Trigeminal and facial neuralgia
Neuralgia is a disease in which damage or compression of the trigeminal nerve and/or its branches occurs. This causes a sharp piercing pain that occurs suddenly and brings physical and psychological discomfort to the patient. Despite the fact that the term “neuralgia” can be literally translated as “nerve pain,” the matter is not limited to pain. Trigeminal and facial neuralgia are radically different in symptoms. The facial nerve contains mostly motor fibers, so neuralgia leads to dysfunction of the facial muscles (the degree depends on the severity of the disease), and can also cause lacrimation, dry eyes and partial loss of taste. Pain in facial neuralgia is usually concentrated in the area of the parotid gland (the patient complains that the pain radiates to the ear), but there may be no pain at all. It is because of the lack of pain that some experts use the term “neuropathy” when talking about damage to the facial nerve. With the trigeminal nerve it’s exactly the opposite, since it contains many sensory fibers.
When pain is considered abnormal
Pain in the gums that lasts longer than seven days, increased body temperature and facial asymmetry indicate the development of complications after surgery. In order for the pain to go away, it is necessary to identify the cause of its occurrence.
The gums may hurt for the following reasons: - severe trauma to the soft tissues of the periodontium during removal; — the trigeminal nerve was damaged during the removal procedure; — non-compliance by medical personnel with antiseptic measures; - inflammation of the socket due to the developing activity of bacteria in the oral cavity; - failure of the patient to comply with the specialist’s recommendations.
Dental surgeon's mistake
The complex structure of a wisdom tooth, breakdown of medical equipment or human error may be the reasons why an error was made during removal. That is, in this case, prolonged pain in the gums can result from:
— incorrectly chosen removal method; — tooth fragments were left in the wound; - use of aggressive antiseptic agents during treatment of the hole; — use of non-sterile instruments and dressings.
If the gums are swollen after removal, and after several hours a blood clot has not formed in the socket, we can confidently speak of a medical error.
Symptoms of neuralgia
- Facial pain (prosopalgia). A characteristic sign of neuralgia. Sharp and sudden, reminiscent of an electric shock. Usually lasts from 5 to 15 seconds, is paroxysmal in nature and can occur at any time. During periods of remission, the number of attacks decreases. Most often, pain occurs in the area of the cheekbones and lower jaw (both right and left), and can be localized in almost all areas of the face.
- Impaired sensitivity. A severe form of neuralgia can lead to partial or complete loss of sensitivity of the skin.
- Nervous tic of the eyelid (nystagmus), spasms and twitching of facial muscles.
- Loss of coordination and motor skills are rarer manifestations of severe forms of the disease.
- Headaches, fever, chills and weakness are syndromes caused by viruses and infections.
Causes
Unlike neuritis, neuralgia is not an inflammatory disease. Fever, fever, swelling and other symptoms of the inflammatory process are not associated with this disease. However, if the trigeminal nerve is damaged due to neuritis, pain sensations that fit the description of neuralgia may well occur. To avoid confusion and differentiate the two pathologies, it is necessary to consider their etiology.
The cause of neuritis (like any other inflammatory disease) is viruses and infections that cause gradual destruction of the membrane and nerve trunk, and classical neuralgia in the vast majority of cases occurs due to mechanical effects on the nerve. Today, experts identify dozens of factors that provoke the development of the disease.
Main causes of neuralgia
- Head injuries leading to changes in the cranial structure and displacement of bones.
- Benign and malignant tumors that, as they grow, compress the trigeminal nerve.
- Various bite pathologies and other dental anomalies.
- Pathologies of the structure and diseases of blood vessels located in close proximity to the nerve (atherosclerosis, aneurysm, vasodilatation, etc.).
- Sinusitis and otitis in chronic form.
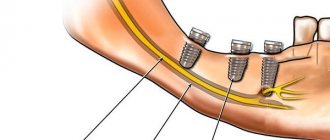
- Trigeminal neuralgia after tooth extraction. Occurs during a traumatic or incorrectly performed extraction procedure.
- Damage as a result of infection resulting from a number of diseases: periodontitis, periodontitis, stomatitis, herpes, syphilis.
Trigeminal neuralgia from hypothermia occurs rarely. However, this factor contributes to the development of the disease and complicates treatment. The same can be said about decreased immunity, metabolic disorders, neurosis, diabetes and other complicating factors.
How is a wisdom tooth removed?
Extraction of the third molar is performed for the following reasons::
- incorrect location causing discomfort to the patient;
- carious lesions that cannot be treated due to difficulty in accessing the dental unit;
- severe destruction;
- before starting orthodontic treatment.
After examination and diagnosis, the specialist decides whether to preserve or remove the tooth. There are two types of figure eight extraction: simple and complex.
Easy removal:
- anesthesia;
- tooth extraction using forceps or an elevator;
- removing debris and splinters from the hole;
- treatment of the hole with antiseptic agents;
- applying a bandage to stop bleeding.
Extraction of a wisdom tooth located under the gum and in a horizontal position is considered difficult This procedure includes the following steps:
- anesthesia;
- cutting the gums with a scalpel;
- sawing the tooth (the root is separated from the crown using a bur);
- extraction of crown and roots;
- antiseptic treatment;
- applying a bandage;
- suturing.
Classification of the disease
Due to the occurrence
- Primary (idiopathic) trigeminal neuralgia. A classic type of neuralgia, so to speak. Occurs due to compression of the trigeminal nerve.
- Secondary trigeminal neuralgia is a consequence of other diseases and viruses.
By coverage
- Unilateral (one branch of the trigeminal nerve is affected).
- Bilateral (more than one branch is affected).
Neuralgia can affect the 1st, 2nd, 3rd branches of the trigeminal nerve. The first branch is responsible for the orbital zone, the second for the median zone (including the nose and upper lip), and the third for the lower jaw. Most often, damage to the third branch is diagnosed, so the pain affects the area of the lower jaw, and an attack often occurs during hygiene, eating or shaving.
Types of trigeminal neuralgia
There is an additional classification that can also be used in making a diagnosis.
Acute
Acute trigeminal neuralgia, accompanied by frequent and severe attacks.
Chronic
Chronic trigeminal neuralgia is a consequence of an untreated disease. The patient has been observed for a long time: remissions alternate with exacerbations.
Atypical
Atypical trigeminal neuralgia occurs against a background of stress and nervous exhaustion (psychosomatics).
Postherpetic
Postherpetic trigeminal neuralgia occurs after a history of herpes and its symptoms differ from the classic type. The pain is usually burning and may not go away for two to three hours.
Why paresthesia needs to be treated
Some patients whose symptoms are mild refuse treatment. They get used to living with a numb part of their face and do not want to devote time to long-term treatment measures. You can't do that.
The fact is that in the absence of the necessary therapy, the entire sensitive part of the nerve can be affected. Then the sensitivity of a separate part of the face will be lost completely and forever. Therefore, in order to avoid such a complication, you must definitely consult a dentist if paresthesia does not go away on its own.
Diagnosis of the disease
Modern medicine has in its arsenal many diagnostic techniques that make it possible to determine the type of neuralgia and the cause of its occurrence:
- visual examination and questioning of the patient;
- X-ray of the jaw;
- MRI of the brain and blood vessels;
- laboratory analysis of urine and blood;
- electromyography.
Diagnosis is carried out by a neurologist, but additional examinations by other specialists are often required: dentist, ophthalmologist, otolaryngologist. Particular attention is paid to differential diagnosis, since neuralgia may resemble other diseases in its symptoms, in particular glaucoma, otitis media, ethmoiditis, Slader syndrome, etc.
Preparing for surgery
Before removing a wisdom tooth in the upper jaw, the doctor prepares the patient for the upcoming operation. The preparatory process consists of:
- X-ray examination of the problematic tooth;
- clinical examination of the patient for the presence of pathologies and other concomitant diseases that may affect the course of the operation;
- removal of subgingival and supragingival deposits from the tooth being removed and adjacent teeth to prevent the penetration of infected plaque into the alveolus.
The surgeon also assesses the patient’s psycho-emotional state and, if necessary, recommends taking a sedative.
Treatment of trigeminal neuralgia
Treatment and drugs
For successful treatment, complex drug therapy is used. First of all, these are anticonvulsants (carbamazepine, finlepsin or clonazepam), which are included in the mandatory rehabilitation program and relieve the main manifestations of neuralgia. The dosage and duration of treatment are determined strictly by the attending physician.
For additional effect, antihistamines and local pain relievers may be prescribed. To compensate for the lack of gamma-aminobutyric acid (a kind of mediator between the brain and the nervous system), baclofen, phenibut or gabapentin are prescribed. In the stage of exacerbation of neuralgia, specialists often prescribe antidepressants to eliminate psychological discomfort (the most common remedy is finlepsin). If the cause of the disease is a virus or infection, antiviral and antibacterial agents, as well as NSAIDs, are prescribed. During the recovery period, it is recommended to take B vitamins.
Physiotherapy
To eliminate pain, novocaine blockades and sodium hydroxybutyrate injections are actively used. The most popular and effective physiotherapeutic techniques: acupuncture, ultraphonophoresis, magnetic therapy, and low-frequency laser therapy. Massage for trigeminal neuralgia is also a good addition to general treatment and allows for better blood circulation.
Reasons and indications for removal
Dentists determine a list of indications for tooth nerve removal:
- caries in an advanced form (after the destruction of enamel and dentin, bacteria reach the pulp and gradually destroy it. If you go to the clinic in a timely manner, the doctor will not remove the nerve. The only thing the patient has to go through is cleaning the tissues affected by the pathology and filling the canal);
- tooth trauma (despite the most common trauma to the front teeth, premolars and molars often suffer from falls or impacts);
- infection entering the pulp by destroying the apex of the root unit.
Upcoming prosthetics is also a reason to remove the nerve. If more than 75% of the tooth is destroyed, the pulp is completely removed. This precaution indicates the high professionalism of the dentist, since the unremoved pulp under the metal-ceramic crown will overheat and cause quite painful sensations. Removing the nerve (tooth depulpation) under the crown is a more expensive and problematic procedure. It would be more reasonable to prevent this complication from occurring.
Often patients do not want to re-visit a dentist who made a mistake during prosthetics. Our specialists often encounter a problem that arose due to the fault of colleagues from other clinics.