Cheilitis, or, in simple terms, inflammation of the lip, is a fairly common disease. However, both the causes and development of cheilitis remain largely unknown. The development of the disease is associated with impaired lip closure and changes in the tone of facial muscles, a decrease in the height of the lower part of the face and age-related changes in soft tissues, bad habits and systemic diseases. By its nature, inflammation of the lip can be an independent disease: exfoliative, glandular, allergic, actinic and meteorological, and a symptom of a systemic disease: eczematous, atopic, macrocheilitis. This article will discuss the symptoms and treatment of cheilitis of various etiologies.
Glandular cheilitis
The clinical picture of glandular cheilitis is recognizable - the bumpy surface of the red border of the lips with droplets of “dew” - a light transparent liquid from the excretory ducts of small glands. After evaporation, the surface is dry, with cracks and erosions. The patient begins to worry not only about the appearance, but also about pain, swelling, and yellow-green or brown-black crusts.
Despite the fact that the clinical picture is quite typical, it is necessary to exclude diseases such as Miescher granulomatous cheilitis, sarcoidosis, Melkersson-Rosenthal syndrome, and Crohn's disease.
Etiology of glandular cheilitis
The etiology of glandular cheilitis is unknown, but hyperplasia and heterotopia of the minor salivary glands are of great importance. Develops on the lower lip along the Klein line in people over 30 years of age.
Treatment of glandular cheilitis
Treatment of glandular cheilitis is surgical - removal of the entire Klein zone with displaced glands. Deep electrocoagulation of the gland parenchyma or laser therapy is acceptable.
Symptoms
A typical clinical picture of this disease is characterized by the following symptoms:
- Glandular cheilitis begins with the appearance of a large number of red dots on the lips - previously absent on the surface of the mucous membrane of the openings of the salivary glands.
- The abundant secretion of saliva caused by external irritation leads to constant moistening of the lips, however, when the liquid evaporates, the skin immediately dries out, begins to peel, crack and itch.
- Over time, a precancerous tumor may form at the site of cracks and irritations.
- The lower lip is affected twice as often as the upper lip, and a large number of drops of salivary fluid are constantly visible on it.
- Swelling, pain, discharge of pus when infection enters the dilated gland ducts, formation of brown and marsh-colored crusts, as well as erosions and abscesses.
Miescher granulomatous cheilitis
Rare chronic diseases of the lower lip include Miescher's granulomatous cheilitis, which sometimes occurs with exacerbations. The causes of the disease are still unclear. The course is painless, and the patient looks like after unsuccessful lipofilling, and only sometimes small vesicles, erosions and crusts form.
It should be borne in mind that this is one of the forms of Melkersson-Rosenthal syndrome and is differentiated from Crohn's disease, sarcoidosis, glandular cheilitis, angioedema and lymphangioma. It is treated by removing the affected lip tissue.
Causes
The cause of the development of primary glandular cheilitis is genetic abnormalities and heredity. Parents suffering from pathologies and increased secretion of the salivary glands have a high risk of having a child with similar problems. The secondary type of disease can be caused by factors such as:
- decayed diseased teeth with sharp edges;
- tartar;
- periodontal disease and periodontitis;
- chronic inflammation of the skin of the lips.
Timely treatment of the problems described above helps to avoid damage to the glands, however, such an anomaly does not occur in all people who are faced with the above problems.
Melkersson-Rosenthal syndrome
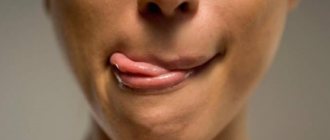
Melkersson-Rosenthal syndrome is a condition characterized by swelling of the lips, unilateral facial nerve palsy, and a folded tongue.
The causes of the syndrome are not fully understood, but an infectious-allergic origin is most likely. The patient is concerned about swelling of the lip and drooping of the corner of the mouth, which suddenly appeared and then recurred. The border of swollen lips may have cracks. On palpation, the lip is soft, elastic, without infiltration in the depth of the lesion. Acute swelling subsides after some time, but may recur. With each crisis, the lip tissue thickens. The lips are bluish-red in color, and some patients have a folded tongue.
Treatment of Melkersson-Rosenthal syndrome is carried out in two directions - surgical and conservative. The best results are obtained by conservative combined treatment with corticosteroids, broad-spectrum antibiotics, synthetic antimalarials, and desensitizing agents for 30-40 days. The course of treatment is repeated after 3 months.
Exfoliative cheilitis
Exfoliative cheilitis is a chronic disease of the red border of the lips and is accompanied by peeling of epithelial cells. The causes of cheilitis are still not clear, but preference is given to neurogenic disruptions.
There are 2 forms: dry and exudative, which can transform into each other.
Dry form of exfoliative cheilitis
The dry form of exfoliative cheilitis is characterized by the presence of a strip of thin transparent scales at the border of the red border and mucosa, attached in the center. 5-7 days after appearance they are easily removed, exposing the bright red surface of the border, but erosion does not form. Relapse. The disease is not prone to self-healing and lasts for decades.
Exudative form of exfoliative cheilitis
The exudative form of exfoliative cheilitis is characterized by yellow crusts on the hyperemic red border of predominantly the lower lip, which do not extend to the mucous membrane of the lip, nor to the skin, nor to the corners of the lips. After peeling off the crusts, a hyperemic surface without erosion is exposed.
Diagnosis is based on clinical examination. The exudative form occurs more easily than the dry form.
Treatment of exfoliative cheilitis
Treatment of exfoliative cheilitis with pathogenetic therapy with drugs that increase the body's reactivity, using hygienic lipsticks and balms.
Oral candidiasis - symptoms and treatment
If treatment is untimely or incorrect, acute candidiasis can become complicated and become chronic or invasive, which is difficult to treat. In addition, complications such as fungal esophagitis, tracheitis, gastrointestinal candidiasis, and candidal sepsis may occur. There is a high probability of inflammation of the genital organs in women and men.
Candidal esophagitis (inflammation of the esophagus). Symptoms: signs of intoxication of the body, bloating, heartburn, sore throat, dysphagia (difficulty swallowing solid food), bitterness in the mouth or sour taste. Can lead to esophageal ulcers, rupture of the esophageal tube, internal bleeding, stricture (narrowing of the lumen) of the esophagus.
Candidal tracheitis (inflammation of the trachea). Symptoms: increased body temperature up to 37 °C, severe pain in the trachea, chest, shortness of breath and a feeling of suffocation when coughing, itching, burning, pain behind the sternum or between the shoulder blades, the appearance of ulcers on the skin. Through abscesses on the walls of the trachea, the fungus can penetrate into the blood, which will subsequently lead to sepsis.
Candidiasis of the gastrointestinal tract . Candida penetrates the intestines and injures the mucous membrane, causing a severe form of dysbiosis. Symptoms: nausea, vomiting with blood and whitish films, increased body temperature to 37-38 °C, bloating and pain in the upper abdomen, diarrhea mixed with white flakes. If the stomach wall is perforated, serious consequences can occur, such as peritonitis (inflammation of the peritoneum) or internal bleeding.
Also a severe complication of oral candidiasis is candidal meningitis , which can be fatal. Most often, the complication occurs in patients with severe concomitant diseases (immunodeficiency, decompensated diabetes mellitus) and in people with reduced immunity. Candidal meningitis is manifested by the following symptoms: increased body temperature to 37.2-37.9 °C, cephalalgia (constant headaches), drowsiness, hemorrhagic rash throughout the body, vomiting, which does not bring relief to the patient, often without preceding nausea. Neurological symptoms may appear: disturbances of consciousness, higher nervous activity, movement disorders, sensitivity, vision.
The danger of the disease lies in a sharp decrease in the body's immunity and the rapid spread of infection to the spinal cord and brain. There are also difficulties in diagnosing the disease due to the erased symptoms and the absence of pronounced meningeal syndrome (signs of irritation of the meninges).
Attachment of a secondary infection. Inflamed organs and tissues are very sensitive to other infections. They penetrate most quickly through ulcers and cracks with bleeding. When a secondary infection is added, ulcerative necrotizing stomatitis or Vincent's tonsillitis, syphilitic seizure, syphilitic dysphonia (impaired vocal function), etc. may occur.
Candidal sepsis is the introduction of a fungal infection into the general bloodstream. A serious condition in which candida penetrates into all organs and tissues. Signs of intoxication of the body: nausea, vomiting, abdominal pain, tachycardia and body hyperthermia develop (increase in temperature above 38 ° C), multiple organ failure occurs (disruption of several functional systems of the body), and the activity of the central nervous system (CNS) is disrupted. In this condition, treatment is carried out only in intensive care units, since if assistance and special therapy are not provided in a timely manner, the outcome can be fatal [2].
Actinic cheilitis
Actinic cheilitis is a chronic degenerative disease of the lower lip.
The reason is the increased sensitivity of the red border of the lips to ultraviolet radiation. The clinic distinguishes two forms - dry and exudative.
In the dry form of actinic cheilitis, the patient complains of dryness of the red border of the lips; it is bright red in color and covered with silver-white scales.
In the exudative form, there is a bright red border with bursting blisters, erosions, crusts and cracks.
Treatment is etiological - less sunlight, as well as the use of ointments with corticosteroids and B vitamins.
Treatment
If symptoms of this disease are detected, the patient should seek help from a dentist, dermatologist and infectious disease specialist as soon as possible. ointments that relieve inflammation are still used : hydrocortisone, prednisolone or naphthalan.
In case of secondary cheilitis, it is more logical to resort to this type of treatment for granular cheilitis, such as diathermocoagulation . The essence of this procedure is to cauterize pathological and hypertrophied glands with electric current using a thin electrode. Another treatment option is surgical excision of such glands. Lack of timely treatment can lead to the formation of lip cancer.
Contact allergic cheilitis
Allergic cheilitis occurs during contact with various chemical agents, more often in women, because the cause is the chemicals contained in lipsticks, toothpastes, denture plastics, etc. The disease can be of an occupational nature. In the clinic - hyperemia and swelling of the red border of the lips, peeling, cracks, and in more severe cases - blisters and erosions. The acute onset and causal relationship of contact cheilitis with chemicals are the starting point for making a diagnosis.
Treatment of allergic cheilitis begins with eliminating the chemical factor. Locally - corticosteroid ointments, plus desensitizing therapy.
Angular cheilitis
We saw cracks in the corners of the interlocutor’s mouth - he has angular cheilitis due to iron deficiency anemia, riboflavin hypovitaminosis, increased levels of fungi of the genus Candida, Streptococci, Staphylococci, or simple mechanical trauma. With a decrease in the height of the lower part of the face, the folding of soft tissues in the corners of the mouth becomes the cause of the accumulation of microflora, and the actual inflammatory and destructive processes. Therefore, treatment of angular cheilitis sometimes consists of correcting the occlusal height; for streptococcal infection, in combination with ointments containing antibiotics; for candidiasis, with nystatin ointment.
Prevention methods
Careful oral hygiene
To prevent the appearance of cracks, you need to protect the skin and mucous membranes from adverse effects. To do this, you should get rid of the habit of licking your lips and corners of your mouth, using medicinal cosmetics for dry skin and hygienic lipsticks. To prevent infection from getting onto the skin of the lips from the oral cavity, it is necessary to brush your teeth at least twice a day, as well as treat caries and inflammatory gum diseases.
Changing your diet
If pockets begin to appear in the corners of the mouth, it is necessary to limit the consumption of spicy, sour and salty foods that irritate the mucous membranes and skin. You can add non-acidic fruits and vegetables to your daily diet, as well as foods containing iron and riboflavin (beef, liver, dairy products, cabbage, potatoes, peanuts, almonds, etc.).
Up to contents
Abrasive precancerous cheilitis Manganotti
Manganotti cheilitis occurs in men over 50 years of age, most often on the lower lip. There must be one or more erosions of a round or irregular shape with a smooth red surface on the red border of the lip. In some patients, crusts form on it. They can recur and become malignant.
We distinguish Manganotti cheilitis from the erosive form of lupus erythematosus, lichen planus and leukoplakia, pemphigus, exudative erythema multiforme and herpetic erosion, primary syphiloma.
Treatment of cheilitis by eliminating local traumatic factors. A concentrate of vitamin A, nicotinic acid, methyluracil, corticosteroid ointments, and epithelializing ointments are effective. If conservative treatment within 1 month does not lead to epithelization of erosion, the lesion is removed.
Atopic cheilitis
Atopic cheilitis is a symptom of dermatitis or neurodermatitis in children and adolescents from 7 to 17 years old. Genetics comes to the fore among the factors causing inflammation. Klinkartina is characterized by damage to the red border of the lips and skin in the area of the corners of the mouth, but does not extend to the mucous membrane. The patient is concerned about itching, erythema, swelling with inflammation of the skin in the corners of the mouth. Then peeling appears. Desensitization and corticosteroids are the treatment of choice for atopic cheilitis.
Meteorological cheilitis
Regardless of the time of year, meteorological cheilitis occurs in response to unfavorable weather for the body. The disease is chronic and occurs more often in men. The border of the lips is infiltrated, dry, congestively hyperemic and covered with small crusts.
Treatment of meteorological cheilitis consists of protecting the lips with balms and vitamin ointments.
Eczematous cheilitis
Manifests itself as a symptom of facial eczema. Allergens include components of toothpastes, lipsticks, food substances, denture materials, and the like.
Eczematous cheilitis begins with redness and small blisters filled with yellowish serous contents. The bubbles merge with each other, burst, a weeping surface is formed, then crusts. All this is accompanied by itching and swelling of the lips. The lesion quickly spreads to the skin and corners of the mouth. The disease lasts for years with frequent exacerbations.
They treat it like skin eczema - desensitization, vitamins, ointments with corticosteroids.
Manifestations and stages
Cheilosis is a common inflammatory problem. When the lip tissue is damaged, signs such as increased dryness and redness, the development of wounds and ulcers, and pain appear. Often develops due to poor ecology, irritation caused by food or chemicals. In some cases, it is caused by other diseases, that is, it acts as a symptom.
The following types of lesions are observed in children:
- traumatic;
- exfoliative;
- contact;
- meteorological;
- grandular and angular cheilitis in children;
- microbial.
The traumatic form occurs due to mechanical, chemical and other influences, after which infection develops. Swelling appears, the mucous membrane becomes tense, and lip movements become limited. In some cases, this type of cheilitis is caused by herpes in the acute stage. For treatment, antibiotics, antiseptics or anti-inflammatory drugs are prescribed.
The exfoliative type of the disease is accompanied by increased dryness and peeling. The reason is a lack of vitamin B, ascorbic or nicotinic acid. The problem arises with dysfunction of the endocrine or nervous system, impaired lip closure, or mouth breathing. Therapy is prescribed depending on the cause of the lesion; multivitamins and softening creams are often used.
Allergic, or contact, cheilitis in most cases develops in adolescents. The causes are chemicals and other external factors. Manifestations of the disease include itching or burning, blisters on the surface, and dryness. To eliminate the problem, you need to avoid contact with the substance that caused the allergy and take antihistamines.
In addition, there are:
- atopic cheilitis in children, which is accompanied by peeling, swelling, erythema and edema;
- hypovitaminosis, characterized by cracks, soreness, the causes are bad habits, for example, frequent licking of lips;
- Eczematous cheilitis is not an independent disease, but one of the symptoms of an inflammatory process affecting the skin.
Cheilitis in children
A fairly common condition that persists for a long time. Cheilitis in children is associated primarily with a violation of the architectonics of the lips at this age, systemic diseases, as well as the love of children to pull any objects into their mouths.
A feature of cheilitis in childhood is its acute onset, long course against the background of immune failure.
Important importance should be given to autoanesthesiophagy - “self-biting” after anesthesia. Before administering anesthesia to a child, the parent should be warned about possible biting of the lips and cheeks, and to speed up healing we use proteolytic enzymes and epithelializing ointments.
The article was written by O. Vishnyak specifically for the OHI-S.COM website. Please, when copying material, do not forget to provide a link to the current page.
What it is
Increased sensitivity of the skin of the lips to external weather influences, such as frost, sun and wind, ultimately leading to an inflammatory process and dysplasia, is called meteorological cheilitis. This lip lesion usually occurs in people who spend a long time outdoors (road workers, construction workers, beach lifeguards and representatives of other professions), therefore it is believed that it is men of working age, from 20 to 60 years old, who are most at risk of developing this type of cheilitis. However, actinic cheilitis or the so-called “farmer's lip” can develop in both women and children who spend a long time in the sun, for example, during a vacation at the seaside.
Meteorological cheilitis refers to inflammatory lesions of the lips and photoallergic reactions, while it is also classified as a precancerous disease. Therefore, a person who is faced with this type of damage to the skin of the lips must urgently contact a dentist and dermatologist, because this disease can progress very quickly.