Caries is the most common oral disease. Therefore, there is a constant search for new, more durable materials and treatment methods. In order for the filling to serve for a long time and the tooth underneath it not to be destroyed, there are certain algorithms for performing treatment. One of them is the use of an alcohol adhesive protocol.
In the last 5-7 years, this method has become very popular among dentists. The first studies on this topic appeared back in 2007.
General information
What is adhesion
Adhesion is the bond of bond (dental glue) with tooth tissue (enamel and dentin).
And the filling material is already attached to the glue. Without it, it is impossible to glue the light seal. Bond is divided into 7 generations, each with its own characteristics of application and strength of adhesion to the tooth. The 4th generation is usually used in the alcohol protocol. The better the enamel and dentin are prepared, the more durable the bond and restoration will be.
Essence of the protocol
Dentin contains an enzyme that is activated when the tooth is processed. It is this that over time destroys the adhesive layer (the connection between tooth tissue and material). It can also be found in saliva and gingival fluid. The use of an alcohol adhesion protocol is aimed at neutralizing this enzyme.
If the cavity is poorly dried, the service life of the filling will be reduced. If you overdry it, too, since the glue will not penetrate well into the tooth tissue. In addition, in both cases, the patient will be bothered by severe sensitivity from cold and hot, or when biting on a tooth.
It is necessary to know the methods of the alcohol adhesive protocol and the nuances of its implementation. The survival of the restoration and the health of the tooth depend on this. Methods are divided into complete and incomplete.
The use of chlorhexidine in the adhesive protocol: literature analysis and expert opinions
The influence of chlorhexidine on the quality of the formation of an adhesive connection between the composite restoration and the treated walls of the dental cavity has been a topic of discussion and discussion among scientists and practicing dentists for many years.
This article analyzed a number of scientific articles, and also obtained the opinions of practicing dentists on the use of chlorhexidine.
The advisability of using chlorhexidine at the stage of adhesive treatment of the prepared cavity is justified by the possibility of inactivating matrix metalproteinase (MMP) enzymes, which have collagenolytic, gelatinolitic effects and enamel-lysis activity. Given the corresponding activity of matrix metalproteinases, the connection between their action and the progressive degradation of the interface between the tooth structure and the composite material becomes quite logical.
Photo 1. The mechanism of formation of an adhesive connection, which is degraded over time under the action of metalproteinases.
Photo 2. Schematic illustration of the degradation of the bonding layer.
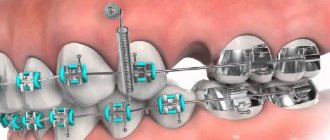
This process is critical in the area of the intermediate bond layer and adhesive-infiltrated dentin, since it is this area that provides the chemical retention of the filling. The action of metalproteinases is manifested precisely by insufficient infiltration of the enamel and dentin structures with the proper layer of bond: under such conditions, part of the fibrin fibers of dentin remains exposed, thus providing the opportunity for MMP to penetrate into the gap between the composite and the tooth, where enzymes begin to gradually “pull apart” the adhesive layer. In addition to the dentinal tubules, MMPs can be found in fairly large quantities in saliva and gingival fluid, where they take part in the fermentation process, as well as tissue remodeling, proliferation, migration and differentiation of cells, and apoptosis.
However, the very use of chlorhexidine already raises a number of specific questions: how to use it? according to what protocol? is it needed at all? And is this approach demonstrably effective?
It is known that the use of chlorhexidine at the stages of adhesive processing is possible using several protocols:
- First, treatment of the cavity with chlorhexidine, then washing, etching and subsequent application of adhesive;
- Using chlorhexidine before etching without additional cavity rinsing;
- The use of chlorhexidine after etching followed by rinsing the cavity;
- Using chlorhexidine as a solution for rinsing the cavity after the etching procedure.
"Staging" and temporary exposure to the use of chlorhexidine
Japanese researchers Chang and Shin argue that the best effect from the use of chlorhexidine can be achieved by using it strictly after etching the cavity as an additional treatment before applying the adhesive. Already other Japanese under the leadership of Hyun-Jung Kang have proven that the exposure time of chlorhexidine, in fact, does not play an important role in ensuring the appropriate effect of using the solution. Testing by researchers of temporary exposures of 5, 15, 20 and 60 seconds after etching and subsequent washing of the dentin surface did not reveal any difference in the effect obtained, thus, 5 seconds of chlorhexidine is sufficient to provide the desired effect of the adhesive bond.
Expert opinions regarding the use of chlorhexidine also differ.
So, Olga Tkachuk , for example, does not use the solution in her work: “I do not use chlorhexidine treatment of the carious cavity in my work at any stage of treatment. It is impossible to achieve complete sterility in a carious cavity, and I consider the effect of chlorhexidine in increasing the durability of the adhesive layer to be insufficiently proven.”
Others argue that the use of chlorhexidine is inappropriate due to the lack of appropriate recommendations in the instructions of manufacturers of adhesive systems.
For example, Alexey Sazonov opposes the use of chlorhexidine in general, since, in his opinion, “MMPs are needed for the transition of altered dentin to sclerotic types.”
Some practicing dentists, in particular Roman Vasiliadis , express their opinion more than categorically in their answers to such questions: “I can answer right away, I don’t use it, I conducted experiments, but refused to use this solution...”.
It should be noted that the use of chlorhexidine has also found its supporters, among whom is Alexander Grigoriev : “I use a solution of chlorhexidine both as an antiseptic and as an MMP inhibitor in the total etching technique.”
Or, for example, Roman Aliyev Fr.
Denis Krutikov took neutrality on this issue , saying: “I don’t use HG. But I’m neither for nor against, because it is needed in some cases.”
Chlorhexidine concentration: what should it be?
Be that as it may, but if there are not so many questions with the stage and time exposure of the use of chlorhexidine, then with the required concentration everything is much more complicated. Preliminary laboratory studies have demonstrated that chlorhexidine concentrations of 0.001% are sufficient to inactivate MMP-2, 0.02% for MMP-8, and 0.002% for MMP-9. However, how effective such low concentrations of the drug are for the entire complex of metalproteinases has not yet been determined. In addition, at such concentrations of chlorhexidine, it is impossible to achieve its retention interaction with dentin hydroxyapatite, while the use of higher concentrations of the solution (up to 2%) allows for prolonged persistence of the components of chlorhexidine in the tooth structure.
Photo 3. Commercially available forms of chlorhexidine in different concentrations.
American researchers also agreed that the use of higher concentrations of chlorhexidine in the range of 0.1-1.0% provides more successful restoration results in terms of guaranteeing its long-term functioning. With a similar approach to cavity preparation, but using a 0.05% concentration of chloroxydine, no changes in bond strength or longevity of the filling were observed. At the same time, American scientists have clearly determined that such a protocol is effective (or ineffective depending on the concentration) only in cases of using Clearfil SE Bond, thus, having already drawn attention not only to the inactivation effect of chlorhexidine relative to metalproteinases, but also to the specificity its interactions with various bonding systems.
In parallel, ongoing research by Peter C. Moon also argued the advisability of using only 2% chlorhexidine at the stage of etching and washing off the etchant agent, which, according to the author, is currently the only method that provides demonstrably more reliable results for the functioning of composite restorations. This opinion is no different from the argumentation of Chang and Shin, already mentioned above regarding the stages of using the solution.
But let’s return to the issue mentioned by the Americans: as it turned out, the effectiveness of using chlorhexidine also depends on the adhesive system with which it is used.
On this occasion Denis Krutikov , answering the question “Does the possibility of using chlorhexidine depend on the generation of the bond used?”, Fr.
Edson Alves de Campos et al found that the use of chlorhexidine concentrations above 0.12% with self-etching adhesive systems is generally undesirable because such solution concentrations tend to reduce the adhesive bond strength in the immediate follow-up period. On the other hand, the same researchers found that the use of 2% chlorhexidine with “etch-and-rinse” adhesive systems does not cause an immediate decrease in the strength of the adhesive bond, but rather provides longer retention of an adequate bonding interface. When testing Clearfil SE Bond (SE) and Clearfil Protect Bond (PB), Fereshteh S. and colleagues found that chlorhexidine, although it has a positive effect on maintaining proper adhesive bond in the long term, but provokes its decrease immediately after polymerization, thus increasing the risk of developing possible complications specifically with these two adhesives.
Ricardo de Sousa Vieira noticed another interesting fact: treating the cavity surface with a commercially available 2% chlorhexidine solution before etching the dentin also negatively affects the formation of the adhesive bond when using the Single Bond bonding system. The attentive reader will note that Single Bond precisely belongs to the group of self-etching adhesives that Edson Alves de Campos warned about. A study by Deng D et al found that chlorhexidine provided better bond retention when using Single-Bond (but in an etch-and-rinse protocol), while it had no effect when using self-etching G-Bond, which was applied according to the manufacturer's protocol. But the Brazilians not only confirmed this fact, but went even further and proved that the use of an etching gel containing 2% chlorhexidine also does not provide a better effect compared to the classic protocol for etching tooth dentin without the use of any disinfectants.
Stanislawczuk R. and colleagues can argue with the latter judgment, who, in order to avoid direct interaction between chlorhexidine and the bond components, proposed the use of a special acid agent containing 2% chlorhexidine. When testing this approach with two adhesive systems, Prime & Bond NT (PB) and Adper Single Bond 2 (SB), researchers noted positive effects on both systems over a two-year follow-up. Similar results were obtained by Loguercio AD, who tested, in addition to the corresponding chlorhexidine-containing acid, also the use of a water-soluble chlorhexidine-containing primer. Both preparations provided long-term stability of the composite-dentin joint during observation.
For a similar purpose, Abu Nawareg M (2016) and colleagues conducted a study that compared the effect of using conventional chlorhexidine digluconate and modified chlorhexidine methacrylate. It turned out that both forms of chlorhexidine have a positive effect on the duration of the restoration’s functioning, but, given the specific chemical structure of chlorhexidine methacrylate, it provides a longer effect, since it copolymerizes with the monomers of the composite, thus guaranteeing long-term retention of the active substance. In terms of chlorhexidine content, Peak Universal Bond is universal, which already contains 0.2% chlorhexidine.
Photo 4. Peak Universal Bond is an adhesive that contains 0.2% chlorhexidine.
But a comparative study by Sabatini S. did not reveal a difference in the effectiveness of the use of Peak Universal Bond and the isolated use of chlorhexidine as a compounding agent at the stages of cavity adhesive treatment. Similar concentrations of chlorhexidine (0.2%) are also found in such modified forms of bonds as XP Bond [XP] and Ambar {AM}. Moreover, the presence of exactly this concentration of chlorhexidine in the adhesive composition does not demonstrably affect the physical and mechanical properties of the bonding system.
An alternative to chlorhexidine, according to experts , is the following:
- ready-made solutions for dentists with an appropriate cost (Alexey Soshnikov) ;
- ammonium compounds from a series of antiseptics (Alexey Sazonov) ;
- only preparation and rinsing with distilled water (Olga Tkachuk) ;
- acid with benzalkonium chloride (Alexander Grigoriev) .
Use of chlorhexidine in combination with other agents
Separate European studies have demonstrated the effectiveness of the simultaneous use of chlorhexidine and ethanol during the adhesive preparation stages of the cavity (thereby reducing the level of microleakage, which was re-evaluated 12 months after the procedure). Other studies, on the contrary, have demonstrated the lack of a complex effect of using chlorhexidine and ethanol compared to the isolated use of ethanol alone, although the facts obtained are very, very contradictory with a huge amount of sufficiently confirmed data. In 2012, Lenzi TL and colleagues demonstrated that chlorhexidine does not provide immediate improvement in adhesive bond strength to both healthy and caries-affected hard tissue structures of primary and permanent teeth. In other words, if the issue of ensuring long-term stability of the adhesive layer with the help of chlorhexidine can still be considered more or less resolved, then the aspect of the formation of an immediate adhesive bond and the risks of its disruption remains open to debate. If we consider the specifics of the formation of a bond between the bond and the hard tissues of the tooth under the conditions of treating the latter with chlorhexidine, then the same Brazilians came to the conclusion that in the early period of observation the level of dentin demineralization is the most critical and influential factor regarding the formation of an adequate bonding interface, at least , when using self-etch adhesive systems. Thus, in cases of insufficient dentin mineralization, regardless of the concentration of chlorhexidine used, the latter will not be able to influence the stabilization of the bond between the composite and hard dental tissues.
The question also remains interesting: how to check whether the cavity was treated correctly with chlorhexidine? Alexey Soshnikov adheres to a simple method: “There should be enough of it, there is no need to save it. Moreover, the solution prepared in a pharmacy is inexpensive.”
Olga Tkachuk states the following: “I only allow antiseptic treatment of the cavity with chlorhexidine before all stages of adhesive preparation with rinsing with distilled water and drying. However, it has been proven that in a sealed cavity, bacteria die or become inactive, which defeats the purpose of attempting to sterilize the cavity.”
Alexander Grigoriev answered this question like this: “There are no such signs: simply following the adhesive (drying) technique will be the criterion for a correctly performed procedure. After etching and washing off the acid for 2 times longer than etching, the cavity is filled with CG solution, left for 15-30 seconds, and then the wet drying procedure.”
Thus, before using chlorhexidine, the doctor at the stage of adhesive treatment of the dental cavity needs to familiarize himself with the results of relevant studies already available online in order to determine the possibility of a promising complex use of this solution together with the appropriate adhesive, without violating the manufacturer’s recommendations.
In addition, within the framework of the topic under discussion, the problems of which require ambiguous answers, the exchange of experience and knowledge is of some value. In order to discuss current issues of using chlorhexidine in an adhesive protocol and determine the promising capabilities of this solution, a joint discussion of this topic in the comments will be very valuable and useful.
Share your experience and practical advice in the comments - because only together we can discuss the nuances and weigh the pros and cons regarding the use of chlorhexidine.
Stages
For high-quality restoration, the working field is isolated from saliva with a rubber dam or other system. Protocol:
- Etching of enamel - 10-15 seconds, dentin - 3-5 seconds.
- Washing off the acid with a stream of water or a water-air spray. Must be equal to or greater than the etching time. By no means less. Do not dry.
- Rinsing the cavity with alcohol (from 70%, preferably 95%) or an alcohol solution of Chlorhexidine from a syringe for 60 seconds. You can rinse one at a time - first with Chlorhexidine, then with alcohol. Dry slightly, you can remove excess moisture with paper pins.
- For 5th generation bond and higher: apply adhesive, rub it into the cavity for 10-15 seconds. Dry slightly. Then a second layer is applied (the same as the first) and blown until the “waves” disappear. For 4th generation bond: apply primer at least 2 times, each layer must be rubbed in and inflated! Apply the bond in the same way.
- Applying a thin layer of flowable composite to the bottom of the cavity.
- Polymerization according to the instructions for the adhesive.
During the adhesive preparation process, the cavity must be constantly moistened! Do not overdry fabrics.
What is an alcohol protocol?
A protocol in medicine is recommendations for treatment developed by scientific and medical communities. These recommendations are scientifically based, within the framework of evidence-based medicine, practice-oriented guidelines for action.
The alcohol protocol is a recommendation for the use of an alcohol solution, which is necessary for dentin hybridization. Alcohol is used to inhibit metalloproteinase enzymes, which are formed in dentin under the influence of phosphoric acid.
Opinion of Alexey Olegovich Sazonov
In the video, Sazonov’s technique:
Alexey Olegovich Sazonov graduated from MGMSU - Moscow State Medical and Dental University named after. A.I. Evdokimov, majoring in Dentistry. Doctor - dentist-therapist, orthopedist, chief physician of the Art-pro clinic. Work experience - 19 years.
He does not use Chlorhexidine, because he considers its action useless: “MMPs are needed for the transition of altered dentin to sclerotic types.” This is necessary in the presence of deep caries, to strengthen the affected but healthy tissues. Chlorhexidine, according to the doctor, can prevent this. Sazonov uses 95% alcohol. For different generations of adhesives, the operating algorithms are different. More often, Alexey Olegovich adheres to the following sequence (4th generation: acid, primer, adhesive):
- Selective dynamic etching of enamel 15 sec with phosphoric acid, dentin 3-5 sec.
- Rinse with water, DO NOT dry, add 95% alcohol (water from a syringe for 30 seconds), do not dry.
- Rub in the primer 3 times, dry well (1 time).
- Rub in the adhesive and inflate.
- Apply the fluid-flowing composite in a thin layer.
- Polymerization - 10 sec.
There are many articles and studies on this topic, they often contradict each other. First of all, you need to understand the causes of the problems, and not blindly accept recommendations on faith. The relevance of the alcohol adhesive protocol in dentistry will only be confirmed by the long-term durability of restorations.
Types of adhesive systems.
Now in practice there are a couple of types of such systems, which must be included:
- Special system for enamel. It is necessarily based on hydrophobic liquids and monomers of materials. This involves the use of micromechanical adhesion. Such a system will not provide adhesion to dentin. The latter is isolated from the toxic effects of the insulating gasket. Otherwise, you need to use the system below. In this case, chemical polymerization is used. The workflow includes the following stages as follows:
— etching of enamel for up to 30 seconds. (37% acid solution); — removal of etching gel from the water mass up to 30 seconds; — drying of enamel and systemic control of quality characteristics; — mixing in equal proportions the components of such a system; — using the system using applicators; - use of a jet of air to intelligently distribute the system; — use of composite materials.
- Special system for dentin. The use of such materials simplifies and improves adhesion. Therefore, let’s move on to consider the types of generations of adhesives.