Selective tooth grinding is a complex treatment method that is used for periodontal diseases. The procedure is used to correct occlusion and articulation on natural and artificial teeth, and allows you to evenly distribute the chewing load on the teeth. This is one of the most common methods in the complex therapy of periodontal diseases, which is used both in the initial and active stages of the pathological process.
Indications
Selective tooth grinding is a complex procedure that requires a strictly individual approach to each patient. In some cases, achieving an ideal ratio is impossible due to the structure of the jaw and individual teeth. In this case, the procedure is carried out in order to get as close as possible to the desired result.
The main purpose of grinding is to create uniform contact throughout the entire dentition, remove excessive load on the jaw and distribute it evenly over all teeth. To do this, hard tissues are ground off from the teeth that come into contact during chewing movements, after which they are aligned with the dentition, on which there are no points of contact.
Main indications for the procedure:
- improper closure of molars;
- increased tone of the masticatory muscles;
- displacement or deformation of the dentition due to injury;
- lack of natural tooth wear;
- abnormalities in the structure of the jaw;
- prevention of periodontal diseases.
In some cases, the grinding method is used to grind down sharp edges of teeth, which injure the tongue and oral mucosa. This saves the patient from minor injuries or damage.
Contraindications
Sanding is not carried out in the following cases:
- During the period of progressive periodontal inflammation. In this case, before the main procedure, the patient is prescribed a course of treatment.
- The patient has been diagnosed with dental anomalies and deformations that require treatment by other specialists (orthopedist or surgeon).
- Acute and chronic diseases of the temporomandibular joint are observed.
The grinding procedure should only be carried out by a qualified specialist. Incorrectly performed correction can lead to displacement of teeth, excessive load on the periodontium due to flattening of the dental tubercle, and removal of one or more teeth from occlusal contact.
How does the procedure work?
The operation is carried out in several stages, with short breaks.
Preparation for the procedure is based on a preliminary visual examination of the patient. Closing the dentition helps to identify points of contact between the dental surface and the arch where this closure is absent. Next, final (more accurate) testing is done using carbon paper to identify all problem areas for further occlusion correction.
Based on the data obtained, zones for grinding are selected. The procedure itself may seem unpleasant, so it is usually carried out under the influence of an anesthetic. A preliminary test for allergic reactions eliminates all negative consequences from the use of painkillers.
The grinding procedure is carried out in three stages:
- At the first stage, a preliminary grinding procedure is carried out in order to eliminate the most pronounced unevenness of the dental surfaces. In case of significant shortening of teeth, mandatory depulpation is carried out.
- Next, the procedure is carried out on other teeth that require correction.
- After final polishing, fluoride-containing polishing pastes are used.
After each stage, treatment is carried out with special preparations that reduce tooth sensitivity.
Main directions
The techniques used in modern dentistry are based on two basic approaches:
- Jenkelson's technique involves determining the occlusal relationship through the efforts of the patient himself, without medical assistance and in a form convenient for him. Abnormally contacting areas are corrected within the framework of central and distal occlusion, while the frontal and lateral areas remain unchanged.
- Schuyler's technique determines the need to correct areas that create articulation problems. The removal procedure involves sequential treatment of distal and central, frontal, and then lateral occlusion, with mandatory manual adjustment of the jaw position.
Possible complications
If the rules for the procedure are not followed, the following complications are possible:
- decrease in interalveolar height;
- tooth displacement;
- hyperesthesia of hard tissues;
- excessive load on the periodontium after flattening the cusps of the teeth;
- removal of some teeth from occlusal contact and overload of the periodontium of others.
Therefore, the procedure can only be trusted to a dentist who has undergone special training and has the appropriate qualifications.
Selective grinding of teeth.
⇐ PreviousPage 8 of 10Next ⇒
The method of selective grinding of teeth involves the correction of functional occlusion by grinding down identified supercontacts on natural and artificial teeth. Grinding can be started only after analyzing the dentofacial system and occlusion, establishing a diagnosis, drawing up a plan for occlusal correction; in difficult cases, diagnostic grinding of teeth is carried out on models of jaws installed in an articulator. The main principle is maintaining or creating a stable occlusion, i.e. the presence of fissure-tubercular contacts of the lateral teeth with minimal removal of hard tissues. If stable occlusion cannot be achieved in this way, then other methods of occlusal correction are chosen
(Fig. 1).
A
FIG 1. Ideal tooth contact (a)
To achieve ideal contact, minor occlusal correction is required
(6)
To stabilize occlusal contacts, significant occlusal correction is required (c) Occlusal stability cannot be achieved by selective grinding of teeth
(d)
To carry out treatment, the patient must be prepared: informed about the purpose of grinding the teeth, about that if there is no effect, other methods of occlusal correction will be necessary. For excited patients, premedication is indicated an hour before treatment. For pain and limited jaw movement, physiotherapy and the use of relaxation splints are recommended.
The goals of selective grinding of teeth can be formulated as follows.
1. Elimination of the traumatic situation in the periodontium by distributing the functional load over as many teeth as possible.
2. Removing trauma to the hard tissues of teeth and pulp.
3. Load distribution along the axis of the teeth.
4. Removing the pathological activity of the masticatory muscles.
5. Elimination of balancing and hyperbalancing supercontacts.
6. Creation of a stable, stable central occlusion.
7. Elimination of occlusion disorders before orthopedic treatment.
8. Restoration of functional occlusion after orthodontic treatment.
9. Prevention and treatment of periodontal pathology, masticatory muscles and TMJ in the period of primary, mixed and permanent dentition.
10. When grinding teeth of complete removable dentures, creating multiple bilateral contacts for all types of occlusion (to stabilize the dentures), while maintaining the cuspal overlap of the lateral teeth (to prevent biting of the cheek mucosa).
Complications as a result of selective grinding of teeth: reduction in occlusal height, orthodontic effect of tooth movement, hyperesthesia of hard dental tissues, excessive load on the periodontium after flattening the cusps of the teeth, removal of some teeth from the contacts and overload of the periodontium of other teeth.
There are centric and eccentric supercontacts. First
observed in central occlusion, in posterior contact position
(central ratio) and on the path of teeth sliding from the posterior contact
positions into central occlusion (“sliding along true central occlusion” (Fig. 2,b),
This also creates stability of the occlusion and the possibility of some free movements of the lower jaw. According to other authors, grinding should lead to the formation of flat fissures for the cusps of the opposing teeth, this provides axial loads on the teeth (Fig. 1.a). Still others believe that it is possible to create both types of tooth contacts.
On the working side, occlusal surfaces of classes 1 and 2 are polished, on the balancing side - class 3 (Fig. 2,b)
A
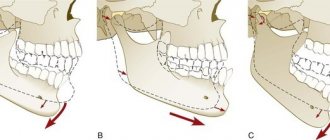
RICE. 2. Grinding should lead to the formation of flat fissures (“stops”) for the slopes of the cusps of the opposing teeth, and the supporting cusp loads the opposite tooth in a direction parallel to the axis of the tooth (“free, planned long” central occlusion according to ( Gross M.D.. Mztyus J.D., 1986); b -
Three-point contact between the cusp and the finsura creates lateral forces on the teeth (“true posterior contact position”).
In the “posterior contact position,” the slopes of the cusps of several teeth should normally be in symmetrical contact. If there are separate slopes of one side in contact, then it is necessary to grind the anterior lingual slopes of the upper premolars and the posterior slopes of the lower premolars so as to obtain bilateral contact of 2-3 pairs of teeth (rule: anterior slopes of the upper teeth, posterior slopes of the lower teeth) .
The sliding contacts are then checked from the “posterior contact position” to the position of maximum tooth contact (habitual occlusion). Those slopes of the tuberosities that interfere with uniform mid-sagittal movements or displace the lower jaw to the side are eliminated. The cusp apices and marginal areas of the teeth must be preserved
Grinding of the slopes of the cusps is carried out in the direction from the gingival edge to the top of the cusp.
The tops of the supporting cusps (upper palatal and lower buccal) are not ground off, because they ensure the stability of the central occlusion and maintain the occlusal height. Protective cusps - upper buccal and lower lingual - are retained, since the former protect the mucous membrane of the cheek, the latter - the tongue from getting between the teeth. The slopes of the cusps, unworn areas of the teeth are ground off, fissures are deepened, and sharp edges are smoothed.
Before grinding off centric supercontacts, which displace the lower jaw into the usual forced occlusion, persons with “articular and muscular” complaints must look at the position of the articular heads on the left and right tomogram of the joint, and analyze the displacement of the heads after treatment. As a result of grinding the teeth, the position of the heads should improve. Otherwise, “super contact” is maintained and the occlusal surface of other teeth is restored. For example, on the working side there is a supercontact that prevents the other lateral teeth and canines from closing. This can be due to a dentoalveolar anomaly or after the manufacture of crowns, bridges (Fig. 3). To avoid grinding off the cusps of the molars, it is possible to create “canine guidance” in lateral occlusion by making a crown on the canine (if it is destroyed or worn out) or applying filling material to the lingual surface of the canine (Fig. 4).
| Rice. 3. Super contact on the molar of the working side, preventing the teeth from closing . |
| .
|
Selective grinding of teeth is carried out over 3-4 visits with intervals between grindings of one week. After each procedure, the teeth are polished and treated with sodium fluoride and fluoride varnish.
It must be emphasized that occlusion disorders can be caused not only by local factors in the oral cavity, but also by joint lesions and dysfunction of the masticatory muscles in general diseases.
When grinding in the posterior contact position, the mandible is first moved distally, until the first light contact of the teeth in the posterior contact position. This contact is marked and ground down until there is even contact at this position on the posterior teeth of both sides.
The goal of occlusal correction is to achieve canine contacts or group contact of canines, buccal cusps of premolars (and molars) in lateral occlusions on the working side on the left and right; in anterior occlusion, it is to create symmetrical contacts of incisors (and canines).
In orthognathic occlusion, Jenkelson's classification of occlusal surfaces is used to diagnose supercontacts. In lateral occlusion, on the working side (the side of laterotrusion), the 1st and 2nd classes of the occlusal surface are ground (external slopes of the buccal cusps of the lower lateral teeth and internal slopes of the buccal cusps of the upper lateral teeth, external slopes of the palatal cusps of the upper lateral teeth and internal ones facing the central fissure is the slopes of the lingual cusps of the lower lateral teeth), and on the balancing side (side of mediotrusion) - class 3 occlusal surface (internal and anterior slopes of the buccal cusps of the lower lateral teeth, internal and posterior slopes of the palatal cusps of the upper lateral teeth) (see Fig. .2 ). On the balancing (mediotrusive side) there can be two options for supercontacts - balancing and hyperbalancing
Balancing supercontacts - occlusal contacts on the balancing side, which in lateral occlusion do not interfere with the closure of the teeth on the working side
Hyperbalancing contacts, unlike balancing contacts, separate the teeth of the working side. In Fig. Figure 5 shows a hyperbalanced supercontact on the right molars, which in the right lateral occlusion interferes with the closure of the working side. Such contacts are observed with elongated wisdom teeth, as well as with crossbite. To determine such contacts, two strips of articulation paper are placed on the lateral teeth on both sides. In lateral occlusion (without strong compression of the jaws), they try to pull out both strips. If the strip is held more on the balancing side than on the working side, then there is an overbalancing supercontact. First of all, overbalancing contacts are eliminated. When reconstructing the occlusal surface, balancing contacts should be avoided. Then the occlusal contacts of the lateral teeth are checked during anterior movements of the lower jaw, grinding the supercontacts on the anterior slopes of the cusps of the lower teeth and on the distal slopes of the cusps of the upper teeth (“protrusive” surfaces of the teeth). In anterior occlusion there should be no contact between the lateral teeth.
FIGURE 5. Hyper-balancing contact on the non-working side, preventing the anterior and posterior teeth from closing on the working side
When the lower jaw moves backward, premature contacts are revealed on the distal slopes of the cusps of the lower lateral teeth and on the anterior slopes of the cusps of the upper lateral teeth (“retrusion” surfaces). When grinding off eccentric occlusal irregularities in the area of chewing teeth, centric occlusal contacts must be preserved. Preliminary analysis of models in the articulator and marking of different contacts with different colors of articulation paper increase the accuracy of selective grinding. If in lateral occlusion on the working side there is contact of the canines and separation of the lateral teeth, then it is necessary, especially with periodontal damage, to stabilize the canine with orthopedic devices.
These rules apply to orthognathic occlusion, and in case of malocclusion and tooth position are limited to improving functional occlusion. With deep incisal overlap, it is almost impossible to adjust the anterior movements. Due to the predominance of vertical movements, it is enough to ensure unhindered lateral displacement within 2 mm with uniform contact of as many teeth as possible on the working side. Normal eccentric occlusion occurs only with orthognathic occlusion. With malocclusions and tooth position, various deviations from normal eccentric occlusion are observed that cannot be eliminated by grinding, and orthodontic treatment in adults is difficult or unacceptable. In these cases, it is enough to improve existing contacts. Our observations show that with intact dentition and dental anomalies, it is sufficient to obtain bilateral symmetrical contacts of the lateral teeth in the lateral
occlusions, symmetrical contacts of the anterior teeth in anterior occlusion.
Not all occlusal disorders lead to dysfunctional symptoms, and therefore indications for occlusal correction are needed. A distinction is made between acceptable and unacceptable occlusion (this applies to cases with normal occlusal height). If there is a decrease in occlusal height, this is an unacceptable occlusion. Occlusion is acceptable if, despite deviations from normal occlusion, there are no dysfunctional symptoms (pain, joint noise, changes in the periodontium of individual teeth, etc.) But if there is even one symptom, for example, horizontal ground areas or impaired movements of the lower jaw (joint noise or pain), then in this case occlusal disorders must be eliminated, since in a stressful situation it is possible that many symptoms may arise or the existing ones will intensify.
In case of malocclusion and tooth position, it is possible to obtain normal eccentric occlusion by grinding. For this purpose, extensive orthopedic reconstruction is carried out, but in the absence of single teeth, this makes no sense. In these cases, it is enough to eliminate eccentric occlusal disorders, having previously found out which of them are acceptable and which are unacceptable.
Bilateral asymmetric deviations from normal eccentric occlusion, as opposed to unilateral deviations, are acceptable.
Bi- and unilateral eccentric occlusal disorders with inclined and elongated teeth, which cause disocclusion of the remaining teeth, must be eliminated both with intact dentition and with iatrogenic disorders.
In the area of the anterior teeth, those supercontacts that are located on individual teeth must be eliminated.
Symmetrical contact of the incisors in lateral occlusions with malocclusions is acceptable. For malocclusions, as a rule, orthodontic treatment precedes selective grinding of teeth
In case of periodontitis that has developed against the background of a deep bite, shortening the frontal group of teeth has the goal of removing blocking areas of the teeth during a sagittal shift of the lower jaw and reducing the separation of the group of chewing teeth during anterior occlusion. Grinding is carried out along the cutting edge and along the contacting surfaces of the teeth when the jaw moves forward. In case of periodontitis, grinding is carried out to remove the concentration of occlusal contacts on individual teeth, and not to exclude them from occlusion. Grinding is carried out under visual control when the lower jaw moves anteriorly, to the right and to the left and is stopped at the first pain. First, the central incisors are shortened, then the lateral and, if necessary, canines. After shortening the teeth, they begin to remove the blocking areas. To do this, articulation paper folded in half is placed between the teeth and, fixing the movable teeth with fingers, the patient is asked to move the lower jaw forward, then to the right and left. Traces of articulation paper remain on the teeth in places of greatest contact. After visually checking these areas during jaw movements, they are ground off. If the paper leaves a uniform mark on all contacting surfaces, and visual inspection confirms the absence of blocking areas, sanding is stopped. All sanded areas are smoothed with a rubber polisher.
When the stage of periodontitis has developed and the teeth are highly mobile, selective grinding is best done after applying a temporary splint.
The final stage is the treatment of the wound surfaces of the teeth. Firstly, they are polished, and secondly, calcium ions are impregnated into them using electrophoresis. Thirdly, they are coated with fluoride varnish or protective coating varnish.
Complications during selective grinding of teeth: decrease in occlusal height, orthodontic effect of tooth movement, hyperesthesia of hard dental tissues, excessive load on the periodontium after grinding of the cusps of the teeth, removal of some teeth from contact and overload of the periodontium of other teeth. Therefore, for the correct use of this method of occlusal correction, it is necessary to know the basics of the biomechanics of the dentofacial system, analyze occlusal contacts in the oral cavity, as well as on diagnostic models, and adherence to certain rules.
Topics studied previously and necessary for the lesson:
1. Anatomy of periodontal tissues.
2. Etiology, pathogenesis, clinic of periodontal tissue diseases.
3. Features of the clinical picture of periodontitis and periodontal disease.
4. Basic orthopedic measures carried out by a doctor in patients with periodontal tissue diseases.
Questions to monitor the results of mastering the material:
1. Purpose of selective grinding of teeth.
2. How is selective grinding planned?
3. What is the final treatment of teeth after selective grinding?
Situational tasks.
1.The patient is 40 years old. He came to the clinic with complaints of difficulty chewing food, pain and bleeding in the area of the lower front teeth. Regularly treated by a periodontist.
Teeth 21 22 21 12 have 1 degree of mobility; there is an increase in the height of the clinical crowns of these teeth due to their protrusion from the alveoli and atrophy of the alveolar process. With articulatory movements and various types of occlusion, supercontacts and blocking of the movements of the lower jaw are observed. To diagnose. Make a treatment plan.
2. A 51-year-old patient came to the clinic with complaints of mobility of the 16th and 11th teeth, pain when eating, and purulent discharge from the gum pocket.
16 has second degree mobility. Give a plan for grinding off blocking areas of the dentition.
3.At the clinic, an orthopedic dentist sees a 57-year-old patient with a complete dentition in the upper jaw and a complete absence of teeth in the lower jaw.
43, 42, 41, 31, 32, 33, have II degree mobility. What should be the tactics of an orthopedic surgeon? Is teeth grinding necessary here? In what case is it necessary to do this?
4.A 38-year-old patient was diagnosed with deep, mildly expressed incisal overlap. Periodontitis of the 1st degree of the frontal group of teeth.
What should be the sequence of actions of a doctor when grinding teeth?
Literature:
1. Gavrilov E.I. Shcherbakov A.S. Orthopedic dentistry. M.,
1984.- p. 296-302.
2. Kopeikin V.N. Orthopedic treatment of periodontal diseases.
M., 1977.- p. 57-77.
3. Kopeikin V.N. Orthopedic dentistry. M., 1988.- p. 298-305.
4. Ivanov BC Periodontal diseases. M., 1981.- p. 159-183.
5. Sugar L et al. Oral diseases. Budapest. 1980.- p.
340-347.
6. Khvatova V.A. Diagnosis and treatment of functional occlusion disorders. N. Novgorod: Publishing house NGMA, 1996.-p. 48-49,163-171.
Practical lesson No. 5
Topic of the lesson: Biomechanical principles and main types of dental splinting.
Purpose of the lesson: to familiarize students with the biomechanical principles of designing splinting devices.
Contents of the lesson.
The assistant introduces students to the basic principles of splinting teeth, reminding them that splinting means combining several or all teeth into a single block with some kind of orthopedic device (splint).
Splinting is aimed at solving the main problems of orthopedic treatment for periodontal diseases (see topic No. 2).
The tire should:
· create a strong block from a group of teeth, limiting their movements in three directions (vestibular-oral, mesiosteal and vertical):
· be rigid and firmly fixed on the teeth;
The tire must not:
· be associated with radical preparation of teeth;
· have an irritating effect on the marginal periodontium and interfere with manipulations in the gingival pockets;
· block the movements of the lower jaw and impair speech;
· have retention points for food retention and disrupt the aesthetics of the patient’s appearance.
E.I. Gavrilov (1984) believes that in order to achieve a therapeutic effect, it is necessary to be guided by the following biomechanical principles:
· restriction of tooth mobility due to the rigidity of the splint, which has a beneficial effect on diseased periodontium;
· unloading of the periodontium occurs due to the normalization of the distribution of chewing pressure;
· unloading of the periodontium with minor damage occurs due to the most stable teeth;
· the splinting structure, located along an arc, is the most rigid due to the arched shape and the mutual intersection of the mobility vectors of the teeth included in the splint;
· with a linear arrangement of the tires in the lateral sections, on the right and left, they must be connected transversely using an arc prosthesis.
⇐ Previous8Next ⇒
Recommended pages:
Use the site search: