One of the stages of endodontic treatment of any tooth is the opening of its coronal cavity and finding the mouths of the root canals for subsequent instrumental and medicinal treatment. Traditionally, in the process of performing this manipulation, the dentist, using information about the anatomical structure of the coronal cavity of a particular tooth obtained from scientific and educational literature, visually outlines the place for preparation [1-3, 5, 9, 13-15]. By removing hard tooth tissues using turbine burs, he opens the coronal cavity and expands it to the required boundaries. As a rule, this manipulation is successful if the tooth cavity does not change its normal anatomical parameters. However, quite often situations arise when, as a result of various pathological processes (dental caries, developmental anomalies, pathological abrasion, abrasion and erosion of enamel in the neck of the tooth, etc.) or age-related changes, the coronal cavity of the tooth can significantly change in volume, contain denticles or become completely calcified [4, 8, 10, 12, 16, 17]. In this case, its detection and opening for endodontic manipulations causes considerable difficulties even for experienced specialists. Often this situation leads to serious complications: perforation of the bottom and walls of the tooth cavity, failure to find the mouths of its root canals [6-8, 11, 18-26].
Currently, in dentistry there are no methods with which it would be possible to accurately mark the individual boundaries of its cavity in three dimensions in a clinical setting on the crown of a tooth.
The purpose of this study is to develop a new method that allows, using modern computer and digital technologies, to create endodontic templates that improve the quality of endodontic treatment of teeth by visualizing the boundaries of their coronal cavities.
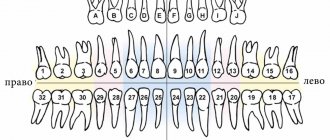
Difference between molars and premolars
The main difference between molar teeth and premolars is their location on the jaw.
Premolars are located closer to the front of the dentition, and molars are slightly moved inward. Their quantity also varies. There are always two premolars on each side of the upper and lower jaws. There can be either two or three molars. Still others are also called “wisdom teeth.” They grow later than others and often appear only at 20-25 years of age. This process is often accompanied by malaise and fever. However, not all people on earth have third ones. A certain genetic predisposition can cause the absence of wisdom teeth in the oral cavity.
Small indigenous
There are 8 of these teeth, 2 each on the right and left immediately behind the fangs in the upper and lower jaws. They refer to permanent teeth in the human oral cavity, which replace milk teeth at an early age (up to 10 years) and remain (ideally) until the end of his life. Normal service life is up to a maximum of 65 years, subject to ideal care and general genetic predisposition. However, this also applies to all other teeth.
Unlike large molars, which have 3-4 roots, premolars have:
- 2 roots at the top, and then only at the second, so-called. appromaximal
- And 1 root each for the lower ones, both vestibular and appromaximal.
That is, they sit less firmly in the gums than their “older” and “heavier” counterparts, which means they have problems more often.
The wavy, or rather lumpy, surface of the premolars crushes fragments of food that the incisors and canines have bitten off and torn from a whole piece. There are usually two tubercles: one of them, the palatal (or lingual) is directed deep, towards the pharynx, while the second, usually slightly smaller, called the buccal (or vestibular) “looks” towards the cheek.
But two tubercles are just “usually” There are three of them on premolars; as a result of the division of the tubercles into subtubercles, there are three, with the appearance of a fissure ridge , and four, when each tubercle is divided in two, and even five, with the addition of a distal apex . This provides a unique picture of dental impressions that could be used to identify each person if it were not for the simpler method of identification using fingerprints.
All organs of the oral cavity, over millions of years of evolution, have acquired such a shape and acquired such functions that the work of the internal muscular-mucosal surface of the cheek, tongue and lower jaw, which has three degrees of freedom during its movements, will automatically push large pieces onto the molars - large molars, leaving the small and medium ones “to be torn to pieces” by the premolars. That is, it turns out that if the main task of large molars is to grind food, then the premolars are to crush the pieces before grinding.
Now imagine that, due to root weakness, problems arose with premolars? Do they hurt, or have they already been removed altogether as a result of extensive caries that was not treated in time? An increased load falls on the molars, which will also begin to gradually disable them.
Features of the structure of molars
Molars have a characteristic structure. On the upper jaw they have three roots and four canals. The lower jaw has two roots and three canals. Moreover, the number of canals also differs depending on the location of the individual tooth. Thus, the first of them often have one more channel than the next two.
The main characteristic feature of this type of teeth is the area of their chewing surface. They bear the heaviest load when chewing food particles. The molars themselves also have differences among themselves, which are associated with the structure of the jaw.
Molar Differences
Often the surface of each molar tooth is shaped like a triangle. There is a certain number of tubercles on it, which take an active part in chewing food. The number of such tubercles may vary. Usually there are three, but sometimes there are more.
Such mounds are connected to each other by special ridges. On the upper and lower jaws the structure of these elements is different. In the upper dentition, the apex of the surface triangle is directed towards the tongue. This form is called a trigon. On the lower jaw, the apex of such a triangle is directed towards the cheek, which is called the trigonid. The size of the first and second types of teeth is practically the same.
Variant of the direct method modeling technique for the occlusal surface of lateral teeth
The results of studies on the structural features of the lateral teeth, and in particular their occlusal relief, formed the basis for the development of a variant of the technique for modeling their occlusal surface. The essence of the proposed technique is that the modeling of the tubercles and the relief of the occlusal surface is performed according to the “envelope” principle. In this case, the restoration is carried out with the sequential restoration of the opposite tubercles. We propose to take into account two clinical situations: a) destruction of the occlusal surface of the lateral teeth while maintaining the height of the tubercles; b) complete destruction of the occlusal surface of the lateral teeth. Restoration of the occlusal surface with its complete destruction was carried out in 11 patients on 5 premolars and 7 molars, and while maintaining the height of at least one cusp - in 9 patients on 4 premolars and 5 molars. The modeling stages are presented in diagrams (Fig. 2, 3, 6, 9) and clinical cases (Fig. 4, 7, 8). For restorations, light-curing composites Filtek P-60, Filtek Zet-250 and Filtek flow (3M/ESPE) were used in compliance with the instructions for their use.
Stages of modeling the occlusal surface of the first upper molar with its complete destruction
1. Study of interocclusal relationships, relief and structural features of the “oblique ridge”.
Before starting restoration, for a more detailed study of the occlusal relationships between the dentition, and in particular between a tooth with a destroyed occlusal surface and antagonists, it is advisable to take impressions and make diagnostic models from high-strength plaster to prevent possible abrasion of individual relief details in the process of studying the models. Using diagnostic models, the individual characteristics of the orthognathic bite, interocclusal relationships in the area of the lateral and anterior teeth, the degree of overlap of the lower anterior teeth with the upper ones, as well as the topography of occlusal contacts are determined. Particular attention is paid to the study of occlusal relief and the structure of the “oblique ridge”. In the absence of the possibility of producing diagnostic models, the above criteria can be determined in the oral cavity. Using articulation paper (for example, Bausch), the topography of occlusal contacts on an irrationally restored occlusal surface is studied, as well as the presence or absence of vertical displacement of the teeth. In case of complete destruction of the occlusal surface, it is necessary to determine the projection of the vestibular distal (median) tubercle of the first lower molar in relation to the destroyed surface of the antagonist tooth. With the help of functional tests, the degree of disocclusion should be studied during movements of the lower jaw in the sagittal and transversal planes - as a guide to a certain relationship between the depth of overlap of teeth in the frontal area, the height of the cusps of the lateral teeth and occlusal curves. The more pronounced the frontal overlap of the teeth, the more pronounced the height of the cusps of the lateral teeth and the sharper the occlusal curves. If non-functional occlusal contacts are detected, they should be eliminated by selective grinding before starting treatment.
2. Determination of the color of the restoration using a shade scale of the composite material.
3. In the presence of a tooth defect that cannot be attributed to any of the Black classes, we followed the technique of constructing a lateral tooth, taking into account the biomimetic principle, proposed by S.V. Radlinsky. (1996, 1999, 2000). Using this technique, the restoration of lateral teeth begins with the oral and vestibular walls, then the contact surfaces are built, and the middle remains empty until all vertical walls of the crown are completely built. In this technique, the labial and oral walls act as the main positioners of the crown, which can be compared to the “marks” used to create a level when laying ceramic tiles. Thanks to the construction of “marks,” we consistently transform an arbitrary crown defect into a MOD defect—medial-occlusal-distal. With the construction of the proximal distal contact wall, the crown defect from the MOD is transferred to the MO defect—medial occlusal. At the same time, through the free central space, not filled with filling material, the light of the polymerization lamp penetrates more easily, which ensures better polymerization of the proximal walls of the restoration. Next, the medial contact wall is performed, transferring the defect to O - occlusal.
4. Modeling of the medial vestibular tubercle with preliminary determination of its height along the tooth of the opposite side of the dental arch and orientation to the height of the crown of the second premolar on the working side.
If there is no preserved height of the tubercles on both sides, restoration is carried out according to the average height of the tubercles. Since the vestibular surface of the medial tubercle is more convex than the distal one, we form it with two separate portions of material. After the first layer, we outline the longitudinal ridge and its slopes on the occlusal surface, and then complete the modeling of the vestibular surface of the tubercle at the base. For correct spatial orientation when constructing tubercles, as suggested by Vetchinkin A.V. (2002), modeling is carried out taking into account three main lines: the line connecting the tops of the vestibular tubercles, the line of the central groove of the occlusal surface and the line connecting the tops of the oral tubercles.12
5. Modeling of the vestibular distal tubercle and the formation of the vestibular groove (the border of the odontomeres) with its transfer to the occlusal surface to the center of the crown. Its depth and extent varies widely.
6. Modeling of the medial palatal tubercle and transverse enamel ridge - “oblique ridge”.
Using a separate portion of material, we form the palatal surface of the tubercle and outline its future apex so that it is in line with the top of the distal vestibular tubercle. The medial ridge is smoothly transformed into a fairly pronounced medial marginal ridge, and the distal one is connected in the central part of the chewing surface with the ridge of the longitudinal ridge of the distal vestibular tubercle. Thus, the distal surface of the “marginal ridge” is formed, which divides the occlusal surface of the crown into two unequal parts. Next, we model the ridge of the longitudinal ridge, medial and distal slope from the top of the tubercle to the center of the chewing surface. At the junction with the longitudinal ridge of the medial vestibular tubercle, a central groove is formed. The distal slope of this tubercle, through the resulting transverse groove, coinciding with the line of the largest diagonal from the vestibular-medial edge to the distal-palatal one, is connected to the medial slope of the distal vestibular tubercle.
If there is significant destruction of the palatal surface of the crown, the Carabelli tubercle is restored with a separate portion of material.
7. Modeling of the medial accessory tubercle and formation of the anterior central (triangular) fossa.
8. Modeling of the lowest distal palatine tubercle, additional distal tubercle and formation of the posterior central (triangular) fossa with the distal palatal sulcus.
9. Determination of the nature of the closure of the restored tooth with antagonist teeth, localization of occlusal contacts using articulation paper (for example, Bausch), their correction in central and functional occlusion.
10. Finishing the restoration.
Stages of modeling the occlusal surface of the first upper molar while maintaining the height of the cusps
The principles and sequence of modeling in such clinical situations follow the rules described above, taking into account the number of remaining cusps and the occlusal surface pattern characteristic of the tooth.
An example of restoration of the occlusal surface of tooth 26 while maintaining the height of the cusps
Stages of modeling the occlusal surface of the first lower molar with its complete destruction
1. Study of interocclusal relationships, relief and determination of the type of pattern on the first lower molars.
Before starting restoration, it is necessary to study the occlusal relationships between the dentition, and in particular between the first molars on the side of the affected tooth. In case of a destroyed, irrationally restored occlusal surface of a symmetrical tooth or its absence, it is necessary to determine the place of occlusal contact of the medial palatal tubercle of the upper antagonist molar. In such cases, we recommend restoring the occlusal surface of the tooth with the simplest pattern in the form of a plus sign (“+”). Normally, a pattern in the form of a “plus” sign is characterized by the presence of one central fossa, with which, in the position of central occlusion, the medial lingual cusp of the upper molar antagonist forms occlusal contact. Patterns in the form of the letter “Y” (“Y”) and the letter “X” (“X”) are characterized by the presence of a medial and distal central fossa. With these types of patterns, the medial lingual cusp forms an occlusal contact in the area of the distal fossa. It follows from this that the location of the occlusal contact formed by the medial lingual cusp can serve as a guide for optimal restoration of the destroyed chewing surface of the lower first molar to its original state. This will allow you to create more accurate occlusal intertubercular relationships and choose an individual restorative treatment plan in each clinical case. Thus, depending on the type of pattern, we will take into account their characteristic features during modeling. During the biometry of the models, the presence or absence of tooth migration and the nature of the overlap of the lower teeth with the upper ones in the frontal area were also determined.
2. Determining the color of the future restoration using the VITA Classic color shade scale.
3. Construction of the supporting parts of the crown with separate portions of restoration material and transfer of the defect from arbitrary to MOD (medial-occlusal-distal).
4. Transfer of the MOD defect to the MO (medial-occlusal). Installation of a sectional matrix and wedge to construct a proximal-distal contact point. Contact points on the lateral teeth are located closer to the vestibular surface, and the lingual proximal surfaces are turned toward the oral side. To properly construct the contact point, the wedges must be installed on the lingual side.
5. Transfer of the MO defect to O (occlusal). Installation of a sectional matrix and wedge with the construction of a proximal medial contact.
6. At this stage, regardless of the type of pattern, based on the principles of shaping tooth crowns from odontometer modules proposed by L.M. Lomiashvili, L.G. Ayupova. (2004), we begin modeling the chewing surface from the vestibular distal tubercle, which occupies the central position of the vestibular part of the molar, with a preliminary determination of the height of the crown based on a symmetrically located tooth. If there is no preserved height of the tubercles on both sides, restoration is carried out according to the average height values of the odontometer. The formation of the medial border of the vestibular surface of the tubercle should be carried out at an average distance of about 5 mm from the medial corner of the crown with an inclination towards the lingual side, leaving space for modeling the medial vestibular tubercle. We form the distal border of the tubercle at a distance of about 4 mm, leaving 2 mm for the distal tubercle, which corresponds to the average values of the mesial-distal size of the crown according to odontometry data of the permanent first molar of the mandible. In this way we simultaneously establish the boundaries of three vestibular tubercles and two sulci, of which the medial vestibular sulcus is slightly longer and more pronounced than the distal vestibular sulcus.
7. Depending on the type of pattern, with a pattern in the form of a “plus” sign, we proceed to modeling the lingual distal tubercle. This tubercle is restored higher and sharper than the distal (posterior) one. The medial border of this cusp (lingual sulcus) is formed at the level of the medial vestibular sulcus with the formation in the central part of the crown of one central fossa or common point of contact between the cusps. Next, we model the vestibular medial tubercle using sequentially separate portions of material. We model it as a more massive tubercle using existing additional anatomical landmarks - the distal vestibular and medial lingual tubercles. An additional cusp is often located between the medial vestibular and medial lingual cusps.
With a pattern in the form of the letter “X” (“X”), the lingual distal tubercle is modeled in such a way that the longitudinal ridge of this tubercle intersects diagonally the central part of the crown in the direction of the vestibular medial tubercle, where a straight line should be formed between it and the lingual distal tubercle. contact not separated by a groove. Next, we carry out sequential modeling of the vestibular and lingual medial tubercles in separate portions of material.
With a pattern in the form of the letter “Y”, the medial lingual tubercle is modeled, which, with its pronounced longitudinal ridge, connects through a short groove in the central part of the crown with the distal vestibular tubercle, dividing the occlusal surface into two parts. Next, we sequentially construct the lingual distal and vestibular medial tubercles using separate portions of material. After this, we model the lingual medial tubercle. The lingual medial tubercle is slightly higher and larger than the lingual distal one, and also higher and sharper than the medial vestibular one. The angle formed by the slopes of the tubercles facing each other is close to straight. When modeling the lingual medial tubercle, an additional guideline for the correct formation of its medial border, according to our observation, can be an imaginary line drawn from the apex of the lingual tubercle of the second premolar to the medial central fossa of the first lower molar. Next comes the modeling of the additional medial tubercle.
8. Modeling the distal cusp is the final stage in modeling the occlusal surface of the first lower molar for all three main types of pattern.
9. Determination of the nature of the closure of the restored tooth with antagonist teeth, the topography of occlusal contacts using articulating paper (for example, Bausch), their correction in central and functional occlusion.
10. Finishing the restoration. This algorithm for modeling the occlusal surface of molars, in our opinion, allows not only to most correctly restore the lost anatomical relief, but also to perform directional polymerization using diagonal positions of the light guide.
Stages of modeling the occlusal surface of the lower first molar while maintaining the height of the cusps
In such clinical situations, a tooth crown defect can be described as a MOD (medial-occlusal-distal) defect, or a MO (medial-occlusal) and OD (occlusal-distal) defect, which must be converted into an O (occlusal) defect. After preparation and isolation of the surgical field from moisture, if there is not enough space between the teeth to install a sectional matrix and restore the contact point, it is necessary to first carry out separation preparation (“wedging”) using wooden wedges that are able to adsorb moisture and increase in volume. In the future, the basic principles and sequence of modeling are based on the above rules, taking into account the amount of tissue of the preserved tubercles and the pattern of the occlusal surface characteristic of a given tooth.
Stages of modeling the occlusal surface of the second molar of the mandible with its complete destruction
The basic principles and sequence of modeling are according to the rules described above, taking into account the pattern of the occlusal surface characteristic of a given tooth.
Subsequence:
1) modeling of the lingual distal tubercle;
2) modeling of the medial vestibular tubercle;
3) modeling of the lingual medial tubercle;
4) modeling of the vestibular distal tubercle.
Discussion of the results obtained
The anatomical shape of the first molars of the upper and lower jaws is one of the most complex in the dental system, and regardless of the method used to restore the defect in the coronal part of the tooth, the key point is modeling the relief of the occlusal surface. For each structural unit of the chewing surface, nature has its own function, and the features of the anatomical and morphological structure of these structural units determine the location of the occlusal contacts that maintain the height of the bite. Thanks to this fine differentiation, the working area of the chewing surface of the teeth is significantly increased, ensuring optimal performance of the function. Therefore, the stages of modeling the occlusal surface are based on the main anatomical features of the structure of the coronal part of the premolars and molars of the upper and lower jaws. Taking this into account, it is easier to plan the sequence of stages of modeling teeth with composite materials and eliminate possible errors made in the sequence of modeling the occlusal surface in each specific clinical case. Based on the above, a variant of the technique for modeling the tubercles and the relief of the occlusal surface of the lateral teeth was developed using the “envelope” principle, when restoration is carried out with the sequential restoration of the opposing tubercles.
It has been proven that always and in all cases each force must be balanced by another, equal in magnitude and opposite in direction, at every point of the structure. This statement is true for any structures that exist in nature, regardless of their size and complexity. If this condition is not met or changes for any reason, then under the influence of the load there is an imbalance between all elements of the structure, and over time - its destruction.16 Man is part of living nature, and the dental system is a complex of interconnected and interacting structural elements , ensuring the normally harmonious function of the entire structure. Considering the function of the dentofacial system from the point of view of the above, one can be convinced of the well-known fact that chewing pressure transmitted through the teeth to the lower jaw leads to the orientation of the crossbars of the cancellous bone tissue in a certain direction, according to local stresses, along the so-called trajectories. Collectively, the path lines of counter-loads create a frame-like structure and reflect the functional activity of the mandible. From the point of view of the theory of resistance, the lower jaw is considered as a body of equal resistance. 17, 18 It becomes clear that with regard to the structural features of the dentition, the most stable occlusion will be observed when the dental cusps come into contact with the fissures of the antagonists in the central occlusion, in which the greatest forces develop and, accordingly, , a function often used during chewing.19 As Novikov V. (2001) notes, this relationship between the cusps and marginal ridges is reminiscent of “brickwork,” the principle of which is that the bricks of each upper row are laid so that each of them overlaps the seam between bricks of the bottom row, which is optimal for evenly distributing the load and ensuring effective chewing. In addition, the morphological structure of the cusps of the lateral teeth is also of no small importance for the performance of the function of the dentofacial system. As S.V. Radlinsky points out,3 each tubercle of the chewing surface is shaped like a tetrahedral pyramid, the base of which has the shape of an irregular quadrangle and is located inside the dental crown, and the triangular faces form four ribs. One of them, located on the occlusal surface of the crown, is the most important from the point of view of chewing efficiency, since at a distance of 1-2 mm from the top of the tubercles there are occlusal contact points on it, which lead to the grinding of food, and the edges of the pyramid ensure the stability of the biostructure during the function. It can be assumed that this shape of the tubercles not only provides the function of grinding and chewing food, but also makes it possible to evenly distribute occlusal pressure along the ribs of the tubercles to the base of the pyramid, the level of which is located in the equator. In this case, the ribs are not only food crushers, but also “load crushers,” preventing overload of periodontal tissue along the long axis of the tooth. This assumption is confirmed by studies conducted by Boyanov B. and Raichev L.,20 which showed that when a tooth is loaded, stress spreads along the longitudinal axes or tangentially - at contact points between antagonist teeth.
The functional features of load distribution must be taken into account when modeling the masticatory surface tubercles, since occlusal contacts during chewing, not significantly different from those during swallowing, most often occur during sliding movements in different directions and from different starting points, thus forming occlusal areas during chewing and ensuring optimal performance of the function.19 The location and number of occlusal contacts, as well as the direction of the applied force during the closure of the teeth, affect the activity of the muscles that lift the mandible.21 Violations of occlusion lead to deformation of the occlusal plane, a change in the load on the elements of the temporomandibular joints , contributing to the development of chronic microtrauma and reflexively reducing the activity of the masticatory muscles. Only in the habitual closure of the dentition, free from disturbance, is their maximum activity noted.22
It has also been established that lateral teeth with a small distance between the vestibular and lingual cusps have less favorable conditions for normal transversal occlusion, taking into account the topographic position of the antagonists and the location of the axes of the teeth.23 From this it follows that with significant destruction of the tooth crown, when the main anatomical landmarks of the occlusal surface and there is no similar tooth with preserved morphology, when modeling the average anatomical dimensions of this tooth should be taken as a basis. This is necessary for more accurate restoration of the height of the tooth crown and its correct orientation in the dentition, which prevents destruction under the influence of chewing load in various planes.
The proposed version of the technique for modeling the occlusal surface of molars is based on the anatomical features of their structure, which, in our opinion, are guidelines for restoration, and only complements the known methods. For example, Radlinsky S.V. (1999) proposes to restore the occlusal surface with separate portions of restoration material, imitating individual cusps of the tooth, which with their boundaries will form a specific fissure pattern characteristic of a given tooth.3 According to V. Novikov (2001), one should focus on the preserved cusp tops and the main formation of the masticatory surfaces should be carried out after polymerization of the restoration material with special diamond burs of various grain sizes at the stage of finishing the restoration.9 Salova A.V., Rekhachev V.M. (2004) use a clinical example to demonstrate the restoration of tooth 46 and recommend that the buccal supporting cusps be restored first, then the lingual guides, and the weakened cusps be reduced in height by 2 mm and subsequently covered with a composite.10
Compliance with all stages of working with restorative filling material in the direct technique and modeling the occlusal surface is a complex task, difficult to accomplish without the use of a rubber dam or auxiliary tools (various types of roller holders) for maximum isolation of the restored tooth from contamination with saliva, etc. On the other hand, the larger the area destruction of the occlusal surface, the more difficult it is to achieve a positive treatment result without a specific modeling algorithm. This algorithm, on the one hand, should be easy to understand and remember, and on the other hand, it should be a “flexible tool” in the hands of the dentist, which could be easily adapted to various clinical situations, and would not change in its essence. In this case, a preliminary assessment of occlusal contacts and planning of the contours of future restoration are mandatory.24
Knowledge of the topography and anatomy of the occlusal surface of the lateral teeth will help to navigate the architectural features and correctly restore the tooth crown. Irrational filling, as well as prosthetics, which disrupts the maximum intertubercular contact, can contribute to the development of structural changes in periodontal tissues, cause chronic impairment of the activity of the masticatory muscles and lead to dysfunction of the temporomandibular joints (pain, clicking, crunching, etc.).25
conclusions
1. When modeling the occlusal relief of the lateral teeth, one should be guided by their individual architecture, that is, relief patterns.
2. A method for modeling the occlusal surface of lateral teeth using the “envelope” principle has been proposed, which provides the most accurate reproduction of the occlusal architecture.
Source: radlinskiy.ru
Possible damage to small molars
Carious lesions of primary and molar teeth in children are observed quite often. This is due to the bumpiness of their surface, which can trap food particles and bacteria. Since children at an early age do not always actively and correctly brush their teeth, these residues can lead to damage to the enamel and deeper spread of caries.
Depending on the degree of damage, caries can penetrate either exclusively into the enamel, or into dentin or even cement. In the latter case, we are talking about deep caries, which often requires serious treatment or even tooth extraction.
Another variant of damage is a change in tissue structure, which may be associated with metabolic disorders in the human body or other diseases. Such a disease can also be the result of poor nutrition or constant diets, in which the body does not receive enough nutrients.
At any age, a person can experience excessive tooth wear, which leads to the destruction of enamel and can cause other serious damage. Teeth can wear down in different situations, such as:
- if a person has bad habits of grinding his teeth, etc.;
- in case of improper or insufficient nutrition;
- in the presence of diseases of the endocrine system;
- due to a genetic predisposition to enamel depletion.
All of these lesions can be the result of both an incorrect lifestyle and various diseases or heredity. Regardless of the reasons, it is necessary to begin treatment of emerging injuries immediately so as not to aggravate the process.
Replacement of primary molars with permanent permanent molars
Molars are the first permanent teeth to appear in a child's mouth. This begins around the age of five. Growth begins with the first molar tooth, which appears in a free space in the depths of the jaw, closer to the milk one that has not yet fallen out.
The second molar usually grows in at the age of 12-13 years. It also takes up free space and does not replace a baby tooth. The latter, or “wisdom teeth,” may take up to 25 years to grow or may not appear at all.
As for dairy products, they begin to fall out from the age of 9. In their place, permanent teeth grow, which occurs at approximately 10-12 years of age. Usually these are the last molars, the growth of which must wait to fill the adult dentition (not counting “wisdom teeth”).
Is it possible to loosen baby molars?
The process of tooth loss always begins with softening of its root. This occurs as the jaw grows, freeing up more space for a permanent tooth. Thus, while the baby tooth is still in the hole, the molar is already beginning to take its correct place.
In this regard, dentists categorically do not recommend deliberately loosening baby molars. If they fall out prematurely, jaw growth may be stunted. As a result, there will not be enough space for permanent teeth, and they will begin to grow crookedly, getting out of the general dentition.
Signs of imminent appearance of molars
The first signs that molars are about to appear are noticeable even before the baby teeth fall out. These include the following:
- widening of the jaw, which can be seen when gaps appear between other baby teeth;
- the appearance of sufficient free space behind the outer lateral milk teeth;
- swelling of the gums.
In this case, the temperature does not necessarily have to rise or the child’s well-being deteriorates, as was the case with the growth of baby teeth. This is why the appearance of the first molars often goes unnoticed.
Helping your child replace teeth
The process of replacing teeth often takes place without pain or discomfort. The roots of baby teeth dissolve on their own, and the dental crown falls out freely. However, there are a number of recommendations that should be followed during this period.
The main one is systematic rinsing of teeth for disinfection purposes. This is necessary in order to avoid bacteria from entering the hole that will form at the site of the falling tooth. In addition, the sharp edges of a crown that has separated from the gum may cause minor damage to soft tissue. To prevent them from becoming inflamed, it is important to exclude any infection.
If your child experiences any pain during the tooth replacement stage, you should immediately consult a doctor. Under no circumstances should pain be eliminated using improvised methods.
Molars and prevention of their loss
Molars are stronger than baby teeth. However, they need proper care to prevent their loss, because new ones will not grow in place of a lost tooth.
Prevention of molar tooth loss involves proper oral hygiene. It includes systematic brushing of teeth, use of dental floss and mouthwash. In addition, you should carefully monitor the condition of your teeth and consult a doctor if even minor damage is detected.
Proper balanced nutrition is also mandatory. Especially in childhood and adolescence, you need to ensure that your body gets enough calcium and vitamin D.
results
The use of the above research methods made it possible to develop the following algorithm of actions to achieve the goal: first of all, CBCT of the teeth of the upper or lower jaw (skeletal jaw with teeth) planned for endodontic treatment was performed. The obtained data was processed using computer viewing X-ray programs and a thorough study of the resulting digital image of the causative tooth (row of teeth) in direct and axial projections was carried out in order to detect and localize the boundaries of its coronal cavity (Fig. 1).
Rice. 1. CBCT of a skeletonized human lower jaw with teeth in axial projection. The coronal cavity of a molar is at the level of its roof.
Next, an impression was taken of the teeth requiring endodontic treatment using an impression mass and a plaster model was cast that accurately copied their crown parts. In the case of using a skeletonized jaw with teeth, this stage was skipped, taking into account the possibility of using an intraoral laser scanner in a clinical setting. The resulting model or skeletonized jaw was scanned with a 3SHAPE D900 dental scanner (3M, USA) to obtain a digital image of the crowns of the teeth under study (Fig. 2). Then, using the computer program Amira 4.1.2 (Visualization Sciences Group, Mercury Computer Systems, USA), digital images of the tooth obtained using computed tomography and scanning were combined. Then, using the computer program 3ds MAX 2009 (Autodesk, USA), a three-dimensional individual template was virtually modeled for the crown of the tooth, which had a hole strictly coinciding with the boundaries of the tooth cavity and projected onto its chewing surface (Fig. 3, 4, 6 ). Next, in the same way, a second template was modeled for the crown part of this tooth, which ensured the optimal depth of opening of the cavity. A small hole was modeled in the template, the projection of which was located within the boundaries of the tooth cavity. The template had a limiter, which was a hollow cylinder, through which a diamond bur was first introduced before contacting the coronal part of the tooth (Fig. 5, 8). It had a cylindrical shape and was covered with diamond chips only at the end of the working part (Fig. 9). When rotating and moving the bur deep into the tooth, it reached the bottom of the coronal cavity and stopped, since the bur shank rested against the limiter. Thus, the length of the limiter could be used to regulate the immersion depth of the drill.
Rice. 2. Digital image of the coronal part of the molars obtained using surface scanning. Anatomical features of the relief of the chewing surface of the teeth.
Rice. 3. The stage of virtual modeling of the endodontic template on the combined image obtained as a result of CBCT and surface scanning of the tooth. The module of the template corresponds to the volume of the coronal cavity of the mandibular molar. The lower border of the module is located at the level of the mouths of the root canals of the tooth.
Rice. 4. Modeled endodontic template, visualizing the required dimensions of the preparation of the coronal part of the tooth. The hole in the template exactly repeats the shape of the coronal cavity of the molar, projected onto its chewing surface.
Rice. 5. Endodontic template modeling stage. Formation of immersion limiters for a diamond turbine end bur designed to determine the depth of preparation of the coronal part of a molar.
Rice. 8. The shape of the endodontic template designed to visualize the depth of the coronal cavity of the molar.
Rice. 9. Endodontic template with an end bur inserted into it to determine the depth of the coronal cavity of the tooth.
The digital images of the templates were then converted by laser prototyping using a 3D printer into a product made of heavy-duty plastic.
In laboratory conditions, simulating the clinical stage of endodontic treatment of a molar, the first plastic template was placed on its coronal part and secured to it using an adhesive light polymerization system (Fig. 6, 7). Using a thin black felt-tip pen, the established contour of the tooth cavity was applied through the hole of the template onto the chewing surface of the crown of the tooth requiring endodontic treatment. We shot the first template. Then a second template was put on the same tooth and the coronal part was prepared through the hole in it with an end bur to the set depth (Fig. 8, 9). In this way, clear three-dimensional landmarks were formed for constructing optimal endodontic access. After removing the template, the tooth cavity was opened and its subsequent endodontic treatment was carried out using standard methods.
Rice. 6. Shape of the endodontic template reproduced using a 3D printer.
Rice. 7. Visualized boundaries of the coronal cavity of the lower molar after fixing the endodotic template on the teeth.
The advantages of the proposed method compared to traditional ones are: prevention of complications and errors during endodontic treatment of a tooth at the stage of opening the tooth cavity; preservation of hard dental tissues from excessive preparation in the process of searching for root canal orifices. The disadvantages of the method can be recognized as: the need for endodontic treatment of the tooth in several visits; additional costs for modeling and production of an individual template.
Maxillary premolars
The crown of the premolars on the upper dentition has a prismatic shape. The buccal and palatal bones often have a convex surface. The first and second premolars in the row also have their differences.
First premolar
The difference between the first premolar of the upper jaw is the predominance of the vestibular surface over the palatal surface. Its contact surfaces are rectangular in shape. The buccal tubercle has two distinct slopes. The root of such a tooth often has a bifurcation.
Second premolar
In such a tooth, the buccal surface usually predominates over the palatal surface, which is more rounded. In most cases, this premolar tooth has a single cone-shaped root. However, there are also cases when it has a split.