased fatigue and periodic headaches. Parents paid attention to weakness, sweating, frequent colds, and a prolonged “unmotivated” increase in body temperature to subfebrile levels.
During examination, all children showed enlargement and hardening of the submandibular lymph nodes. Soreness was noted by 11 (16%) children included in the examination 7-10 days after suffering from tonsillitis.
All children had slight hyperemia of the mucous membrane of the tonsils and the posterior pharyngeal wall. The anterior arches were significantly hyperemic and injected with vessels. The tonsils are fused to the arches, with widened lacunae; there is pathological purulent discharge in the lacunae. 49 (72%) people had grade II tonsils and 19 (23%) people had grade III tonsils. 10 children had a purulent odor from their mouth.
All children under our supervision underwent a course of conservative treatment of chronic tonsillitis 2 times a year. Every other day, they washed the lacunae of the tonsils (from 8 to 10 procedures, depending on the effectiveness). In all cases, these procedures were combined with ultrasound examination of the submandibular area.
Washings were carried out with solutions of Hexoral (10 patients), Miramistin (20 patients), Octinosept (28 patients). These drugs were chosen due to the fact that they have a wide spectrum of antimicrobial and antifungal effects, are non-toxic, are not absorbed through intact mucous membranes, have a taste acceptable to children, and are available in the form of solutions.
After the treatment, a visual effect was noted after the 5th procedure: the tonsils shrank in size, acquired a pale pink color, the lacunae remained free, and the bad breath disappeared.
In addition to the direct impact on the tonsils with antiseptic solutions and the use of physiotherapy, we included in the complex of preventive procedures homeopathic remedies that have an anti-inflammatory effect, aimed at strengthening the lymphoid tissue. In particular, tonsilotren was used, a complex drug whose action is aimed at eliminating the symptoms of inflammation, reducing hypertrophy of the palatine and nasopharyngeal tonsils, as well as regional lymph nodes by improving the drainage of lymphoid tissue and the immunomodulatory effect.
The drug was prescribed as a tablet 3 times a day (at the same time a course of lavage of the tonsil lacunae and physiotherapy began) and was taken for a long time, for 6 weeks. The drug was well tolerated. In 4 (6%) children, tonsilotren had to be discontinued on the 4th day of treatment at the request of their parents due to a slight exacerbation of tonsillitis symptoms.
Control was carried out 3 months after the start of complex therapy. After the first course of preventive treatment, out of 64 children taking tonsilotren, 53 (83%) people did not have any complaints related to diseases of the ENT organs for 3 months. The pharyngoscopy picture remained satisfactory. 9 (14%) people suffered mild ARVI, 2 (3%) patients had ARVI with high fever and sore throat.
After 6 months (from the start of the first course), 64 people underwent preventive treatment again in full, excluding 4 children who did not take the homeopathic drug. During a follow-up examination carried out 6 months later (before the next course of preventive treatment), a satisfactory pharyngoscopy picture was noted, no pathological changes were observed in clinical blood and urine tests, and the ECG was within the age norm. During the reporting period, 59 (92%) people had virtually no complaints. 2 (3%) children suffered from ARVI, 1 child had bronchitis, 2 (3%) people suffered from follicular tonsillitis. In 1 child, tonsillitis was complicated by a peritonsillar abscess. The parents refused the operation.
During the observation period, the children received 5 courses of preventive treatment for chronic tonsillitis. During this time, the number of children suffering from acute respiratory viral infections and other respiratory infections sharply decreased. In 62 (97%) people, sore throats did not recur. The pharyngoscopy picture remained satisfactory.
In 2 children, bilateral tonsillectomy was performed due to the ineffectiveness of conservative treatment.
Thus, complex preventive treatment of chronic tonsillitis with the inclusion of antiseptic solutions and homeopathic drugs (tonsilotren) in the therapeutic regimen is highly effective and allows children to preserve the tonsils as a necessary immunocompetent organ and avoid traumatic surgery.
Literature
- Belov B.S. A-streptococcal tonsillitis: clinical significance, issues of antibacterial therapy // Attending Physician. 2002. No. 1-2. pp. 24-28.
- Karaulov A.V., Sokurenko S.I., Barmotin G.V. Principles of immunoprophylaxis and immunotherapy of recurrent respiratory diseases // MMA im. I. M. Sechenov, clinic of the Ministry of Foreign Affairs of the Russian Federation. M., 1999.
- Lazarev V.N. Adaptation reactions and their correction in chronic inflammatory diseases of the upper respiratory tract: Abstract of thesis. dis. ... doc. honey. Sci. M., 1995.
- Lopatin A. S. Treatment of acute and chronic pharyngitis // RMZh. 2001. T. 9. No. 16-17.
- Dagnelie CF Sore Throat in General Practice. A Diagnostic and Therapeutic Study. Thesis. Rotterdam, 1994.
- Rice D. H. Microbiology. In: Donald PJ, Gluckman JL, Rice DH Editors. The Sinuses. New York: Raven Press. 1995. pp. 57-64.
At the beginning of an exacerbation of chronic tonsillitis or in the postoperative period (after tonsillectomy), it makes sense to use topical antiseptics to accelerate the relief of inflammatory and pain symptoms in the oral cavity. In particular, the drug faringosept, which has a pronounced antiseptic effect and is available in the form of lozenges, has proven itself well. This ensures convenience and painlessness of its use, which is especially important in the postoperative period.
Prevention of recurrence of tonsil cysts
After removal of the cysts, relapse of the disease may occur. To avoid this, it is necessary to prevent the occurrence of situations that provoke inflammation of the mucous membrane of the oropharynx. Try to promptly treat ENT diseases, especially tonsillitis, and avoid injury to mucous tissues. If you smoke, if possible, give up the bad habit or reduce the number of cigarettes you smoke to 1-2 per day. Tars and other substances contained in tobacco have an irritating effect on the throat and can provoke an exacerbation of sore throats.
If the patient has a history of frequent ENT diseases and relapses of tonsillitis, then the doctor may recommend removing the entire tonsil. A tonsillectomy will relieve you of chronic infection and many other health problems. But tonsil removal is carried out according to indications. You can talk about the need for total resection with the doctors of the CONSTANTA Clinic at your appointment.
If you have any questions or make an appointment with a specialist, please call: (4852) 37-00-85 Daily from 8:00 to 20:00
Sign up for a consultation