There are a wide variety of dental diseases that damage the health of the teeth and oral cavity. Some pathologies - for example, primary caries - can be treated quickly and even without drilling the tooth; therapy for other diseases requires a whole course of procedures. For example, the treatment of periodontitis is always a complex process, since the disease affects not only the tooth itself, but also the tissues located next to it, which has a negative effect on the body as a whole.
If periodontitis develops to a certain stage, then all therapeutic measures may turn out to be useless and there will only be one way out - to remove the tooth. We will talk in detail about what periodontitis is, its forms, symptoms, and treatment methods in the following sections of the article.
Periodontitis: how does the disease appear and how does it develop?
Periodontitis is a term dentists use to refer to an inflammatory process that affects the tissues that surround the tooth and help keep it in the socket. The causes of periodontitis may vary in etiology (origin) and the disease is classified into subtypes. Correct diagnosis of the subtype of periodontitis is of fundamental importance: on its basis, the specialist will select the most effective treatment methods. Below we will get acquainted in detail with the forms of the disease, and also consider in detail their characteristic symptoms.
Infectious periodontitis
Dentists have to treat the infectious form of periodontitis in 90% of cases. The disease appears due to infection entering the root canals of the tooth and usually against the background of caries or pulpitis, the timely treatment of which was ignored. Infection in the canal cavities can also occur due to errors in endodontic treatment. The inflammatory process begins to actively develop from the moment pathogenic microflora enters the cavity of the dental canal. As inflammation spreads, not only soft but also hard tissues are destroyed; a granuloma can form, and if left untreated, a cyst.
IMPORTANT: The process of cyst formation can be asymptomatic, but the formation can grow to significant and dangerous sizes and lead to various types of pathologies, including deformation of the jaw joint.
Why does periodontitis start?
- As we have already noted, most often periodontitis is a consequence of untreated or poorly treated caries and pulpitis.
There may also be other reasons:
- Mechanical trauma and damage to the pulp, in which inflammation develops over time.
- As a complication of periodontal diseases.
- As a complication of rhinitis, sinusitis, osteomyelitis.
- As a consequence of weakening of the body, vitamin deficiency.
- As a concomitant disease with diabetes mellitus.
- As a result of poor oral hygiene and the presence of tartar in the cervical area.
Retrograde periodontitis
This form of the disease is quite rare. Periodontitis of this form begins to develop against the background of infection penetration into the periodontium through the blood flow or lymph flow.
Traumatic periodontitis
Periodontitis of traumatic origin appears against the background of trauma, when a person receives a sufficiently severe bruise. Some medical errors made during dental treatment can lead to traumatic periodontitis:
- A small piece of an instrument that was “forgotten” after treatment in the cavity of the dental canals;
- Re-filling of the dental canal, which consists of excessive filling of filling material, which ultimately protrudes beyond the apical part of the tooth root;
- Incorrectly restored natural tooth crown, prosthesis, which constantly injure the tissues of the oral cavity.
Toxic periodontitis
This form of periodontitis usually occurs after poorly treated caries, and can occur due to tissue irritation caused by certain medications.
Each form of periodontitis has its own symptoms, but inflammation in the periodontium can also be determined by some general signs:
- Pulsating and clearly localized pain, the intensity of which gradually increases. The pain impulse intensifies at the slightest attempt to touch the teeth, during the period of their closure, while eating;
- The appearance of elevated body temperature due to toothache;
- Feeling of fullness in the area of the inflammatory process;
- Swelling of soft tissues.
IMPORTANT: Severe symptoms during the development of periodontitis are not present in all cases. Some phases of the disease can occur without the slightest external signs at all, or the person feels slight discomfort, which he mistakes for ordinary caries. Professional dental examinations, which are recommended to be carried out at least once every six months, will help to identify periodontitis in a timely manner for treatment.
Signs
Clinical manifestations of periodontal inflammation depend on the form of the disease.
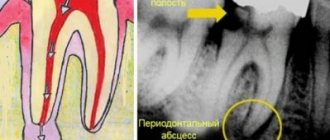
In the acute course, the symptoms are pronounced, often accompanied by the formation of a painful abscess on the gum, gumboil (deeply located abscess with intense swelling of the soft tissues of the gums and face), increased body temperature, etc. Acute inflammation can occur in two forms:
- Serous periodontitis occurs without the formation of a purulent cavity. Accompanied by constant aching pain that does not intensify when touching a tooth or biting food.
- Purulent periodontitis is accompanied by the formation of an abscess. Accompanied by sharp, bursting or throbbing pain, the intensity of which may vary. Flux is noticeable on the gum near the diseased tooth, and the soft tissues of the face on the affected side swell. The mobility of the tooth is increased, the pain intensifies when biting and touching the tooth.
In the chronic form, periodontitis is not as severe as acute periodontitis. There are three forms of the disease:
- Fibrous , the symptoms of which are sluggish inflammation without the formation of an abscess and fistulas. Pain with this form rarely occurs. An external sign is a change in the color of the enamel to gray, a change in its transparency. Signs of inflammation are visible only on x-rays.
- Granulomatous , the symptoms of which are periodic formation of an abscess. As it “ripens,” a duct opens on the gum, from which purulent contents pour out. Such ducts can form permanent non-healing fistulas. On x-rays, this form of periodontitis looks like a lesion with a diameter of up to 5 mm at the root apex.
- Granulating , the symptoms of which are chronic toothache, aggravated by biting hard, hot or cold food with a sore tooth. The gums near the tooth are constantly swollen and hyperemic. The opening of the fistula can open both on the oral mucosa and on the skin of the face.
Symptoms of any form of periodontitis tend to subside when the purulent cavity is cleared of its contents.
It is important to know! The main difference between periodontitis and pulpitis is the nature of the pain. With pulpitis, it is acute, painful, reminiscent of electric discharges, intensifying when the diseased tooth comes into contact with solid food particles, hot or cold air.
Treatment methods for periodontitis
The treatment method for periodontitis will be selected based on the characteristics of the clinical case. Methods that are used to treat inflammation in the periodontium can be divided into two groups - conservative and surgical. However, the goal of any treatment method for periodontitis will be to obtain the following results: elimination of all tissues that are affected by the infectious process, elimination of inflammation, restoration of healthy tissue, as well as restoration of the aesthetics and functional qualities of the dental unit.
To accurately diagnose, determine the form of periodontitis and select the optimal treatment method, a number of measures are carried out: a thorough examination of the patient’s oral cavity, radiography, CT, OPTG.
Forms and types of periodontitis disease
Periodontitis is the fourth stage from the onset of caries formation. The process looks like this:
- First, hard tissues are affected by caries;
- Further, in the absence of timely treatment, superficial caries turns into deep caries, the destruction becomes more extensive;
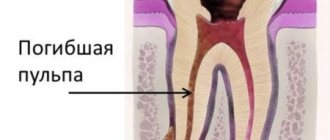
- After this, pulpitis develops - inflammation of the internal tissues (pulp);
- In the absence of qualified treatment for pulpitis, the pathology gradually turns into periodontitis, inflammation of the canals and periodontal tissues.
Therapeutic treatment of periodontitis: features and key stages
Therapeutic treatment of periodontitis is a complex, lengthy process and associated with certain difficulties. In particular, a fairly large amount of time is required to restore periodontal tissues damaged by inflammation; competent and high-quality treatment of dental canals will not be easy.
The complex of therapeutic measures for the treatment of periodontitis includes the following procedures:
- Drilling the diseased tooth to gain access to the canals;
- Work on expanding channels to a certain size, allowing for their high-quality processing;
- Painstaking cleaning of the canals from damaged and destroyed tissues;
- Flushing the canal cavity with antiseptic agents;
- Placement of antibiotic-impregnated linings into the tooth canals;
- Permanent canal filling;
- Restoration of the natural tooth crown.
Treatment of periodontitis may require repeated changes of medications in the canals, and therefore the patient is given a temporary filling for this period. After the inflammatory process can be completely eliminated, the tooth canals are filled with gutta-percha and a permanent photopolymer filling is placed on the tooth.
IMPORTANT: The more stages there are in the therapeutic treatment of periodontitis, the higher the price of the service as a whole will be.
When carrying out filling, it is extremely important to achieve complete sealing of the dental canals and all branches coming from them. After endodontic treatment of periodontitis, the doctor may additionally prescribe a number of medications for the patient to take that will help accelerate tissue recovery. Endodontic treatment of periodontitis can be supplemented by a number of physiotherapeutic procedures:
- UHF;
- Laser and magnetic therapy;
- Ozone therapy.
The need for additional physiotherapeutic procedures is determined by the dentist when drawing up a plan for the therapeutic treatment of periodontitis and based on the diagnostics performed and the characteristics of the clinical case.
What antibiotics are used?
What antibiotics are used?
To suppress pathogenic microorganisms, the following drugs are prescribed:
- "Lincomycin", "Doxycycline";
- "Tetracycline", "Amoxiclav";
- "Ciprofloxacin", "Azithromycin";
- "Erythromycin", "Metronidazole";
- "Ofloxacin", "Cifrofloxan".
Also, antiseptics “Biseptol”, “Chlorhexidine”, “Biomycin”, “Povidone-iodine”, sodium hypochloride, penicillin group drugs “Clavulanate”, “Sulbactam” have a negative effect on bacteria.
During the treatment process, local antibacterial agents are used, which are placed into the affected cavity after cleaning. Often, along with antibiotics, the doctor prescribes antihistamines to reduce reactions from the immune system. The course of administration is 5-7 days, it cannot be interrupted, otherwise the drugs will stop working. Important! Tetracycline group drugs do not enter the bloodstream, so they can only have a local effect on microorganisms.
Operative (surgical) treatment of periodontitis
Surgical techniques for the treatment of periodontitis are used if conservative therapy turns out to be ineffective or initially inapplicable due to clinical reasons. In 90% of cases, doctors try to perform tooth-preserving operations, that is, resort to a type of intervention that will eliminate inflammation, but at the same time preserve the dental unit. These types of interventions in the treatment of periodontitis include:
- Resection of the root apex. It is indicated for use when cysts and granulomas are identified during diagnostic procedures. The essence of the operation is to remove all infected tissues along with the apical part of the tooth root;
- Cystectomy. During this type of intervention in the treatment of periodontitis, the formed cyst or granuloma is removed, and the apical part of the root is excised, in which inflammation has caused pathological tissue changes.
After the operations, treatment and hermetically sealed dental canals are also carried out.
Another surgical method for treating periodontitis is an operation to amputate the apex of the tooth root. But it is possible only on multi-rooted teeth and taking into account the healthy state of the other roots of the dental unit. During intervention for the treatment of periodontitis, the crown part of the tooth can be preserved completely or partially removed. In our dental clinic in St. Petersburg you can receive services for safe and painless treatment of periodontitis. At all stages of the treatment process, dental specialists will use ultra-modern dental techniques and instruments to ensure the effectiveness of the treatment as a whole and guarantee the absence of complications.
Periodontitis in children: treatment
Treatment of periodontitis in primary teeth is not an easy task, which requires the dentist to have great skill in performing manipulations and, more importantly, making the right and consistent decisions. The choice of adequate treatment depends on the accuracy of the assessment of the condition of the tooth.
Milk teeth affected by periodontitis must be removed in a number of cases: for example, if less than two years remain before their natural loss or if the tooth has acquired noticeable mobility as a result of the disease. The tooth is also removed if most of its root is affected by the pathological process, and if the patient’s history contains references to previous exacerbations of the chronic inflammatory process. A tooth that does not respond to treatment can become a constant source of infection, which poses a significant danger - especially if the patient's immune status is reduced as a result of illness or other factors.
Unfortunately, a simple examination and even instrumental diagnostics do not always provide accurate information about the condition of the tooth and surrounding tissues. A small carious cavity can cause extensive damage to the root and periosteum. However, in many cases, periodontitis in children can be asymptomatic. For this reason, an obligatory component of treatment is to conduct X-ray examinations at various stages - to monitor the condition of the tooth and the effectiveness of the manipulations performed.
Sources:
- Prevention of recurrence of localized periodontitis in young A.K. YORDANISHVILI, Doctor of Medical Sciences, Professor, North-Western State Medical University named after. I.I. Mechnikov, Military Medical Academy named after. CM. Kirov, International Academy of Sciences of Ecology, Human Safety and Nature.
- The role of anti-inflammatory rinse in the treatment of periodontal diseases (L.Yu. Orekhova, A.A. Leontyev, S.B. Ulitovsky) L.Yu. OREKHOVA, Doctor of Medical Sciences, Prof., Head of Department; A.A. LEONTIEV, dentist; S.B. ULITOVSKY, Doctor of Medical Sciences, Prof. Department of Therapeutic Dentistry of St. Petersburg State Medical University named after. acad. I. P. Pavlova
Features of the treatment of periodontitis in teeth with previously treated canals
Retreatment of tooth canals with periodontitis is an extremely difficult undertaking, during which the dentist will have to thoroughly clean the cavities from filling material. Only a truly competent and experienced specialist can perform such work in the treatment of periodontitis, because in the course of it it will be necessary to use different methods of cleaning the canals (using specialized reagents and files) and act in fact “blindly”.
After the tooth canals are completely freed from gutta-percha, they need to be thoroughly sanitized. At this stage of treatment of periodontitis, the care and literacy of the dentist are also important, because sanitary treatment of the canal cavities should ensure the complete exclusion of recurrence of inflammation in the future.
Typically, the canals for periodontitis are washed with a specialized solution, after which the doctor places medicine in their cavities and closes the tooth with a temporary filling. In the treatment of periodontitis, a pause is made, which is necessary for the complete cessation of the inflammatory process and the beginning of regeneration of tooth tissue. As soon as the desired effect in the treatment of periodontitis is achieved, secondary permanent filling of the canals and restoration of the tooth crown with a photopolymer filling are performed.
Contraindications and side effects of antibiotics for periodontitis
Depending on the type of drug, contraindications for use are as follows:
- pregnancy and lactation;
- liver and kidney failure;
- epilepsy, lymphocytic leukemia, leukopenia;
- intolerance to the components of the drug;
- severe heart pathologies;
- age (certain products should not be taken by children or elderly people);
- porphyrin disease;
- Infectious mononucleosis.
Contraindications and side effects
Any antibiotics for periodontitis should be taken with caution by those who have problems with the gastrointestinal tract, as well as when using anticoagulants at the same time.
During the course you should not drink alcohol, since many drugs that are incompatible with alcohol can cause a severe reaction. Important !
Before treating periodontitis with antimicrobial agents, the patient must inform the doctor about his state of health. In general, antibacterial medications for periodontitis are well tolerated. However, you should stop using it and consult a doctor if the following signs appear:
- nausea, vomiting, diarrhea;
- dizziness or headache;
- soreness in the stomach;
- itching and skin rashes like urticaria;
- overexcitation, insomnia, anxiety;
- swelling of the face, lips, eyelids;
- shortness of breath, rapid heartbeat.
In severe cases, convulsions, loss of consciousness or fainting, Stevens-Johnson syndrome, and hematuria may occur. You also need to warn the doctor if the patient is taking other medications, since not all are compatible with antibiotics.
If antibiotic therapy is prescribed, the medications must be taken carefully, at the same time, in the strict dosage prescribed by the doctor. It is prohibited to independently increase or decrease the dose or replace the drug - this leads to resistance of microorganisms to the drug. You should also carefully observe oral hygiene, and after treatment, undergo a preventive examination by a dentist.
Traditional medicine: can its recipes help with periodontitis?
It is important to understand that periodontitis is a serious disease that affects the entire body as a whole and is fraught with serious complications. Its treatment cannot be carried out at home, since the infectious process occurs deep in the root canals of the tooth and it is important to thoroughly clean them of all tissues affected by inflammation. Only a doctor can do this - in a clinical setting and using a specialized instrument.
Remedies from folk recipes will be absolutely useless in the fight against periodontitis and, moreover, they can aggravate your condition. For example, hot compresses for periodontitis can provoke an acceleration in the rate of spread of inflammation.
Herbal decoctions and tinctures are powerless against periodontitis. They can only temporarily make the pain less pronounced, but in this case the inflammation will actively develop, affecting an increasingly larger area of tissue. If you are bothered by even a minor toothache, a reasonable solution would be to immediately consult a dentist. Remember that it is not always possible to save a tooth with periodontitis (especially with an advanced stage of inflammation).
The goal of treatment is to get rid of the infection. To achieve this, the dentist may prescribe:
- Surgical intervention
. The dentist makes a small incision in the abscess, allowing the pus to drain, and then disinfects the area with a special solution.
- Root canal treatment
. This will help eliminate the infection and save the tooth. To do this, the dentist drills into your tooth to remove the diseased central tissue (pulp) and then removes the abscess itself. The root canals are then filled. In this case, a crown can be installed on the tooth to make it stronger, especially for teeth - molars. If you take proper care of your restored tooth, it can last you a lifetime.
- Removal
. If the affected tooth cannot be treated, the dentist will remove the tooth and then remove the abscess to get rid of the infection.
- Antibiotics
. If the infection has spread to nearby teeth, or other areas of the jaw, your dentist will likely prescribe antibiotics to stop further spread. Antibiotics may also be recommended if you have a weakened immune system.
Periodontitis treatment time
If you have been diagnosed with periodontitis, you should prepare for a lengthy treatment process. You will have to visit the dental clinic more than once, and in addition, strictly follow all the recommendations that the specialist will give you during the treatment process. Violation of medical recommendations can lead to complications that will increase the complexity and duration of periodontitis treatment. In the simplest case, when treating periodontitis, you will have to visit the dentist two or three times; treatment will be longer if it is supplemented by physical procedures and will require repeated placement of antibiotics into the tooth canals and consultation with highly specialized specialists. Remember that high-quality treatment of periodontitis will imply mandatory control photographs after each stage.
Radiography will allow you to track the positive changes achieved after certain procedures for the treatment of periodontitis, and evaluate the quality of canal filling. Only this approach guarantees a stable and positive result in the treatment of periodontitis and eliminates relapses of inflammation and complications.
Why does periodontitis occur?
The most common causes of periodontitis are the following:
- caries in an advanced stage, which was not subjected to timely treatment;
- pulpitis in an advanced stage, lack of modern treatment;
- falls or blows to the jaw;
- poor-quality root canal treatment in the past;
- an inflammatory process that develops under the crown.
At risk of periodontitis is any patient who does not seek help from the clinic in time for caries. The problem often “pops up” in patients who do not attach importance to pain, and ordinary caries over time transforms into a more global pathology of the periodontium and canals.
Periodontitis treatment price
The cost of periodontitis treatment is always calculated individually, because it consists of a number of factors. The price of the service will depend on the set of diagnostic measures that are carried out not only at the beginning of treatment, but also at its intermediate stages. The price of the service will be influenced by the form of the disease, method of treatment, additional procedures, equipment and drugs that can be used during its course.
If you want to know the price of periodontitis treatment or make an appointment with Uni Dent dentists, just dial our contact phone number!
Vivid symptoms of periodontitis
The disease periodontitis cannot be confused with anything. It is accompanied by the following symptoms:
- the patient has severe periodic aching pain in the projection of the tooth;
- there is an increase in pain at the moment of biting;
- pain during periodontitis increases when the tooth is tapped with a hard object;
- the pain worsens at night and during the cold season;
- a purulent, inflamed sac around the gum, on which a fistula with purulent contents subsequently forms;
- mobility of the affected tooth is observed;
- Gaps appear between teeth;
- with periodontitis, bleeding gums are diagnosed;
- temperature rises;
- When sick, sleep is often disturbed;
- there is general weakness.
Very often, when a patient feels pain while biting food, he begins to chew on the other side, thereby freeing the pathological tooth from the load. During this time, the acute stage gradually turns into a chronic one, and the destructive process intensifies.
Flux on the gum
First visit
The doctor prescribes general treatment for periodontitis to alleviate the symptoms of intoxication in the patient’s body caused by purulent inflammation. Treatment is carried out using the following drugs:
- non-steroidal anti-inflammatory drugs;
- antibiotics supplemented with Metronidazole;
- antihistamines.
Second visit
A second visit is usually scheduled after a few days. Here the root canals are thoroughly washed with antiseptic solutions. After this, a long-acting antiseptic drug is placed in each of the root canals, and the tooth is covered with a temporary filling.
Third visit
If the pain is reduced and there is no pus in the root canals, they are washed again and permanently filled with gutta-percha. Then, as part of the control plan, an x-ray is taken to confirm that the root canals are filled to the root apex.
Fourth visit
Finally, during the fourth and final visit, a permanent filling is placed. It is impossible to put her in the same visit when the root canals were filled!
Exacerbation of periodontitis: how does it manifest?
The chronic form of the disease may not have any symptoms for a long time, but sometimes exacerbation phases may occur.
At such moments, the disease begins to resemble the acute stage of development: the gums swell, severe pain occurs, and pus appears. When there is no more pus left in the lesion, the pain goes away and the symptoms disappear, but this does not mean that periodontitis has been cured: it has simply entered the chronic stage again. After some time, an exacerbation will occur again, accompanied by the same symptoms.
Factors such as hypothermia, various diseases, or simply a weakened immune system can provoke an exacerbation of the disease.
Systemic antibacterial therapy for odontogenic maxillary sinusitis at the present stage
A significant role in the occurrence of chronic inflammation in the maxillary sinus belongs to diseases of the teeth of the upper jaw. Odontogenic sinusitis (OG), in fact, is a complication that arises as a result of the spread of a pathological process from the periapical focus of chronic infection in the area of premolars or molars of the upper jaw (periodontitis, periostitis, osteomyelitis, suppurating radicular cysts, there are also indications of the possibility of sinusitis occurring with abscessive form of periodontitis). Patients with odontogenic sinusitis are admitted for treatment to both dental and otorhinolaryngological hospitals. According to dentists, odontogenic sinusitis is found in 12–50% of patients with chronic sinusitis. According to the observations of otorhinolaryngologists, the frequency of odontogenic sinusitis ranges on average from 2 to 25%, with its open (perforated) form being 41.2–77.2%. Such contradictory data are not due to the true ratio of odontogenic and rhinogenic sinusitis, but to the specifics of examining patients in hospitals of various profiles. Diagnosis of odontogenic sinusitis is difficult and requires synergy in the work of otorhinolaryngological and dental services. Diseases of the teeth of the upper jaw, which are practically asymptomatic, are, as a rule, not regarded as a cause of sinusitis. Unfortunately, dentists and otorhinolaryngologists often underestimate the cause-and-effect relationship between the pathology of the maxillary sinus and diseases and abnormalities in dental development, which leads to diagnostic errors and a recurrent course of the disease. Treatment of odontogenic sinusitis should be comprehensive and in all cases include sanitation of the source of infection. The difficulty of conservative treatment of odontogenic sinusitis lies in the fact that the inflammatory process in the maxillary sinus, which developed as a result of prolonged periapical inflammation of the teeth of the upper jaw, takes on a primarily chronic nature and in most cases requires surgical treatment, the extent of which depends on both the endoscopic picture and the functional state mucous membrane. Conservative treatment is effective only for the exudative form of inflammation. Antibacterial therapy for odontogenic maxillary sinusitis is empirical in nature and is based on data on the main pathogens and their sensitivity to antimicrobial drugs in the region. It also takes into account the fact that due to the high prevalence of microbial associations, the risk of occurrence of b-lactomase-producing strains significantly increases. In this regard, antibiotic therapy for odontogenic sinusitis comes down to a choice between protected penicillins and respiratory fluoroquinolones. The purpose of our study was to study the possibilities of increasing the effectiveness of treatment of odontogenic sinusitis. Over the past year, we observed 32 patients suffering from odontogenic sinusitis and who were undergoing inpatient treatment in the ENT department of the Moscow Clinical Hospital named after. S.P. Botkin - 13 men and 19 women (average age - 38 years). The diagnosis of odontogenic sinusitis was established on the basis of complaints, medical history, objective examination (sinusoscopy, endoscopic examination of the nasal cavity, oroscopy), and the results of X-ray examination (radiography, panoramic zonography and CT scan of the paranasal sinuses). All patients were consulted by a dentist. All patients had mild to moderate severity of the disease. The “causal” teeth were: 1st molar – 19 patients, 2nd molar – 9 patients, 2nd premolar – 4 patients. In one case, there was a combination of pathology of the second premolar and first molar (Table 1). Among the examined, 4 people had an open (perforated) form of odontogenic sinusitis: 3 – antroalveolar communication with the maxillary sinus due to the removal of the first molar, 1 – second molar (Fig. 1). The group with a closed form of odontogenic sinusitis consisted of 28 people, and in four cases the process was associated with the presence of filling material in the maxillary sinus. The exudative form was registered in 9 patients (Fig. 2). According to the results of the examination, surgical treatment was recommended for 19 patients with a closed form of odontogenic sinusitis, 14 of them refused the proposed operation. As a result of bacteriological studies, associations of anaerobes and aerobes were found in 17 patients with odontogenic sinusitis in the punctate of the maxillary sinus. Isolated cultures of aerobes and anaerobes were obtained in 3 and 7 cases, respectively. No flora growth was obtained in 5 studies (Fig. 3). Aerobic flora was represented by Streptococcus spp., Staphylococcus aureus, Haemophilus influenzae, Pseudomonas aeruginosa. Anaerobic – gram-positive cocci (Streptococcus spp.), Veillonella spp., Prevotella spp., Peptostreptococcus spp., Fusobacterium spp. (Table 2). Conservative treatment included antibacterial therapy with protected penicillins, puncture (washing) of the maxillary sinus with the introduction of saline, and local use of decongestants. All patients were consulted by a dentist; sanitation of the odontogenic source of infection was carried out on days 3–4 after the start of conservative therapy. In our work, we compared the effectiveness of systemic antibacterial therapy for odontogenic sinusitis with amoxicillin/sulbactam, which recently appeared on the Russian market, and amoxicillin/clavulanate, which has long been used in ENT practice. Both drugs belong to the group of protected penicillins. Trifamox IBL® (amoxicillin/sulbactam) is an antimicrobial agent from the penicillin group (registered in the fall of 2005 in Russia (Trifamox IBL®, Laboratorios Bago S.A., Argentina)), has a wide spectrum of bactericidal action against aerobic gram-positive bacteria (including strains producing b-lactamases): Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus saprophyticus, Streptococcus pyogenes, Streptococcus anthracis, Streptococcus pneumoniae, Streptococcus viridans, Enterococcus faecalis, Corynebacterium spp., Listeria monocytogenes; anaerobic gram-positive bacteria: Clostridium spp., Peptococcus spp., Peptostreptococcus spp.; aerobic gram-negative bacteria (including strains producing b-lactamases): Escherichia coli, Proteus mirabilis, Proteus vulgaris, Klebsiella spp., Salmonella spp., Shigella spp., Bordetella pertussis, Yersinia enterocolitica, Gardnerella vaginalis, Neisseria meningitidis, Neisseria gonorrhoeae, Moraxella catarrhalis, Haemophilus influenzae, Haemophilus ducreyi, Yersinia multocida, Campylobacter jejuni, Acinetobacter spp.; anaerobic gram-negative bacteria (including strains producing b-lactamases): Bacteroides spp., including Bacteroides fragilis. Amoxicillin acts bactericidal by inhibiting the synthesis of the bacterial wall. Sulbactam is a stable, irreversible inhibitor of b-lactamases secreted by microorganisms resistant to b-lactam antibiotics. Sulbactam expands the spectrum of activity of the drug against resistant strains, without changing the activity of amoxicillin against sensitive strains, forming complexes with penicillin-binding proteins of bacteria, and exhibits synergy when used simultaneously with b-lactam antibiotics. Sulbactam does not have its own clinically significant antibacterial activity (with the exception of Neisseriaceae and Acinetobacter). The drug is available in both tablet and injection forms, which is very convenient when carrying out step-by-step therapy. When taken orally, the drug has a large volume of distribution and reaches high concentrations in tissues and body fluids, especially in the mucous membrane of the upper respiratory tract. In terms of the rate of development of the bactericidal effect, amoxicillin/sulbactam is significantly ahead of other antibacterial drugs, since it has significantly greater resistance to changes in the pH of the solution than clavulanate or tazobactam, and from a practical point of view, this means that in the conditions of a real infectious process occurring with Due to significant variations in the acidity of the environment, sulbactam is able to penetrate tissue more actively than other b-lactamase inhibitors. In our work, patients who received only conservative treatment, depending on the antibiotic therapy performed, were divided into 2 groups (main and control), similar in gender, age and the nature of the process in the maxillary sinuses and dentofacial area. The main group included patients receiving amoxicillin/sulbactam; in the control group, antibacterial therapy was carried out with amoxicillin/clavulanate (Table 3). All patients received an antibiotic in comparable dosages to amoxicillin (500 mg x 3 times a day per os). Based on the results of the conservative treatment, a pronounced positive dynamics of the main clinical symptoms of the disease was noted by the 7th day in both groups of patients with the exudative form of odontogenic sinusitis (Fig. 4, 5). In patients with purulent polyposis lesions of the maxillary sinus who received amoxicillin/sulbactam, remission was achieved on the 8th day, and in the control group on the 9th. Antimicrobial effectiveness and high sensitivity of microorganisms to drugs are confirmed by data from microbiological studies over time. Thus, amoxicillin/sulbactam is not inferior to traditional protected penicillins, the clinical effectiveness of which has been tested by time, and also has a number of advantages: 1. Sulbactam is more resistant to changes in pH, due to which it is able to more actively penetrate into inflamed tissues. 2. Sulbactam's high tolerance to pH fluctuations allows it to be administered intramuscularly. 3. Sulbactam is more resistant to most plasmid and chromosomal type I b-lactamases. 4. Amoxicillin/sulbactam is more convenient for sequential therapy, since, in addition to oral administration, it has a form for intramuscular and intravenous administration. In conclusion, it should be noted that amoxicillin/sulbactam is an effective drug in the treatment of odontogenic sinusitis and can be recommended as initial therapy for chronic maxillary sinusitis. The optimal choice of antibacterial agents for the treatment of odontogenic processes in the maxillary sinus reduces the treatment time.
Literature 1. Anyutin R.G., Luzina V.V., Romanov I.A. Differentiated surgical treatment of odontogenic sinusitis: Mater, III Congress of the Dental Association (all-Russian) - M., 1996. 2. Pluzhnikov M.S. Conservative and surgical methods in rhinology – St.–Pb., 2005 3. Timofeev A.A. Guide to maxillofacial surgery and surgical dentistry - K., 2004. 4. Sidorenko S.V., Yakovlev S.V. Beta-lactam antibiotics. Russian Medical Journal, 1997; 5 (21): 1367–81. 5. Yakovlev S.V. Amoxicillin/sulbactam – new opportunities to overcome antibiotic resistance. Russian Medical Journal 2005, volume 13, no. 21, p. 1418–22 6. Ambler PR. The structure of beta-lactamases. Philos Trans R Soc Lond Ser B 1980;289:321–31. 7. Bush K, Jacoby GA, Medeiros AA. A functional classification scheme for beta–lactamases and its correlation with molecular structure. Antimicrob Agents Chemother 1995;39:1211–33. 8. Pensotti C. et al. Meta-analisis sobre la actividad in vitro e in vivo. Efficacia y tolerancia de la combinación amoxicillina, sulbactam en humanos. La Prensa Medica Argentina 1998;85(4):515–22.
What types of this pathology exist?
Depending on the origin, the classification of periodontitis includes:
- an infectious form that develops mainly as a complication of caries, and then pulpitis;
- traumatic periodontitis is a consequence of a strong external impact on the tooth with its damage.
According to the type of clinical course, pathology is divided into:
1. Acute form with rapid development of symptoms. It, in turn, is divided into a serous subtype - with periodically changing pain intensity; and purulent - with purulent discharge, constant severe pain, tooth mobility and a high risk of irreversible loss.
2. Chronic periodontitis of the tooth, which progresses rather slowly and sometimes has no clinical manifestations at all. This form of the disease is divided into three subtypes:
- fibrous variant - the initial stage of the disease, which is often detected by chance - on radiography for other reasons;
- granulating periodontitis - the next stage with swelling of the soft tissues of the gums, the appearance of purulent discharge, as well as constant pain;
- granulomatous periodontitis, in which purulent cysts are already formed in the thickness of the gum tissue, requiring immediate surgical removal.
The types of the disease are also divided according to the location of the inflammatory process. If the apex of the tooth root is affected, it is apical periodontitis, which in most cases becomes a complication of pulpitis. And when periodontal inflammation occurs in other parts of the tooth, a marginal form develops - its appearance is most often caused by injuries.