According to statistics, the inferior alveolar nerve (IAN) suffers quite often during implantation.
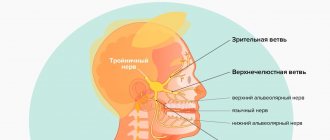
The nerve passing in close proximity to the inferior alveolar process is part of the trigeminal facial nerve, which is responsible for the sensitivity of the facial muscles. Disruption of this nerve during implantation 15-20 years ago was considered a common phenomenon. However, in modern dentistry, the equipment used makes it possible to reduce the risk of damage to the NAS.
Statistics say that only 3% of patients experience a postoperative complication in the form of disruption of the lower branch of the facial nerve. But dental practitioners are sure: more than 30% of people become victims of neuropathy, while about 15% of patients remain with this diagnosis forever.
Causes
The NAN is damaged not only during the installation of implants, but this is the main reason. In addition to unsuccessful implantation of an artificial root, the nerve suffers in the following cases:
- extraction of incorrectly located wisdom teeth in the lower row;
- penetration of the composite material into the canal with the nerve;
- improperly performed conduction anesthesia.
Infectious diseases and inflammatory processes with suppuration also often threaten the integrity and full functionality of the inferior alveolar nerve.
Injury Prevention
Prevention is high-quality preparation for surgery and professional performance of manipulations. A thorough study of the structure of the patient’s mandibular canal, the parameters of the alveolar process and the topographical position of the nerve fiber prevents neurological complications.
For this purpose the following are assigned:
- orthopantomogram;
- computed tomography - 3-dimensional scanning.
Complications will be avoided:
- correct formation of the implant bed;
- careful implantation of the dental structure;
- lateralization (change in the position of the nerve) when it is close to each other.
Alarms
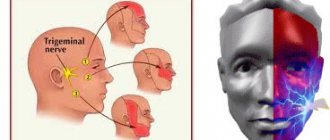
The first signs of NAS damage are discomfort in the innervation zone (lower lip, cheek and gums in the lower jaw). There are 3 types of manifestations of the disease:
- anesthesia (absolute loss of sensation);
- dysesthesia (discomfort in the form of “pins and needles”, pain in the area of the affected NAS);
- paresthesia (decreased sensitivity: the patient does not feel pain when pricked with a needle).
Often, when removing figure eights, the lingual nerve is damaged. Sometimes this happens during implantation. Signs of the disease:
- uncontrolled tongue biting;
- violation of diction;
- decreased performance of taste buds;
- increased salivation.
Note: up to 90% of lingual nerve injuries do not require drug treatment. The pathology disappears on its own after 1.5-2 months.
What methods are used in treatment
The treatment method depends on the extent of the lesion and is carried out after assessing the sensitivity deficit. With neuropraxia, recovery occurs on its own within 4-6 weeks . No medical attention is required since the nerve structure is not damaged.
With partial degeneration, symptoms subside two months after the injury. For a complete recovery, medical measures will be needed. Numbness for 9-12 months is dangerous due to irreversible degeneration of nerve cells . Microsurgical treatment can be urgent (for an open injury) or planned (for a closed injury).
Treatment tactics for closed injury
- For numbness that does not go away for three months - suturing, transplantation;
- For dysesthesia (perversion of sensitivity) for more than 3 months - revision, decompression, neurolysis, suturing and nerve transplantation;
- If hypoesthesia (decreased sensitivity) lasts for more than 3 months, partial unscrewing or removal of the structure, revision, transplantation, suturing is indicated.
Drug treatment
Indicated for chronic nerve inflammation syndrome. An important point is pain relief. Can be used:
- Antineuralgic drugs:
- Carbamazepine;
- Phenytoin;
- Baclofen.
- Antidepressants:
- Amitriptyline;
- Imipramine.
- Local products:
- ointments with capsaicin;
- acupuncture;
- electrical stimulation;
- physiotherapy.
Classification and diagnosis of pathology
Facial nerve injuries are divided into the following types:
- neuropraxia (cured in 3-5 weeks);
- axonotmesis (moderate nerve damage, requiring up to six months of therapeutic treatment);
- neurotmesis (irreversible changes in the structure of nerve fibers. Cannot be treated with medication. Surgical intervention is required).
This neurological pathology is diagnosed using two methods:
- mechanoceptive (brush test - the patient is carried out on the lip, and the patient says the direction of movement and irritation with two points - a device resembling a mathematical compass is applied to the lower part of the face. In this case, the distance between the legs of the device is constantly increasing. As soon as the patient stops feeling each injection separately, the result is recorded and the degree of nerve damage is determined);
- nociceptive (pin prick, temperature test).
Taste buds are tested by dipping a cotton swab in salty or sweet water.
Treatment
Pain in the area of the inferior branch of the trigeminal nerve requires the use of 3 treatment methods.
Drug therapy. The doctor prescribes blockers and painkillers to reduce symptoms. The dentist will also recommend anti-inflammatory therapy. This treatment usually lasts 5-7 days.
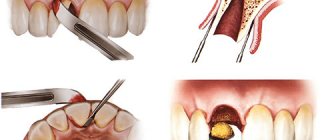
Removing the artificial root. 1-1.5 days after implantation of the rod (if symptoms occur), dentists recommend immediately removing the implant, since such a decision increases the chances of a favorable outcome of therapy. Further treatment is carried out with medication.
Surgical intervention. Indications for a radical method are considered to be the failure of removal of the implant and treatment with medications.
Important! Removing the implant is not always the key to successful treatment of the nerve, but this action increases the chances of a quick recovery and reduces the risk of tumor formation in the area of the nerve bundle.
Treatment tactics are agreed upon with the patient, who signs consent for the operation.
Predictions and prevention
| Click to sign up for a FREE consultation |
Neuropraxia and axonotmesis are quite treatable. Statistics show that more than half of patients completely cure the disease. With neurotmesis, complete recovery does not occur.
Dentists call the main preventive measure a comprehensive study of the performance of the dental system before implantation. At the diagnostic stage, the doctor finds out the exact location of the nerve. This helps to avoid injury to the “twig”.
An experienced dentist will definitely analyze CT and X-ray data, compare the results and draw up an implantation plan based on the individual structural features of the patient’s lower jaw.
The implant is screwed in carefully; its final position should be no closer than 2 mm to the nerve process.
Symptoms of the lesion
You can assume that the mandibular nerve is affected by the following signs:
- numbness of the face from the implantation side: lower lip, chin, tongue, lower teeth, cheeks;
- pain in the implant area;
- the appearance of profuse salivation;
- choking when eating or drinking;
- the occurrence of facial expression and articulation disorders.
A person feels discomfort when caring for facial skin (unpleasant sensations during shaving, applying makeup). Clinical manifestations depend on the type of injury and the depth of the lesion.
Nadent – Natalia Khvorostinova’s Universal Dentistry in Moscow
Medical tactics for injury to the mandibular nerve after dental implantation
Lungu Valery Ivanovich, Ph.D., Georgiev T.D., Ph.D.
Odessa State Medical University named after. N.I. Pirogov, department surgical dentistry (head - prof. Gulyuk A.G.)
Among a number of factors of “failure” in implantology, that is, the occurrence of “complications”, in second place after perforation of the maxillary sinus is, according to A.V. Kamalyan (2007), perforation of the mandibular canal (from 20 to 30%). Considering the fact that dentures on implants have become widespread, the patient hopes and demands high quality of this type of treatment. Hence, the prevention of possible complications is of particular relevance and is increasingly becoming a matter of concern for implantologists [1].
There is still no consensus on the effectiveness of methods for eliminating tissue paresthesia in the area of the mandibular nerve after installing implants in the lateral mandible. V.L. Paraskevich (2004) indicates two reasons for the occurrence of this complication: mechanical compression of the nerve during the formation of an intraosseous hematoma or edema in the bone tissue, as well as direct damage to the neurovascular bundle passing in the mandibular canal [2]. Understanding the mechanism of development of complications associated with mechanical compression of the inferior alveolar nerve allows us to conclude that early use of any treatment methods is necessary [3].
Therefore, the purpose of our study was to determine the doctor’s tactics after complications arise during implantation of the lateral mandible.
Materials and methods. The study was conducted at the Department of Surgical Dentistry of OSMU. Started in 2003 and continues to this day. Patients were selected - 16 people who, in the postoperative period, complained of impaired sensitivity in the chin area after surgery to install implants. The patients' age ranged from 26 to 69 years. On the side of the nerve damage, from 1 to 3 implants were installed, depending on the number of lost teeth and the degree of atrophy of the alveolar process. Upon examination, an area of lack of tactile, pain and temperature sensitivity was revealed in all patients. Computed tomography data revealed adherence of the implants to the mandibular canal or perforation of the upper wall of the mandibular canal. However, it should be noted here that most situations were analyzed using an orthopantomogram, where the error in the image is up to 30%.
The area of dysfunction of the inferior alveolar nerve and the degree of impairment were assessed by changes in the boundaries and sensitivity thresholds of the skin of the chin and lower lip on the affected side, comparing with the results of the opposite side.
Results and its discussion. All patients complained of a long-term and persistent disturbance in the sensitivity of the skin of the lower lip, chin, mucous membrane and teeth of the corresponding side that appeared on the day of surgery. It is worth noting that retrograde from the implantation site, all patients noted radiating pain to the ear and temporal region. Traditionally, for this complication of dental implantation, a course of physiotherapy is carried out and vitamin preparations are prescribed. Conservative treatment, regardless of drugs and duration, had no effect in any patient. Relief of the condition was noted after removal of the implant, and the sooner we removed the implant, the sooner the symptoms of discomfort disappeared. The doctor's wait-and-see tactics in the hope of spontaneous restoration of the function of the inferior alveolar nerve turned out to be erroneous.
When the implant was localized in the lumen of the mandibular canal (damage to the artery and nerve), patients noted a sharp decrease in tactile, pain and temperature sensitivity. This indicated a complete loss of nerve function.
When the apex of the implant was localized 1-2 mm from the upper wall of the canal, tactile sensitivity was maintained while pain and temperature were reduced. We believe that this clinical picture is due to compression of the inferior alveolar nerve by postoperative swelling of the cancellous bone layer or hematoma.
Restoration of tissue sensitivity after removal of the implant occurred within a period of 5 to 8 weeks, if the implant was removed no later than 10 days after the onset of paresthesia. In those cases when we adopted an erroneous wait-and-see approach, serious degenerative changes occurred in the nerve, which is still manifested in loss of sensitivity. The area of paresthesia decreased slightly, but nothing more.
Conclusions. By analyzing the results of the study, we allowed ourselves to determine the doctor’s tactics in case of nerve injury. Long-term unsuccessful conservative treatment of patients in the presence of severe dysfunction of the nerve allows us to conclude that it is impossible to eliminate paresthesia without eliminating the cause. In doubtful cases, it is necessary to clarify the location of the implant using computed tomography. If the localization of the implant is confirmed in the lumen of the canal, it is necessary to remove the implant as soon as possible.
Literature.
1. Kamalyan A.V. Criteria for expert assessment of errors and complications during dental implantation (medical and legal aspects): Dis. ...candidate of medical sciences. – M., 2007.
2. Paraskevich V.L. Dental implantology. Fundamentals of theory and practice. – Minsk: Unipress LLC, 2002. – 386 p.
3. Goncharov I.Yu. and others. Treatment of postoperative complications in surgical dentistry. //Dental magazine No. 2, 2009. Minsk. P.185-186
Features of massage for neuralgia
- In the first days of the disease, massage is carried out in a gentle manner with a gradual increase in load in each subsequent session. Carrying out a deep massage is allowed only after the acute symptoms have subsided and the attacks of pain have subsided.
- At elevated body temperatures, massage is contraindicated.
- The effectiveness of the massage increases if it is done immediately after taking a warm shower (bath) or visiting the bathhouse. Before the massage, it is advisable to apply a warming ointment or cream to painful areas.
- It is not recommended to go out into the cold immediately after the session.
MECHANISM OF DEVELOPMENT OF TRIGEMINAL NEURALGIA
The functional and anatomical features of the trigeminal nerve system cause the occurrence of neuralgia during general infections and intoxications, diseases of the teeth and paranasal sinuses, cerebrovascular pathology, narrowing of the infraorbital and mandibular canals, as well as other pathological conditions. The disease usually begins with irritation of the peripheral nerve with further involvement of the entire trigeminal nerve system and with the development of dominance in the thalamus (visual thalamus) and cerebral cortex.< /p>
At a late stage, a persistent focus of pathological activity is formed in the area of the thalamus (visual thalamus), and the pain acquires a very unpleasant emotional overtones, spreading to the corresponding half of the body.
Against the background of a sharp progression of autonomic dysfunctions, the patient experiences unbearable suffering, his character and habits change.
Baths as therapy
Is it possible to go to the bathhouse if you have neuralgia? A visit to the bathhouse is a good way to cope with pain and inflammation due to neuralgia. This is explained by the fact that during the restoration of bone tissue, pinching is also eliminated.
However, to get maximum benefit, it is important to keep a few recommendations in mind:
You can visit the bathhouse only if the sharp pain has gone away; before going to the bathhouse, you should not eat heavily - just have a small snack, since a full stomach creates additional stress on the cardiac system; You need to wash yourself with soap and dry with a towel in advance - this will provide better heating and protect against overheating; the duration of stay in the steam room should not exceed a quarter of an hour, the maximum number of visits cannot be more than three; It is recommended to cool down for no more than 10 minutes, after which you need to take a half-hour break; massage and self-massage will improve blood flow; from the very beginning, set the minimum temperature of the steam room so that the body has the opportunity to adapt; in the steam room, sit straight, do not slouch - this is especially dangerous with intercostal neuralgia; for neuralgia of the neck and occipital nerve in the steam room, it is best to lie down, with a cushion placed under your head; You should not drink alcoholic beverages during steaming; if neuralgia affects the limbs, then you can massage directly in the steam room; For an additional calming and analgesic effect, the use of aromatic oils is recommended - ylang-ylang, basil, geranium, fir and eucalyptus oils help best.
Contraindications for visiting a bathhouse with neuralgia:
- constant pressure surges;
- acute stage of neuralgia;
- inflammatory processes in the body;
- diseases of the cardiovascular system;
- age over 65 years;
- diseases of the respiratory organs.
Editorial: Cervical migraine, its symptoms and treatment
Find out more about treatments for neuralgia:
- medications, including the drug Finlepsin;
- using the Almag apparatus;
- using ointments.
Therapy results
The prognosis of microsurgical and therapeutic treatment is influenced by:
- age, health status of the patient;
- skill and experience of the surgeon;
- the duration of the period between injury and surgery.
In 80% of cases of neurotmesis operated on in the first 5 months after injury, partial restoration of the function of the mandibular nerve was observed. Delaying surgical intervention systematically reduces the chance of recovery. Seeing a neuromicrosurgeon a year or more after injury has only a 10% chance of success.