Chronic tonsillitis
– a disease of the upper respiratory tract, which is characterized by a long-term inflammatory process of the tonsils.
The cause of the development of chronic tonsillitis is most often an ineffective or incomplete course of treatment for acute tonsillitis, leading to the formation of foci of inflammation of the tonsils and the activation of pathogenic organisms during the period of exacerbation of the disease.
THE INSTITUTE OF ALLERGOLOGY AND CLINICAL IMMUNOLOGY has:
- range of services for accurate diagnosis of ENT diseases
- special treatment programs
- courses of effective procedures conducted by specialists of our institute for more than 10 years
- consultations are carried out by doctors with academic degrees.
When concomitant diseases are identified, consultations are held with specialists in related fields (allergists-immunologists, endocrinologists, neurologists, gastroenterologists), and if necessary, consultations are held with Doctors of Medical Sciences.
Symptoms
Rheumatism of the joints, inflammation of the myocardium, endocardium can be a consequence of chronic tonsillitis! Strictly follow the instructions of the otorhinolaryngologist!
- Frequent sore throats.
- Local symptoms: sore throat, discomfort, sore throat, etc.
- Bad breath.
- Reflex coughing attacks caused by irritation of the mucous membrane of the palate and larynx.
- Enlarged cervical lymph nodes (this symptom is typical for children and adolescents, but can occur in adults).
- Low-grade fever.
- Headache, weakness, weakness.
- Changes in the heart.
Classification
| Simple form Characteristic: the course of the disease with local symptoms, subjective complaints and objective signs of the disease, with frequent sore throats, and in other cases - without repeated sore throats (“anginless” chronic tonsillitis). | Toxicallergic form Characterized by: low-grade fever, phenomena of tonsillogenic intoxication, manifestations of tonsillocardiac syndrome. |
Causes
The etiology and pathogenesis of chronic tonsillitis has not been fully studied to date.
The starting mechanism in the development of chronic tonsillitis is repeated inflammatory processes leading to local immunosuppression.
- Local causes are infectious foci (carious teeth, purulent sinusitis, etc.).
- Pathogenic and opportunistic microorganisms.
- Immunodeficiency states.
- Persistent violation of nasal breathing (adenoids in children, deviated nasal septum, etc.).
- Allergic sensitization of the body.
Diagnostics
THE INSTITUTE OF ALLERGOLOGY AND CLINICAL IMMUNOLOGY has a fundamental base that allows it to carry out the full range of diagnostic and therapeutic measures for any form of allergy that meets the level of international standards. Many of the diagnostic and treatment methods were developed by the staff of our Institute.
Diagnostic measures are based on anamnesis, clinical picture and laboratory diagnostics.
- Bacteriological examination of mucus from the tonsils and posterior pharyngeal wall for aerobic and facultative anaerobic microorganisms.
- Determination of the sensitivity of microorganisms to antibiotics and other drugs.
- Detailed general (clinical) blood test, clinical urine test.
- Determination of the concentration of C-reactive protein in blood serum.
- Determination of antistreptolysin-O in blood serum.
Pathology
Developmental anomalies
. Developmental anomalies include the palatine lobule and the accessory palatine M. Sometimes, instead of one palatine M, two M develop on each side. Additional lobules hanging on the stem have been described. As a rule, these anomalies do not require treatment.
Damage
— burns, wounds of M. — are rare in isolation; more often they are combined with internal and external injuries of the pharynx (see).
Foreign bodies
- most often fish bones, which can penetrate into the muscle tissue, causing pain when swallowing. Remove them with tweezers or special forceps. After removal, a disinfectant rinse and a gentle diet are recommended for one to two days (see Foreign bodies, pharynx).
Diseases
Rice.
6. Schematic representation of the first stage of the tonsillotomy operation: the hyperplastic area of the left palatine tonsil is captured by the tonsillotomy ring. Acute disease of palatine M.— acute
tonsillitis
, or tonsillitis
(see). Hron, inflammation of the palatine M.—tonsillitis (see). Hyperplasia of the palatine membranes occurs in children; there are no signs of inflammation. M. are only increased in size. If hyperplasia causes difficulty breathing or swallowing, children undergo surgery - tonsillotomy (Fig. 6), i.e. partial cutting off of the protruding part of the M. Before the operation, a full wedge examination is necessary.
The operation is low-painful, most often performed without anesthesia, on an outpatient basis, with a special instrument - a guillotine-shaped knife - tonsillotome, the size of which is selected according to the size of the removed muscle. Hyperplasia of the palatine muscles is in most cases accompanied by the proliferation of adenoid tissue of the nasopharynx, therefore tonsillotomy is often combined with adenotomy (see . Adenoids). Bleeding after tonsillotomy is usually minor and stops quickly. The child should remain under medical supervision for 2-3 hours. It is recommended to observe bed rest for 1-2 days, then semi-bed rest for 3-4 days. Food should be liquid and mushy, at room temperature.
Acute inflammation of the pharyngeal M., or acute adenoiditis
(see), observed mainly in children. In this case, the tubal M. may also be involved in the inflammatory process. Inflammation is catarrhal, follicular or fibrinous in nature. Due to the anatomical proximity of the mouth of the auditory tube, symptoms of tubo-otitis may occur (see).
Isolated disease of the lingual M. is much less common. It occurs in middle-aged and elderly people and may be accompanied by an abscess of the lingual M.; occurs with high fever, difficulty swallowing and speaking, and severe pain when protruding the tongue.
With angina of the lateral ridges of the pharynx, inflammation occurs in the lymphoid follicles scattered along the back wall and in the lateral lymphoid ridges (columns). Often a whitish dotted coating appears on individual follicles of the posterior pharyngeal wall.
A disease of the lymphoid tissue of the larynx is called laryngeal angina
; it is manifested by high fever, general malaise, sharp pain when swallowing food and palpating the larynx area. Plaques are often visible, and there may be swelling of the outer ring of the larynx (see Laryngitis).
In addition to the primary lesion of the tonsils, changes in the lymphoid tissue of the pharyngeal ring occur with blood diseases. With leukemia (see), infectious mononucleosis (see Infectious mononucleosis), lymphogranulomatosis (see), an increase in palatal M. can cause difficulty breathing and swallowing. Ulcerative changes in the palatine muscles, such as necrotizing tonsillitis, are also possible.
With syphilis, the palatine M. are affected in all stages of the disease. There are descriptions of hard chancroid M.: against a limited hyperemic background in the upper part of M. a hard infiltrate appears with painless erosion in the center, the edges soon turn into an ulcer with compacted edges and bottom; the lesion is unilateral, characterized by regional lymphadenitis (see). In stage II of syphilis, syphilitic tonsillitis occurs: round or oval plaques, separate and confluent, appear on the muscle, rising above the surface of the muscle, surrounded by a reddish rim, easily ulcerating; characterized by bilateral lesions; the entire M. is enlarged, dense, covered with plaque; Papules are found on the mucous membrane in the corners of the mouth, on the palatine arches, and along the edge of the tongue. In stage III, gumma can lead to the disintegration of M., which threatens bleeding from large vessels. Treatment - see Syphilis.
Primary M. tuberculosis is rare; its main symptom is difficulty swallowing and nasal breathing as a result of concomitant M. hyperplasia. Secondary M. damage can be observed in patients with pulmonary tuberculosis. Both forms can occur hidden, simulating a banal chronic condition, tonsillitis. Treatment - see Tuberculosis.
Treatment
There are two main methods of treatment: surgical and conservative.
The treatment method is determined by an otorhinolaryngologist, which depends on:
- forms of chronic inflammation;
- frequency of exacerbations;
- the presence or absence of beta-hemolytic streptococcus in the tonsils;
- effectiveness of previous therapy.
Conservative treatment method:
- Local antibiotic therapy
- Systemic antibiotic therapy (tablet or injection forms).
- Rinsing the lacunae of the tonsils and introducing antibacterial and anti-inflammatory drugs into them.
- Physiotherapeutic procedures:
- phonophoresis of drugs,
- ultraviolet radiation (UV),
- magnetic laser therapy (MILTA),
- vibroacoustic impact.
Physiology
Having a common structure with other lymphatic organs (see Lymphoid tissue), M. perform similar functions—hematopoietic (lymphocytopoiesis) and protective (barrier). The follicular apparatus, embedded in the mucous membranes, is a lymphoid barrier, biol, whose role is the neutralization of toxic substances and inf. agents that enter mucous membranes from the environment. In human M. there are both thymus-dependent and thymus-independent populations of lymphocytes (see), which carry out reactions of both cellular and humoral immunity (see). M. are a peripheral organ of immunity that has a certain uniqueness. Firstly, they have a lymphoepithelial structure, secondly, they are the entrance gates for microbial antigens and, thirdly, they lack lymphatic vessels. It is known that M. contain cells that produce antibodies of the IgE class, which are believed to perform a protective function. It has been shown that lymphocytes of M.'s lymphoid tissue produce interferon (see), which is a nonspecific factor of antiviral immunity.
Systemic therapy for the treatment of chronic tonsillitis at IAKI LLC
Washing the lacunae of the tonsils in combination with physiotherapeutic procedures has a good therapeutic effect and is widely used at the Institute.
First stage (washing the lacunae of the tonsils)
1. Washing of the tonsils can be done using the Belogolov’s method (Fig. 1) and using hardware methods (using the ATMOS ENT combine (Fig. 2) and the Tonsilor-M apparatus, etc.).
The choice of method depends on diagnostic and therapeutic purposes and is determined by an otorhinolaryngologist.
The antiseptic pressure created by the syringe piston effectively removes large purulent plugs. The disadvantage of the method is that it is traumatic when there is a pronounced gag reflex and the inability to qualitatively clean lacunae of small and medium diameter from purulent caseous contents. This method is widely used when it is necessary to obtain material for diagnostics, as well as for certain anatomical features of the structure of the palatine tonsils.
Rice. 1. Washing according to Belogolov’s method
2. Rinsing the lacunae of the palatine tonsils with a vacuum apparatus “ATMOS” (Fig. 2).
During rinsing, vacuum action allows you to effectively and painlessly remove even purulent plugs located deep in the lacunae. The method is non-traumatic and suitable for treatment in all age groups (vacuum attachments are selected taking into account the age and size of the tonsils). During rinsing, the tonsil is treated with an antiseptic solution.
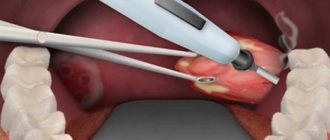
3. Vacuum rinsing of the palatine tonsils with the “Tonsilor-M” apparatus (Fig. 2)
One of the advanced and effective methods of conservative treatment of chronic tonsillitis. The principle of operation of the Tonsilor-M device is based on creating a vacuum at the point of application and emitting low-frequency ultrasound onto the affected tissue of the palatine tonsil. Ultrasonic waves provide cavitation and aspiration of purulent contents from the lacunae of the tonsils, accelerate regeneration processes without causing allergic reactions or addiction, enhancing the therapeutic effect. The device is equipped with special nozzles that allow you to deliver an antiseptic solution directly to the tonsils.
Rice. 2. Washing using an ENT combine “ATMOS”, a device “Tonsilor-M”
Second stage (treatment with an astringent antiseptic solution)
After washing the lacunae of the palatine tonsils and clearing them of purulent contents, the tonsil tissue is soaked with a tampon with an astringent antiseptic agent (Fig. 3).
Rice. 3. Treatment of tonsils with an antiseptic solution
Third stage (laser therapy)
The next stage is a physiotherapeutic effect on the tissue of the palatine tonsil (Fig. 4) using a low-intensity ultraviolet laser beam, aimed at reducing swelling and inflammation of the tissue of the palatine tonsils.
Rice. 4. Laser therapy session after rinsing
Fourth stage (transdermal (percutaneous) exposure to an infrared magnetic laser)
Next, a transdermal (percutaneous) effect of an infrared magnetic laser (Fig. 5) is performed on reflexogenic ENT points: the maxillary region of the projection of the palatine tonsils, the region of the larynx and thyroid cartilage and the projection region of the exit site of the second branch of the trigeminal nerve on the face.
Rice. 5. Transdermal (percutaneous) exposure to an infrared magnetic laser
Fifth stage (vibroacoustic impact)
It is recommended to conduct sessions of vibroacoustic influence; the use of this method is necessary to improve the trophic (nutritional) function and normalize microcirculation in the tissues of the palatine tonsils.
Stage six (therapeutic low-intensity laser exposure)
In some cases, in the treatment of chronic tonsillitis, it is possible to alternate a therapeutic low-intensity laser (Fig. 7, Fig. 8) with other types of physiotherapeutic effects: ultraviolet irradiation (UVR, “quartz tube”) of the mucous membranes of the ENT organs and vibroacoustic effects on the projection area of the palatine tonsils.
This method allows for the sanitation of the microflora located on the surface of the palatine tonsils and the nasal cavity due to ultraviolet irradiation (UVR).
Rice. 7. Sanitation of the microflora of the nasal cavity using ultraviolet irradiation.
Rice. 8. Sanitation of microflora on the surface of the tonsils using ultraviolet irradiation.
Systemic therapy for chronic tonsillitis is carried out in courses (usually spring, autumn). The number of procedures is determined by an otorhinolaryngologist. For a lasting effect to occur, at least five sessions must be performed. If, during the procedure, purulent caseous contents continue to be washed out of the lacunae of the palatine tonsils, the washing procedures must be continued “until clean rinsing waters”. Typically the course duration is 10 procedures.
It is advisable to conduct courses 2 to 4 times a year; between courses it is necessary to carry out medication prescribed by an ENT doctor.
A course of washing the tonsils not only reduces the risk of exacerbation of chronic tonsillitis, but also prevents the occurrence of other ENT pathologies, and also avoids the need to remove the tonsils.
Attention! If, after completing the course, the formation of purulent caseous contents occurs 2-4 weeks later, the doctor may recommend surgical removal of the tonsils.
With systemic therapy, surgical treatment methods are rarely used!
The consequences of chronic tonsillitis most affect the heart and joints! Rheumatism of the joints, inflammation of the myocardium, endocardium can be a consequence of chronic tonsillitis! DO NOT SELF-medicate! CONTACT AN OTOLARINGOLOGIST!
It is not recommended to use antibacterial drugs in the chronic process, however, in the acute period there is a need for their use.
Attention!
The selection of drug therapy should be made individually, taking into account the severity of the disease, the presence of concomitant diseases, the patient’s age and the risk of possible side effects. Strictly follow the instructions of the otorhinolaryngologist! We ask you not to self-medicate based on Internet data!
Branch phone:
+7 (495) 695-56-95
Anatomy
Palatal
The tonsil is a paired formation located in the fossa of the tonsils (fossae tonsillares) of the lateral walls of the pharynx between the palatoglossus arch (areus palatoglossus) and the velopharyngeal arch (areus palatopharyngeus). It has an oval shape, its long axis runs from top to bottom and somewhat from front to back. In a newborn, the size of the palatine m. in the vertical direction is 10 mm, in the transverse direction 9 mm, thickness 2.1 mm; in an adult, respectively, 15-30 mm, 15-20 mm, 12-20 mm. In the palatal M., two surfaces are distinguished: internal (free) and external, facing the wall of the pharynx. The inner surface is uneven, covered with a mucous membrane, has 8-20 irregularly shaped tonsillar dimples (fossulae tonsillares), which are the mouths of tonsillar crypts (cryptae tonsillares), which, branching, penetrate the thickness of the palatine membrane. The crypts increase the free surface area of each palatine membrane up to 300 cm2. When swallowing, the palatine membranes are slightly displaced, and their crypts are freed from their contents. The outer surface of the palatine membranes is covered with a capsule (capsula tonsillae) up to 1 mm thick; on it lies a layer of loose paratonsillar tissue, the edges go down to the root of the tongue, in front it communicates with the tissue of the palatoglossal arch, at the top - with the submucosa of the soft palate. In an adult, the distance to the internal carotid artery from the upper pole of the palatine M. is 28 mm, from the lower pole 11-17 mm, to the external carotid artery 41 mm and 23-39 mm, respectively. The upper corner of the M.'s fossa remains free and is called the supratonsillaris fossa. Sometimes there is an additional palatine M.—the palatine lobe of the palatine M., the edges of which can extend deep into the soft palate and not have a direct connection with the main palatine M. (Fig. 2). In these cases, it represents an additional intrapalatine M. (tonsilla intrapalatina accessoria), the edges usually contain a deep branched crypt - the sinus of Tourtuali, which plays a certain role in the pathology of the M.
Pharyngeal
M. (syn.: nasopharyngeal M., Lushka's tonsil, third M.) is located on the border of the upper and posterior walls of the pharynx (see), has the appearance of a round-shaped plate with 4-8 folds of the mucous membrane diverging on its surface, protruding into the cavity nasopharynx. The pharyngeal M. is well developed only in childhood; with the onset of puberty, its reverse development occurs.
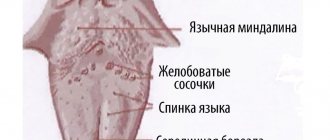
lingual
M. (syn. fourth M.) is located in the region of the root of the tongue (see), occupying almost the entire surface of the root of the tongue. Its shape is often ovoid, the surface is uneven, and lingual follicles (folliculi linguales) are located on the mucous membrane, divided by grooves into a number of folds. M.'s crypts are shallow, at the bottom of many crypts the excretory ducts of the salivary glands open, the secretion of which helps to wash and cleanse the crypts. In a newborn, the lingual M. is well developed, its longitudinal size is 6 mm, transverse 9 mm. After 40 years, a gradual reduction of lingual M occurs.
Pipe
M. is a paired formation, which is an accumulation of lymphoid tissue in the thickness of the mucous membrane of the nasopharynx at the pharyngeal opening of the Eustachian tube (see Auditory tube).
In a newborn, the tubal M. is well defined, approx. 7.5 mm, diameter approx. 3.5 mm. Tubal M. reaches its greatest development at 5-7 years of age; later it gradually atrophies and becomes almost invisible. Rice.
3. Schematic representation of the blood supply to the palatine tonsil: 1 - external carotid artery; 2 - maxillary artery; 3 - descending palatine artery; 4 - ascending pharyngeal artery; 5 - ascending palatine artery; 6 - facial artery; 7 - lingual artery; 8 - superior thyroid artery; 9 - common carotid artery; 10 - internal carotid artery; 11 - palatine tonsil. The blood supply to the tonsils of the lymphoepithelial pharyngeal ring, including the palatine M. (Fig. 3), is carried out by arterial branches (aa. tonsillares), extending directly from the external carotid artery or its branches: the ascending pharyngeal (a. pharyngea ascendens), lingual (a. lingualis), facial (a. facialis), descending palatine (a. palatina descendens). M.'s veins are formed in the parenchyma, accompany the arteries and flow into the pharyngeal venous plexus (plexus venosus pharyngeus), lingual vein (v. lingualis), and pterygoid venous plexus (plexus venosus pterygoideus). M. does not have afferent lymphatic vessels. The draining lymphatic vessels flow into the lymph nodes: parotid, retropharyngeal, lingual, submandibular. M.'s innervation is carried out by the branches of the V, IX, X pairs of cranial nerves and the cervical part of the sympathetic trunk. In the subepithelial layer of connective tissue septa, M.'s parenchyma, there are individual nerve cells, their clusters, pulpy and non-pulpate nerve fibers, various types of nerve endings, and extensive receptor fields. The blood supply and innervation of the muscle change with age.