7.2.9. Sense organs
Human interaction with the world around him occurs through the senses. A person has five of them in total: eyes (organ of vision), ears (organ of hearing), nose (organ of smell), skin (organ of touch), tongue (organ of taste). Each of the senses reacts to certain environmental stimuli.
| 1 |
| Figure 7.2.9.1. Taste zones of the tongue |
With the help of the olfactory organ, located in the epithelium of the upper part of the nasal cavity, a person can distinguish objects by smell, determine the quality of food and inhaled air. The taste organ makes it possible to determine the taste of food, which a person perceives with the help of special nerve endings located in special formations of the oral cavity - taste buds located on the surface of the tongue. Different parts of the tongue perceive different tastes: the tip of the tongue is sweet, the root is bitter, the sides are sour, the edges and tip are salty.
With the help of vision, a person distinguishes colors, shapes, and sizes of observed objects. The eyes are located in the sockets of the skull. The movement of the eyeballs is provided by muscles attached to their outer surface. With the help of the eyelids, eyelashes and lacrimal glands, the eyes are protected from foreign small particles. The eyebrows located above the eyes protect them from sweat.
The eye has a protein membrane - the sclera, which determines the shape of the eyeball. The sclera passes in front into the transparent cornea. The iris, which regulates the size of the pupil and determines the color of the eye, is clearly visible through the cornea. The inner layer of the eye is called the retina. It consists of photoreceptor cells that look like cones and rods. Behind the pupil is the lens, adjacent to the iris. It has the shape of a biconvex lens. The space between the cornea and the lens is filled with fluid. The eyeball itself is filled with vitreous humor - a transparent mass of jelly-like consistency. There are blood vessels and nerves leading to the eye. Light hitting the retina causes excitation in the nerve endings of the eye - receptors, through which excitation is transmitted to the brain - the cerebral cortex.
| Model 7.7. Myopia and farsightedness |
With the help of the organ of hearing, a person gains the opportunity to perceive various sounds of the surrounding world, thanks to which he can navigate the environment. The hearing organ consists of the outer, middle and inner ears.
The outer ear consists of the pinna, auditory canal and eardrum. The Eustachian tube and three small bones - the malleus, incus and stapes - belong to the middle ear. Finally, the inner ear consists of a complex system of interconnected canals and cavities, reminiscent of a cochlea. The cochlea contains fluid and nerve endings. The auditory nerve connects the inner ear directly to the brain.
The sense of touch arises in humans thanks to the skin. The skin, especially in the fingers, palms, soles, lips, etc., contains a large number of nerve endings, which ensures their increased sensitivity. Skin sensitivity is divided into four types: pain, tactile (touch and pressure), cold and heat. Impaired skin sensitivity may be associated with a disease of the internal organs. With the help of the skin, a person is protected from mechanical influences (shocks, pressure, etc.), as well as from ultraviolet radiation.
Impaired sense of smell and taste is one of the most common symptoms of the new coronavirus infection. Changes in chemosensory function occur in the early days of the disease and may be the only symptom of COVID-19. Among the European population, olfactory dysfunction associated with COVID-19 occurs in 60–80% of cases, in East Asians - in 30%.
Elena Malets, scientific secretary of the research department of the Republican Scientific and Practical Center of Otorhinolaryngology, candidate of medical sciences. SciencesEtiopathogenesis
Smell impairment can develop in conductive and neurosensory types. Conductive dysosmia occurs due to swelling and inflammation of the nasal mucosa, accompanied by blockage of the olfactory cleft.
However, with COVID-19, this variant is rarely observed; the most characteristic is the neurosensory mechanism of dysosmia. SARS-CoV-2 infects the supporting cells of the olfactory neuroepithelium, on the surface of which receptors for angiotensin-converting enzyme type 2 (ACE2) are located. After the spike protein binds to the ACE2 receptor, the virus enters the target cell by endocytosis using a type 2 transmembrane serine protease.
Receptor cells of the olfactory neuroepithelium do not contain ACE2; disruption of their functioning and damage to cilia occurs due to the death of supporting cells that perform protective and trophic functions. The role of ACE2, found on the cell membranes of the epithelium of the oral cavity and tongue, in impaired taste sensitivity in COVID-19 has also been proven.
Another molecular cellular mechanism of chemosensory disorders is also possible, due to the glycoprotein neuropilin-1, which is a potential receptor for coronavirus and is expressed in large quantities on neurons and endothelial cells of the capillaries of the olfactory bulb and olfactory tract (I pair of cranial nerves).
The involvement of the olfactory bulb in the pathological process was confirmed by magnetic resonance imaging data of the brain in patients with COVID-19: at the beginning of the disease, accompanied by anosmia, an increase in the volume of the olfactory bulb was noted and a significant decrease by the time the patient recovered and the olfactory function was restored.
Isolated damage to cranial nerves due to penetration of SARS-CoV-2 through the blood-brain barrier damaged as a result of a cytokine storm is currently being actively discussed. This may also explain the taste disturbance that develops as a result of damage to the taste fibers of the glossopharyngeal nerve (IX pair) and the chorda tympani, a branch of the facial nerve (VII pair).
Modern literature describes two mechanisms of smell: orthonasal and retronasal. The first mechanism is realized during normal nasal breathing, when air passes in a linear flow through the lower nasal passage. The retronasal mechanism is observed during the act of swallowing, followed by reflex exhalation. The exhaled air, together with the odorous substance, penetrates the olfactory cleft through the nasopharynx and choanae. The latter mechanism explains taste disturbances in many patients with coronavirus infection.
Clinical picture
Impaired sense of smell and taste (ICD-10: R 43) associated with COVID-19:
- anosmia - complete loss of smell;
- hyposmia - reduced ability to smell;
- parosmia - perverted perception of smells;
- phantosmia - sensation of smell in the absence of a stimulus;
- ageusia - complete lack of perception of taste sensations;
- hypogeusia - weakening of taste sensations.
Often, a violation of the sense of smell in 70–80% of cases is accompanied by a violation of taste, but can occur as a monosymptom. Isolated taste disturbance without olfactory dysfunction in COVID-19 is extremely rare (about 5–15%). Olfactory dysfunction in COVID-19 in 70–80% of patients occurs in the form of anosmia, hyposmia has been confirmed in 20–30%. Phenomena such as difficulty in nasal breathing and runny nose are not typical for COVID-19.
International associations of otolaryngologists urge that the sudden onset of loss of smell and/or taste be considered a specific diagnostic criterion for COVID-19 disease. It is argued that the first identified olfactory disorders during the COVID-19 pandemic are sufficient grounds for self-isolation of the patient and the mandatory use of PPE by both the patient and health care workers. Also, the importance of smell and taste sensitivity for the patient should not be underestimated, since chemosensory dysfunction not only reduces the quality of life, but can also lead to severe neurological and neuropsychiatric complications (for example, depression, cognitive impairment, etc.).
In most cases, restoration of olfactory function occurs spontaneously within one month during treatment of the underlying disease. No additional treatment measures are required.
60–70% of patients with COVID-19 note an improvement in their sense of smell on the 8–9th day of the disease; in 80–90%, complete recovery is observed by the 15th day. And only 10–15% of patients are forced to seek medical help from an otolaryngologist due to the lack of smell and/or taste for more than 20 days. The presented time data for the restoration of olfactory function are explained by the pathophysiological mechanisms occurring in the olfactory epithelium under the influence of SARS-CoV-2. Stem cells provide regeneration of supporting cells by the 7th day of the disease, and restoration of cilia of receptor cells is noted on the 8th–9th day.
Full functioning of the olfactory neuroepithelium becomes possible on the 15th day from the onset of the disease. It is assumed that long-term anosmia (more than 15–20 days) is due to possible damage to the olfactory receptor cells themselves, the natural recovery period of which can take up to 2 months.
The mechanism of smell impairment in COVID-19.
Diagnostics
Considering the high workload of the healthcare system, at the initial stage of diagnostic activities it is recommended to actively use the capabilities of modern telemedicine. The American Academy of Otorhinolaryngology and Head and Neck Surgery recommends remote assessment of olfactory function and taste sensitivity using online questionnaires that take into account the duration of the disease, the date of manifestation of the smell and/or taste impairment and its duration, comorbidities, and risk factors for anosmia/ageusia.
Such questionnaires must be supplemented with a questionnaire to assess the quality of life of a patient with olfactory impairment (Questionnaire of olfactory disorders-negative statements of patient) or its short version. The resulting sum of points allows us to make assumptions about the degree of violation. For the purpose of subjective assessment of chemosensory dysfunction, it is possible to use visual analog scales on which the patient notes the level of his sense of smell and taste sensitivity. The patient’s self-assessment of olfactory and gustatory disorders is subjective, but ensures timely collection of information.
At the next stage, after discharge from an infectious diseases hospital and/or termination of self-isolation, if the result of a PCR test for coronavirus is negative, when the patient contacts an otolaryngologist offline, it is necessary to perform a standard examination of the ENT organs and an endoscopic examination of the nasal cavity with targeted visualization of the upper nasal passage and olfactory fissure. If diseases of the paranasal sinuses are suspected, it is necessary to include a CT examination of the paranasal sinuses in the diagnostic complex. In the absence of pathology of the nose and paranasal sinuses (for example, allergic rhinitis, nasal polyposis, acute or chronic rhinosinusitis, neoplasms of the nose and paranasal sinuses), the study of olfactory function is supplemented by olfactometry.
Olfactometry involves the use of psychophysical tests with a set of odorants (odorants) to determine the acuity of smell and the patient’s ability to distinguish and identify odors. The most popular psychophysical ratified and standardized tests of orthonasal olfaction, with high diagnostic value, are the Sniffing' Sticks Test and the University of Pennsylvania Smell Identification Test (UPSIT).
The sniffing stix test is a reusable portable test, which is a set of 8 tubes with different odorants and 4 tubes with different tastes. This test is aimed at determining all three indicators of olfactory function. UPSIT only measures the ability to identify odors. To perform UPSIT, certified single-use kits are used, produced in the form of booklets and consisting of 40 microencapsulated odorants. The smell is released by rubbing a pencil on paper, the patient identifies the smell and marks the correct answer from the four options given. Less than 18 correct answers indicate the patient has anosmia.
It is important to remember that in order to determine olfactory impairment in patients, it is not recommended to use ammonia and acetic acid, since they act on both the olfactory and trigeminal nerves, which will complicate the diagnosis of true olfactory dysfunction.
To assess taste sensitivity, specially made strips impregnated with various tastes can be used, which are applied to certain areas of the tongue. For example, to determine the perception of sweetness, a strip with a sweet taste is applied to the anterior third of the right and left halves of the tongue and to the anterior third of its lateral surfaces. Sensitivity to sour taste is determined at the root of the tongue. To bitter - on both halves of the back third, to salty - on the entire surface of the tongue.
Also for this purpose, in Europe, otorhinolaryngologists use standardized valid tests consisting of 4 solutions with different tastes and concentrations of substances, which can be easily prepared in normal outpatient settings: table salt solution (30 g per 1 liter of distilled water), sugar solution (30 g per 1 liter of distilled water), a solution of 100% lemon juice (90 ml per 1 liter of distilled water), unsweetened coffee concentrate.
All of the above methods for diagnosing chemosensory disorders are subjective.
Objective methods include the following:
- electroencephalogram (EEG) - additional stimulation of the olfactory and trigeminal nerve allows you to register the reaction of general excitation on the EEG:
- registration of olfactory evoked potentials on the EEG in response to additional intranasal olfactory stimulation;
- registration of dependent negative variation (negative shift of the curve) of the EEG in anticipation of an olfactory stimulus;
- electroolfactography - allows you to measure and record the electrical potentials of the olfactory epithelium;
- registration of taste evoked potentials.
After carrying out the described diagnostic measures, it is possible to verify the violation of the patient’s olfactory function and/or taste sensitivity and prescribe treatment.
If there is no positive dynamics during the 1st month of treatment, a consultation with a neurologist should be included in the diagnostic algorithm.
A neurologist may recommend an MRI of the brain to rule out structural pathology. Also, using special computer programs, it is additionally possible to perform 3D reconstructions of MRI images in order to improve the visualization of the olfactory bulb and measure its volume.
Treatment options
It is necessary to conduct an explanatory conversation with the patient about the need to eliminate unfavorable factors that will slow down the healing process. The patient should avoid dust, smoke, be sure to humidify the air (to prevent dryness of the nasal mucosa), not be exposed to sudden temperature changes (avoid visiting the pool, especially with chlorinated water), and also give up smoking, strong alcohol, consumption of fatty and spicy foods, etc. including hobbies with keto diets.
The doctor must warn the patient about the danger of lack of smell and/or taste, and the patient must ensure an adequate level of personal safety: promptly maintain smoke and gas detectors, monitor expiration dates of food products.
Treatment of patients with impaired sense of smell and taste should begin 2 weeks after the onset of the disease to avoid long-term complications and the development of persistent anosmia/ageusia.
According to recent studies, high effectiveness of treatment of COVID-19-associated olfactory dysfunction was achieved only with olfactory training. Drug support is auxiliary.
Olfactory training is independent regular (6-8 training sessions per day) inhalation of aromatic odorous substances through the nose. Sets of odorants can be compiled arbitrarily, but usually at least 4 varieties of essential oils are used (for example: rose, eucalyptus, lemon, clove). They are applied to a cotton pad to avoid spillage.
The duration of aroma training is from 1–3 months or more. After 3 months, it is recommended to change the composition of the odorant set, use essential oils with other scents (for example: green tea, bergamot, rosemary, gardenia or cinnamon, vanilla, orange, banana). The pathophysiological mechanism for improving the sense of smell during training is associated with an increase in the regenerative capacity of olfactory neurons in response to stimulation by odorants
Considering the etiopathogenesis of this pathology, the main vector in treatment is aimed at neuroprotective therapy using the following drugs:
- Ipidacrine hydrochloride is a reversible cholinesterase inhibitor. The drug directly stimulates the conduction of impulses in the neuromuscular synapse and in the central nervous system due to the blockade of potassium channels in the membrane. Dosage regimen: 1 tablet (20 mg) 3 times a day for 1 month.
- Thioctic (α-lipoic) acid (thioctacid) is an endogenous antioxidant that protects the cell from the toxic effects of free radicals arising in metabolic processes; increases the concentration of the endogenous antioxidant glutathione, which leads to a decrease in the severity of symptoms of polyneuropathy and improves neuronal trophism. Dosage regimen: 1 tablet (600 mg) 3 times a day for 1 month.
- Omega-3 is a dietary supplement containing salmon oil concentrate (1,000 mg) and polyunsaturated fatty acids (eicosapentaenoic acid 180 mg, docosahexaenoic acid 120 mg). Omega-3 accelerates neuroregenerative processes, potentiating the effect of olfactory training. Dosage regimen: 1 tablet (1,400 mg) 3 times a day for 1 month.
- Vitamin D may prevent nerve loss in COVID-19 by stimulating the expression of neurotrophins such as nerve growth factor (NGF). Dosage regimen: 500 IU in multivitamin complexes 1 time per day for 1 month.
- Vitamin A (systemic and intranasal) may have a positive effect in the treatment of olfactory disorders. Thanks to its antioxidant properties, it promotes the regeneration of the olfactory neuroepithelium and potentiates the effect of olfactory training.
- Intranasal corticosteroids have worked well in the treatment of post-Covid anosmia associated with nasal symptoms. The issue of using systemic corticosteroids for COVID-19-associated olfactory dysfunction remains controversial. Some international publications indicate that patients who received systemic corticosteroids for the treatment of coronavirus pneumonia to prevent cytokine storm and severe respiratory failure recovered their sense of smell faster than those who were not prescribed such therapy. But it should be borne in mind that patients receiving basic therapy with inhaled, intranasal and/or systemic steroids for bronchial asthma, allergic rhinitis and/or polypous rhinosinusitis should continue treatment as usual.
- Medicines based on ginkgo biloba provide an antioxidant effect and indirectly help restore olfactory function.
- Medicines containing zinc. Zinc is actively involved in cell proliferation, promoting the regeneration of olfactory receptors.
At the current stage of development of the pandemic, there is no large evidence base confirming the effectiveness of these medicines. However, their use in the treatment of disorders of smell and taste sensitivity associated with COVID-19 is possible.
The lip is not a fool, the tongue is not a shovel: how our taste buds work
Generally speaking, most people fall into one of three categories: non-tasters, tasters and super-tasters - in an approximate percentage ratio of 25:50:25. There is also a special category - super-supertasters, the so-called people with “absolute taste”, and there are very few of them - less than 5%. Supertasters are mostly women, and people of European descent are the least likely to fall into this category.
So who are these supertasters? You might think that such people enjoy food and drink more, but in fact the opposite is true. Supertasters sense taste more intensely than representatives of the first two categories: the impact of different tastes on their tongue may be too pronounced. Things are even worse for super-supertasters. When it comes to taste, “more is not better.”
The best way to describe the differences between these categories is to explain how each of them reacts to my favorite drink: beer. To evaluate the taste of beer, the so-called taste wheel of the American Society of Brewing Chemists is usually recommended.
The Wheel of Taste was created by one of the authors of the book Sensory Evaluation Techniques, which was first published in the 1970s and has now gone through five editions. Morten Meilgaard, an expert on feelings and their measurement, created a taste wheel to quantify beer tasting.
The wheel of taste is not a simple one, it has undergone many changes since Meilgaard came up with it, and focuses on the complexity of beer perception. Examples of over a hundred possible categories include grapefruit, caramel, barnyard, smelly socks, burnt rubber, and baby burp (I hope I don't get to try the latter ones).
These flavors are the result of many factors, but they all come from very simple ingredients in the beer. By the way, to protect this simple composition, in 1516 the Germans passed the Bavarian Beer Purity Law, or Reinheitsgebot, which prohibits calling a drink that contains anything other than hops, water and barley “beer.” Yeast is also necessary in brewing, but five hundred years ago microorganisms were clearly not considered an ingredient.
So, the modern concept of the taste of most classic beers was born from just four ingredients. The most interesting aspect of beer's flavor, at least for me, comes from hops and sugar, and, of course, alcohol, a fermentation product produced by yeast from plant sugars.
Beer is an ancient drink, known since the Neolithic era, but hops have been used in brewing for only a thousand years. Over the past eight hundred years, its use has spread throughout the world, and hops finally gained a foothold in brewing technology with the invention of India pale ale (IPA) in the early to mid-19th century.
Nowadays, due to the abundance of microbreweries and craft beers on the market, many varieties of IPA have appeared, resulting in a huge range of flavors for this drink. It's interesting to note that hops were originally used as a preservative for beer, and the bitterness they impart is just a side effect.
Today, hops are a staple ingredient in craft beer, leading to some pretty interesting varieties (all of which I enjoy immensely, which puts me in the category of casual taster).
Supertasters find beer too bitter, so bitter that they avoid drinking hoppy beers like IPAs, and aren't likely to like more mild beers like most lagers. Personally, I don’t feel the heat of alcohol in beer, and a supertaster will grimace after the first sip: strong drinks are contraindicated for such people - no, no.
Non-tasters are able to drink and eat anything, so they are absolutely tolerant of the taste of hops. But they probably won't be able to tell the difference between Columbia hopped and Cascade hopped bottles. Supertasters will likely be able to handle the task and taste the difference, but if drinking beer is new to them, the first thing they will notice is the extraordinary bitterness of these two varieties. But ordinary tasters get all the shades of hop flavor.
None of this means that supertasters and nontasters alike can't enjoy alcoholic beverages. A non-taster can easily drink tequila with jalapenos, while a super-taster can learn to drink beer or wine and even enjoy it. It is believed that top chefs are supertasters who have trained themselves to overcome the oversensitivity of their taste buds and use their ability to create new dishes.
Surface of the tongue
The shape and position of the tongue change depending on its functional state. At rest, the tongue looks like a shovel (Fig. 1). It consists of an apex, or tip, adjacent to the front teeth, a body and a root, through which the tongue is attached to the lower jaw and hyoid bone. The convex upper surface of the tongue faces the palate and is called the dorsum; on the sides it is limited by the edges of the tongue.
Looking at our tongue in the mirror, we will see only its anterior section (approximately 2/3), the back third of the tongue is located almost vertically and faces the pharynx. On the border between the anterior and posterior sections of the tongue there is a border groove in the shape of an inverted letter V, at the top of which there is a so-called blind foramen (the remnant of a tubular outgrowth associated with the thyroid gland during development). The back of the tongue bears a longitudinally running median groove, which, going deep into the thickness of the tongue, forms a partition dividing the tongue into two symmetrical halves. Both grooves - the border and the median - represent traces of the fusion of individual rudiments from which the tongue is formed in the embryo. Disruption of the process of fusion of the rudiments of the tongue during the prenatal period of development leads to the occurrence of deformities: splitting of the tongue or the appearance of an “additional tongue.”
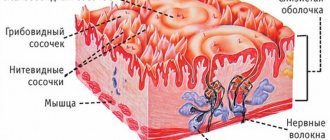
Scattered among the filiform papillae are a few but larger fungiform papillae. They are clearly visible in the form of reddish dots due to translucent blood capillaries. Along the edges of the tongue lie leaf-shaped papillae in the form of several parallel folds. The largest groove-shaped papillae, numbering from 7 to 12, are located on the back of the tongue along the border groove separating the body and the root of the tongue. The grooved papillae are surrounded by a ridge, which is separated from the papilla by a groove - the groove (hence the name).
The mushroom-shaped, leaf-shaped and grooved papillae contain the so-called taste buds - they perceive taste. The surface of the tongue has a rough appearance due to special formations - the papillae of the tongue (Fig. 2). The smallest and most numerous - filiform papillae - are scattered throughout the back and along the edges of the tongue. These brush-like papillae are covered with stratified squamous keratinizing epithelium, the desquamating scales of which are whitish in color, resulting in a whitish-pink tongue. In case of digestive disorders, the rejection of keratinized cells is delayed and a white coating (“coated tongue”) appears on the tongue. The filiform papillae help retain food on the tongue and function as organs of touch: they perceive touch, pain, temperature, but do not participate in the recognition of taste.
The root of the tongue, not visible in the mirror, is covered with a cluster of lymphoid nodules (follicles) that form the lingual tonsil. Together with other tonsils located in the mucous membrane of the oral cavity and pharynx, it performs a protective function - it prevents foreign substances (pathogenic microorganisms) from entering the body and thus participates in providing immunity.
The lower surface of the tongue is smooth, but the mucous membrane forms folds here. A vertical fold runs from the tip of the tongue to the floor of the mouth - the frenulum of the tongue. On the sides of the frenulum below, a small paired elevation is noticeable, on which the excretory ducts of the submandibular and sublingual salivary glands open. Outward from the elevation on each side stretches a transverse sublingual fold, resulting from the sublingual salivary gland located here (Fig. 3). It should be noted that some drugs can be quickly absorbed into the blood through the mucous membrane of the oral cavity. This method of using them is called sublingual (“under the tongue”). This is how they take, for example, validol.